Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Breast imaging is the field of radiology dedicated to the detection and management of breast abnormalities, especially breast cancer. Breast cancer is second only to skin cancer as the most common cancer diagnosed in women and is the second leading cause of cancer death in women, behind lung cancer.
The lifetime risk of breast cancer is defined as the likelihood that a woman will develop cancer over an 80-year life span. For example, a woman with no known risk factors has a lifetime risk of developing breast cancer of approximately 12%.
Risk factors for breast cancer include early menarche, late menopause, and other factors, some of which are shown in Table 29.1 and Box 29.1 . Certain histopathologic findings also increase the risk of breast cancer.
| Category | Percent Risk | Factors Affecting Risk |
|---|---|---|
| Average | <15% | No known risk factors |
| Intermediate | 15%–25% | Strong family history of breast cancer, but no BRCA mutation; those with a mutation in CHEK2 ( Box 29.1 ); those in the highest category of mammographic density; and those with a past history of lobular carcinoma in situ or atypical hyperplasia |
| High | >20% | BRCA mutation carriers and their untested first-degree relatives, such as a sister, mother, or daughter; women with histories of chest radiation between the ages of 10 and 30; a personal history of invasive breast cancer or ductal carcinoma in situ (DCIS) |
The most common cause of hereditary breast cancer is an inherited mutation damaging the BRCA1 or BRCA2 gene. BRCA1 and BRCA2 are human genes that are tumor suppressors . BRCA is an abbreviation for BR east CA ncer.
Mutations in these genes correlate with an increased risk of breast cancer. If BRCA1 or BRCA2 are themselves damaged by a mutation, damaged DNA is not properly repaired.
Females with a harmful variant of the BRCA1 or BRCA2 gene have up to an 80% risk of developing breast cancer by age 90. The increased risk of developing ovarian cancer is about 55% for females with BRCA1 mutations and about 25% for females with BRCA2 mutations.
CHEK2 (checkpoint kinase 2) is a tumor suppressor gene that encodes the protein CHK2. Inherited mutations in the CHEK2 gene have been linked to certain cases of breast cancer.
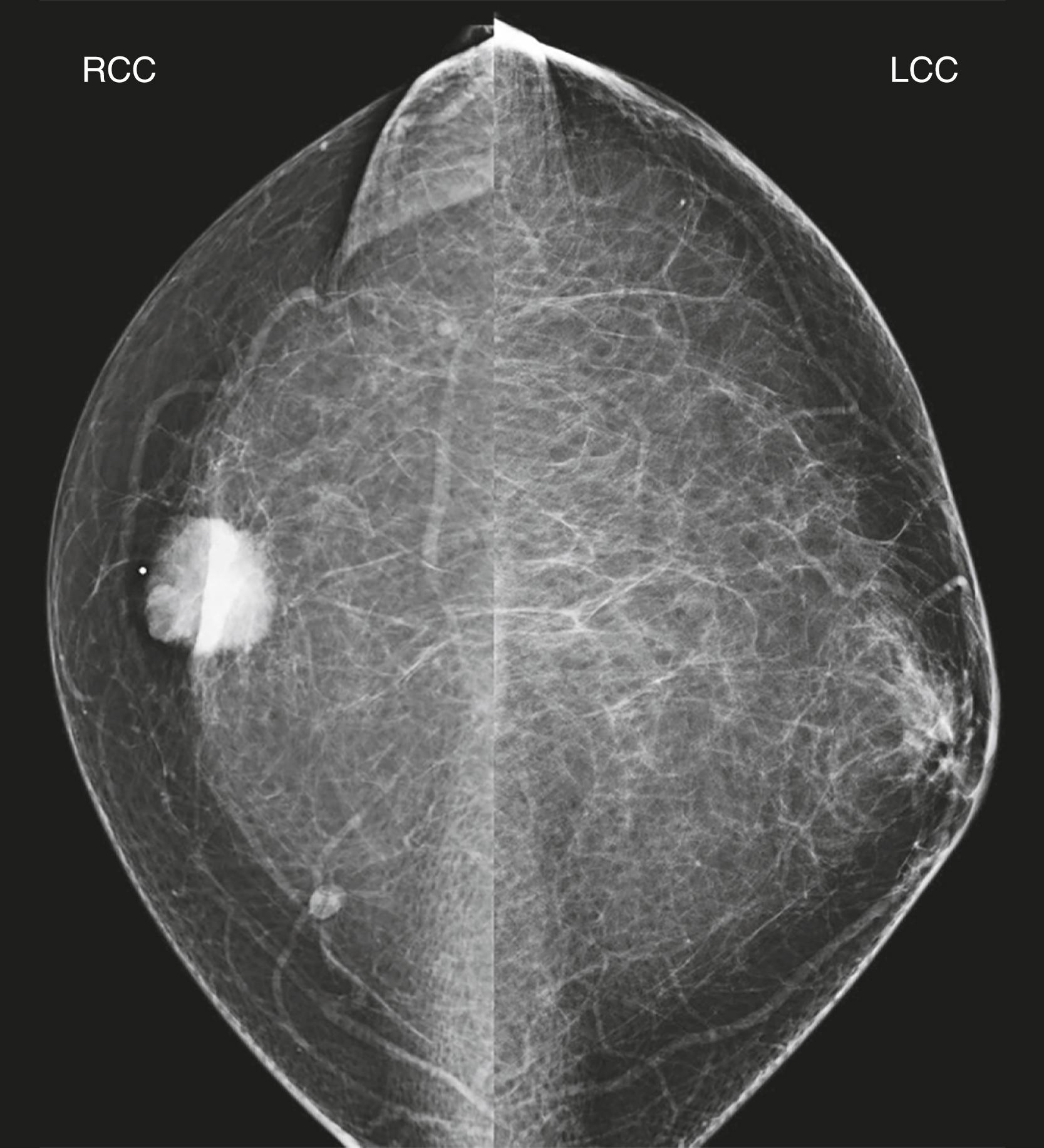
The most widely studied and utilized of all breast imaging studies is mammography. A mammogram is a type of low-dose x-ray imaging developed to evaluate clinical breast abnormalities and to screen patients for breast cancer ( Fig. 29.1 ).
Mammograms are performed on specialized radiographic units that produce low-energy x-rays. Compression is applied to the breast and used to improve image quality by reducing the thickness that the tissue x-rays must penetrate, decreasing radiation scatter, reducing the required radiation dose , and preventing motion. Mammographic images today are almost exclusively captured digitally, rather than on film.
Quality control is an important part of any mammography program. Radiologists are evaluated with regular audits to determine how well they are performing. These include evaluation of recall rate (number of mammograms read that require additional views and/or ultrasound) and positive predictive values (how many patients that undergo biopsy return positive, i.e., cancerous, results).
Digital breast tomosynthesis (DBT) (sometimes called 3D mammography ) is a type of mammography in which images are obtained at multiple different angles of the x-ray tube to create thin slices through the breast. It has been shown to reduce false-positive diagnoses while increasing invasive cancer detection ( Fig. 29.2 ).

Mammographic examinations are divided into screening mammography and diagnostic mammography. We discuss the differences between screening and diagnostic examinations later in this chapter.
Contrast-enhanced mammography (CEM) is a developing technique that uses the same equipment as standard mammography and digital breast tomosynthesis but applies a principle of tumor enhancement similar to contrast-enhanced MRIs.
After intravenous injection with iodinated contrast, a dual-energy mammogram is acquired. Two images of each breast are then available for display; one looks like a regular mammogram and the other highlights any areas that enhance with contrast after masking-out the tissues that do not enhance. Tumors are known to enhance because of tumor angiogenesis. ( Fig. 29.3 ).
.")
CEM may be especially useful in women at increased risk for developing breast cancer or those with dense breasts.
Breast ultrasound is most commonly used in conjunction with diagnostic mammography, but may also be performed as an additional screening method.
Indications for US include:
Problem-solving for asymptomatic patients recalled from a screening mammogram for additional breast imaging
Evaluating symptomatic patients ( Fig. 29.4 )

The initial study used in average-risk, symptomatic patients under 30 years of age
Studies have shown that screening high-risk patients and patients with dense breasts with ultrasound increases breast cancer detection over mammography alone.
Indications for MRI include:
Screening certain high-risk patients ( Fig. 29.5 )

Evaluating patients who have breast implants to determine the integrity of the implants
Evaluating patients with positive lymph nodes and an unknown primary site
Evaluating the response to neoadjuvant chemotherapy . Neoadjuvant chemotherapy refers to treatment that is given to reduce the size of a tumor in advance of more definitive therapy, such as surgery.
In some cases, newly diagnosed breast cancer to look for extent of disease, contralateral disease, and multiple cancers
Breast MRI is the most sensitive of all breast imaging modalities, but also the most expensive. Some patients cannot tolerate an MRI because of feelings of claustrophobia from the scanner or because they have certain medical devices , such as pacemakers, or ferromagnetic foreign bodies, such as some surgical clips.
MRI is the gold standard for evaluating the structural integrity of silicone breast implants discussed later in this chapter.
Other modalities included under the umbrella of breast imaging include molecular breast imaging, positron emission tomography (PET), and even CT.
We will concentrate on the modalities of mammography , US, and MRI , the studies used most widely today.
The purpose of screening mammography is to try to detect breast cancer in asymptomatic patients.
The sensitivity of mammography in detecting a breast abnormality depends on breast density: as density increases (tissue becomes whiter) sensitivity decreases. As with all conventional radiography, fat appears gray on mammography, whereas the imaging signs of breast cancer are whiter. This is why the denser (“whiter”) a patient’s underlying breast tissue is, the more difficult it is to detect a cancer among normal tissue. Finding cancer in a dense breast has been likened to looking for a polar bear in a snowstorm.
Breast density is divided into four categories, ranging from almost entirely fatty to very dense (see Fig. 29.1 ).
Every screening mammogram consists of two views of each breast, the craniocaudal (CC) view and the mediolateral oblique (MLO) view ( Figs. 29.6 and 29.7 ).


Multiple randomized controlled trials (RCTs) have shown at least a 22% reduction in breast cancer mortality in women who undergo screening mammography versus those who do not. More current and larger-scale observational studies report a 38% mortality reduction from breast cancer among those screened.
The American College of Radiology (ACR) recommends annual mammographic screening beginning at age 40 for women at average risk and intermediate risk , such as women with a personal history of breast cancer ( Table 29.2 ). Other organizations also have guidelines.
| Risk Factors | Start Screening | Frequency |
|---|---|---|
| Average | Age 40 | Annual screening |
| Women with certain BRCA1 or BRCA2 mutations or who are untested but have first-degree relatives (mothers, sisters, or daughters) who are proved to have BRCA mutations | Age 30 | Annual screening |
| Women with histories of mantle radiation (usually for Hodgkin disease) received between the ages of 10 and 30 | Starting 8 years after the radiation therapy, but not before age 25 | Annual screening |
| Women with ≥20% lifetime risk for breast cancer on the basis of family history (both maternal and paternal) | Starting by age 30 (but not before age 25), or 10 years earlier than the age of diagnosis of the youngest affected relative, whichever is later | Annual screening |
| Women with mothers or sisters with premenopausal breast cancer | Starting by age 30 (but not before age 25), or 10 years earlier than the age of diagnosis of the youngest affected relative, whichever is later | Annual screening |
| Women with biopsy-proven lobular neoplasia (lobular carcinoma in situ and atypical lobular hyperplasia), atypical ductal hyperplasia (ADH), ductal carcinoma in situ (DCIS), invasive breast cancer, or ovarian cancer | From time of diagnosis, regardless of age | Annual screening |
Some organizations point to the risks or harms of mammography. These include mammograms that are interpreted as abnormal, but turn out to be normal, or biopsy recommendations that reveal benign disease (false-positive) as well as the issue of overdiagnosis, meaning detecting cancers that may not be lethal.
Although cancers may be low grade and grow slowly, they do not disappear without treatment. The ACR contends that overdiagnosis should not be a factor in deciding when to start screening or deciding the interval between examinations.
Screening recommendations from the ACR have level-one evidence to support clear guidelines: start yearly screening at age 40. Other organizations vary in their recommendations, which may make it difficult for patients to decide when and how frequently they should be screened.
At what age should screening mammograms stop? Randomized controlled trials proved the mortality reduction from screening stopped at age 74, but there have been numerous studies that show continued benefit for women over the age of 74. The ACR recommends that screening be stopped based on a woman’s health status and not on her age.
The indications for diagnostic mammography are listed in Box 29.2 .
Breast symptoms (e.g., pain, lumps, nipple discharge)
Need for a more extensive examination for potential abnormalities detected at the time of their screening mammogram
A typical diagnostic imaging workup is shown in Fig. 29.8 for patients with breast symptoms.

Patients recalled because of prior screening mammography findings or undergoing a diagnostic mammogram may be evaluated using a variety of additional mammographic views. Some of these additional views are spot compression images, spot compression magnification views, true lateral or 90-degree lateral views, rolled views, exaggerated views, and cleavage views, as well as US.
Although the majority of symptomatic breast cancers will display an abnormality on mammography, US, or both, some cancers will have no imaging correlate to a clinically palpable finding or a reported symptom. For example, invasive lobular carcinomas are classically difficult to detect with imaging and can also be subtle clinically ( Table 29.3 ).
| Noninvasive | Ductal Carcinoma In Situ (DCIS) | |
|---|---|---|
|
|
| Invasive | Invasive Ductal Carcinoma (IDC) | Invasive Lobular Carcinoma (ILC) |
|---|---|---|
|
|
|
| Inflammatory Breast Cancer | ||
|
||
| Medullary Breast Cancer | ||
|
||
| Tubular Carcinoma | ||
|
||
| Other Types of Cancer | ||
| Mucinous, papillary, and medullary carcinoma with not otherwise specified (NOS) | ||
Therefore, anything that is clinically palpable , but has a negative imaging workup, should be evaluated clinically , often by a breast surgeon. The clinician can then decide whether to do follow-up studies or a biopsy.
Patients who undergo diagnostic mammography typically receive their results at the conclusion of the examination(s) so that they understand what to do next and have the opportunity to ask questions.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here