Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

In developed countries, where the major pyogenic infections have been brought more or less under control, chronic inflammatory conditions result in a huge burden of morbidity and mortality. In less industrialised countries, certain infections, such as tuberculosis, typically cause a chronic inflammatory response and are responsible for a large amount of disease. By definition chronic inflammation lasts longer than acute inflammation. Different stimuli may cause variations in the morphological appearances but, overall, in the chronic inflammatory infiltrate lymphocytes, macrophages and plasma cells predominate, in contrast to acute inflammation where the major cell type is the neutrophil. The hallmark features of chronic inflammation are ongoing tissue damage, a chronic inflammatory infiltrate and fibrosis. Chronic inflammation may be subdivided as follows:
Non-specific chronic inflammation : arises following non-resolution of acute inflammation, e.g. chronic peptic ulcer, chronic abscess
Specific (primary) chronic inflammation : arises de novo in response to certain types of injurious agents, e.g. rheumatoid arthritis, idiopathic pulmonary fibrosis
Granulomatous inflammation : is a subset of specific chronic inflammation characterised by the presence of granulomas, e.g. sarcoidosis, tuberculosis (see Ch. 5 ).
Chronic inflammation may arise following an episode of acute inflammation (see Ch. 3 ) where the acute inflammatory response has not been adequate to neutralise or destroy the noxious stimulus. In this situation, tissue damage, acute inflammation, granulation tissue, tissue repair and chronic inflammation co-exist. There may be active tissue damage in one area with ongoing acute inflammation, while in adjacent areas fibrosis and a chronic inflammatory infiltrate are seen. The chronic inflammatory infiltrate is dominated by tissue macrophages, lymphocytes and plasma cells ( Fig. 4.1 ), in contrast to the marked preponderance of neutrophils in the acute inflammatory response. This type of chronic inflammation represents a dynamic balance between tissue destruction and repair. The course of the disease might include repeated acute phases when tissue damage is predominant and intervening chronic phases when chronic inflammation smoulders along with ongoing tissue repair. The outcome of non-specific chronic inflammation depends on whether local and systemic factors favour the injurious agent or the process of healing ( Table 4.1 ). Chronic inflammation usually heals by fibrosis.
.")
| Factors that impair resolution and healing | Factors that aid resolution and healing |
|---|---|
| Poor nutrition | Administration of appropriate antibiotics |
| Immunosuppression | Surgical removal of foreign material |
| Persisting tissue damage and/or infection | Surgical removal of dead tissue |
| Retained foreign material | General attempts to improve nutrition |
| Sequestered dead tissue | Drugs that specifically modify the inflammatory response |
| Poor blood supply | |
| Deficiency of intrinsic anti-inflammatory factors | |
| Diabetes mellitus and other chronic illnesses | |
| Certain medications, such as corticosteroids | |
| Older age |
E eosinophil F fibrous granulation tissue Fi fibroblast L lymphocyte M muscular wall Ma macrophage P plasma cells Sc scar Sl necrotic slough V vascular granulation tissue
Understanding of the role of H. pylori has revolutionised management of peptic ulceration. In the past, peptic ulcers were treated by surgical procedures, which aimed to reduce acid production, such as partial gastrectomy (to remove the antral source of gastrin) or vagotomy and pyloroplasty (removing the vagal-driven pathway of acid secretion but requiring release of the pylorus since the vagus also controls gastric emptying). Such operations were associated with considerable morbidity. Conventional medical management of peptic ulcer disease employed a range of drugs, from simple alkalis to neutralise excess acid, through various drugs, which interfere with normal physiological control of acid secretion (e.g. adrenergic antagonists and histamine (H2) receptor blockers) to the more recent use of proton pump inhibitors (PPIs) , which effectively block the final common pathway of acid production. Although acid-blocking drugs were usually effective, treatment had to continue for the rest of the patient’s life. Now, treatment usually requires only a short course of eradication therapy, using a combination of two antibiotics with a proton-pump inhibitor (triple therapy) .
 Entire ulcer (LP); (B) surface layers of ulcer (MP); (C) deep layers of ulcer (MP).")
This type of chronic inflammation arises by different mechanisms from non-specific chronic inflammation. Primary chronic inflammation may be either granulomatous or non-granulomatous . A key feature in chronic inflammation is the activation of macrophages, which orchestrate the chronic inflammatory response. Macrophages may become activated by either immune or non-immune mechanisms. Activated macrophages not only become more efficient at phagocytosis and killing of organisms, but also secrete a wide range of factors that control the behaviour of other inflammatory cells (e.g. chemotactic factors, lymphokines) and which induce fibrosis (e.g. fibrogenic cytokines, growth factors). The types of agent that can invoke primary chronic inflammation include:
Immunological
Low-toxicity organisms such as Treponema sp., the causative organism of syphilis and yaws
Infective organisms that grow within cells, e.g. viruses, Mycobacteria
Hypersensitivity reactions such as hypersensitivity pneumonitis
Autoimmune conditions such as systemic lupus erythematosus
Infections by fungi, protozoa and parasites.
Non-immunological
Foreign body reactions
Inert noxious materials such as silica, talc, asbestos or beryllium.
Primary chronic inflammation of the immune type may be either granulomatous or non-granulomatous. A good example of the non-granulomatous immune type is hepatitis B virus infection (HBV) (see Fig. 14.3 ). Virus-infected cells in the liver incite a cell-mediated immune response, producing cytotoxic T lymphocytes, which kill virus-infected hepatocytes. Some individuals mount an effective immune response and clear the infection, whilst in others there is ongoing infiltration of the liver by lymphocytes over months or years, a condition known as chronic active hepatitis . In these people, there is continuing destruction of hepatocytes and fibrosis of the liver, which may eventually cause cirrhosis. As in many examples of chronic inflammation, the tissue damage is due to the inflammatory response rather than the virus itself. In non-immune type primary chronic inflammation, the mechanisms are less clear. However, certain materials such as silica can directly activate macrophages to release mediators that induce an inflammatory reaction and fibrosis.
The defining feature of granulomatous inflammation is the presence of activated epithelioid macrophages and multinucleate giant cells derived from macrophages. Epithelioid macrophages are so named because they bear some resemblance histologically to epithelial (squamous) cells. These cells may form well-circumscribed granulomas (clusters), which are generally surrounded by lymphocytes, macrophages, fibroblasts and varying degrees of fibrosis. Granulomatous primary chronic inflammation may arise by either immune or non-immune mechanisms. The immune type, known as the delayed hypersensitivity response , is epitomised by tuberculosis (see Ch. 5 ). T lymphocytes responding to mycobacterial antigens are activated and divide and mature to produce helper T cells. The helper T cells in turn secrete lymphokines (e.g. interferon (IFN)-γ) that induce the transformation of macrophages into activated epithelioid macrophages and giant cells.
Non-immune granulomatous inflammation is exemplified by the foreign body reaction, for example in response to suture material after a surgical procedure, or when a rose thorn becomes embedded in the skin. Fig. 4.9 is an example of such a reaction and shows plant material (from faeces) embedded in the wall of the bowel in a patient with diverticular disease. In some granulomatous conditions such as Crohn’s disease and sarcoidosis, the mechanism is unclear: infective causes have been postulated but never proven.
The term granuloma needs some clarification. In general, granuloma means a cluster of epithelioid macrophages as opposed to granulation tissue as defined in Ch. 3 . However, in the past, ‘granuloma’ was applied to both a granuloma and granulation tissue and a few examples remain in current terminology where the old usage persists. Examples include an apical granuloma referring to a mass of granulation tissue at the root of a tooth and a pyogenic granuloma (lobular capillary haemangioma), which is a mass of granulation tissue in a healing wound.
A abscess cavity F fibrosis G granulation tissue H hair shaft P pus
Some granulomas develop necrosis in their central area. The classical form is caseous necrosis, which is almost always found in tuberculosis (see Ch. 5 ). Caseous necrosis appears creamy macroscopically (caseous means ‘like cream cheese’). By light microscopy, caseous necrosis is featureless and eosinophilic, containing few cells. Some other granulomatous conditions, such as atypical mycobacterial infection, also develop central necrosis but the necrosis is suppurative with plentiful neutrophils, often called suppurating or necrotising granulomas . Some common types of granulomatous inflammation are characterised by their lack of necrosis; examples of this type are Crohn’s disease and sarcoidosis .
Chronic fibrosis, whatever the cause, can be a cause of great morbidity and sometimes mortality. Fibrosis and scar formation are normal parts of tissue healing after significant damage. However, in some individuals, in association with certain insults, there is a tendency to develop excess fibrosis such that the fibrous tissue impairs organ function. Idiopathic pulmonary fibrosis as described above is one example; others include keloid scars and intra-abdominal adhesions that may arise and persist after abdominal surgery.
The underlying immune basis of a group of unusual fibrosing disorders (including retroperitoneal fibrosis, Riedel’s thyroiditis, chronic sclerosing sialadenitis and autoimmune pancreatitis) has recently been recognised. These are now described using the term IgG4 related disease. All of these disorders are linked by the tendency to form tumour-like lesions with numerous lymphocytes and plasma cells, many of them IgG4 positive plasma cells, prominent storiform fibrosis (with the cells arranged in a cartwheel/woven pattern) and obliterative phlebitis (inflammation obliterating small veins). Some patients also have a raised serum IgG4 level.
Other instances of excessive fibrosis result from known causes (e.g. infections such as tuberculosis (see Ch. 5 ) and fibrosis of a transplanted kidney in chronic rejection.
A enlarged alveolar space E epithelioid macrophage F fibrous tissue I interstitium L lymphocytes P type 2 pneumocyte hyperplasia
A asteroid body F foreign body giant cells G non-caseating granuloma L lipogranuloma M epithelioid macrophages P plant material S Schaumann body
L lipogranulomas
| Type of chronic inflammation | Histological features | Some examples | Figure |
|---|---|---|---|
| Non-specific: follows on from unresolved acute inflammation | Mixed inflammatory response with lymphocytes, plasma cells, eosinophils, neutrophils. Characterised by mixture of acute inflammation, chronic inflammation and attempts at healing (granulation tissue, fibrosis) |
Chronic peptic ulcer Bronchiectasis ( E-Fig. 4.3 G ) Pilonidal sinus Ulcerative colitis |
4.2 4.3 4.4 13.18 |
| Specific chronic inflammation (non-granulomatous) | The inflammatory infiltrate consists predominantly of lymphocytes, plasma cells and macrophages Sometimes there are variable numbers of eosinophils and mast cells |
Viral infections Idiopathic pulmonary fibrosis ( E-Fig. 4.6 G ) Cellular rejection of transplanted kidney Lichen planus |
5.12–5.14 4.5 4.6 21.7 |
| Specific chronic inflammation (granulomatous) | This type of inflammation is characterised by the formation of granulomas: aggregates of epithelioid macrophages, with or without giant cells | Sarcoidosis Foreign body giant cell reaction Tuberculosis Leprosy Crohn’s disease |
4.8 4.9 5.3–5.7 5.9 13.16 |
. (A) LP; (B) HP.")
.")
 Foreign body giant cell (HP); (B) Langhans’ giant cell (HP).")
 Sarcoidosis in a lymph node (MP); (B) sarcoid granulomas (HP).")
 Foreign body granuloma (LP); (B) giant cell with inclusion (HP).")
 Xanthogranulomatous cholecystitis (MP); (B) lipogranuloma in fat necrosis (HP).")
. This micrograph illustrates the body of the stomach in the non-distended state. The mucosa M is thrown into prominent folds or rugae and consists of gastric glands that extend from the level of the muscularis mucosae MM to open into the stomach lumen via gastric pits or foveolae GP . The muscularis propria comprises the usual inner circular C and outer longitudinal L layers, but the inner circular layer is reinforced by a further inner oblique layer O . The submucosa SM is relatively loose and distensible and contains the larger blood vessels. The serosal layer, which covers the peritoneal surface, is thin and barely visible at this magnification. The adipose tissue of the lesser and greater omentum is attached along the lesser and greater curvature of the stomach (not illustrated in this micrograph). Lymph nodes and large blood vessels lie within this omental fatty tissue.")


 bronchus Elastic van Gieson (MP). As bronchi diminish in diameter, the structure progressively changes to resemble more closely that of large bronchioles. The epithelium, just visible in this image, is tall and columnar with little pseudostratification. Goblet cell numbers are greatly diminished. The lamina propria is thin, elastic and completely encircled by smooth muscle M which is disposed in a spiral manner. This arrangement permits contraction of the bronchi in both length and diameter during expiration. Seromucinous glands G are sparse in the submucosa. These glands are rarely found within smaller airways. The cartilage framework C is reduced to a few irregular plates. Cartilage does not usually extend beyond tertiary bronchi. Note that the submucosa SM merges with the surrounding adventitia and then with the lung parenchyma. Small aggregates of lymphocytes L , part of the mucosa-associated lymphoid tissue (MALT), are seen in the adventitia.")
. Terminal bronchioles T are the smallest diameter passages of the purely conducting portion of the respiratory tree. Beyond this, branches become increasingly involved in gaseous exchange. Each terminal bronchiole divides to form short, thinner walled branches called respiratory bronchioles R which contain a small number of single alveoli A in their walls. The epithelium of the respiratory bronchioles is devoid of goblet cells and largely consists of ciliated cuboidal cells and smaller numbers of non-ciliated cells called Clara cells . In the most distal part of the respiratory bronchioles. Clara cells become the predominant cell type. Clara cells have three functions: • They produce one of the components of surfactant . • They act as stem cells , i.e. they are able to divide, differentiate and replace other damaged cell types. • They contain enzyme systems which can detoxify noxious substances.")

 H&E (LP); (B) schematic diagram. Lymph nodes are small, bean-shaped organs situated in the course of lymphatic vessels such that lymph draining back to the bloodstream first passes through one or more lymph nodes. Inactive nodes are only a few millimetres long but may increase greatly in size when mounting an active immunological response. Most lymph nodes in the body show some degree of ‘reactive change’ in response to the constant barrage of antigen to which they are exposed. As shown in micrograph (A) , the outer part of the lymph node is highly cellular and is known as the cortex Cx , whilst the central area, the medulla M , is less cellular. At the hilum H , the efferent lymphatic drains efferent lymph from the lymph node. The hilum is also the site of entry of the artery bringing blood to the lymph node and the vein leaving the node. The lymph node is surrounded by a collagenous capsule C from which trabeculae T extend for a variable distance into the substance of the node. Afferent lymphatic vessels , as shown in diagram (B) , divide into several branches outside the node then pierce the capsule to drain into a narrow space called the subcapsular sinus S that encircles the node beneath the capsule. From here, a labyrinth of channels called cortical sinuses passes towards the medulla through the cortical cell mass; sinuses adjacent to the trabeculae ( trabecular sinuses ) pursue a more direct course towards the medulla, but nevertheless form part of the cortical sinus system. The cortical sinuses are generally difficult to visualise because of their highly convoluted shape and numerous fine extensions that penetrate the cellular mass of the cortex. The superficial cortex contains a number of dense cellular aggregations, the follicles . Most of these in this particular example are secondary follicles SF with a pale-stained germinal centre ; others are inactive primary follicles PF . B cells respond to antigen in the cortex and undergo stimulation, clonal expansion and maturation in the follicles, the presence of germinal centres indicating that an active immune response is underway.The deeper cortex or paracortex P is also densely cellular but has a more homogeneous staining appearance. T lymphocytes interact with antigen presenting cells in the paracortex and undergo a similar process of activation and clonal expansion. T helper cells migrate towards the cortex to provide ‘help’ to B cells while activated cytotoxic T cells leave the node to perform their functions in the periphery. At the left of the field, some lymphoid follicles appear to be located deep in the paracortex; this is not the case but is a product of the plane of section, which passes at that point through the superficial cortex. The dominant feature of the medulla is the network of broad interconnected lymphatic channels called medullary sinuses MS that converge upon the hilum in the concavity of the node. Lymph drains from the hilum in the efferent lymphatic into one or more additional nodes, which in turn drain into more proximal nodes before eventually joining the blood stream via the thoracic duct or right lymphatic duct . Thus the lymph is filtered through a number of lymph nodes to facilitate the exposure of large numbers of lymphocytes to antigens in the lymph. Extensions of the cortical cell mass extend into the medulla as medullary cords MC . The blood supply of the lymph node, as shown in diagram (B) , is derived from one or more small arteries which enter at the hilum and branch in the medulla, giving rise to extensive capillary networks supplying the cortical follicles, paracortical zone and medullary cords. The vascular system provides the main route of entry of lymphocytes into the node, as well as supplying its metabolic requirements. Within the paracortex, the postcapillary high endothelial venules (HEV) have a cuboidal endothelium specialised for the exit of lymphocytes. Recognition by lymphocytes of these exit sites requires the presence of specific complementary adhesion molecules on the surface of both the endothelial cells and lymphocytes. Different groups of lymphocytes home to different tissues. Thus lymphocytes from the mucosa of the gut migrate to mesenteric lymph nodes, then to the spleen and back to mucosal tissues. Lymphocytes from the skin travel to their regional lymph nodes and then return to the skin. This is made possible by the different adhesion molecules or vascular addressins in the HEV of the different lymph node groups and the corresponding binding molecules on the lymphocytes. The HEV drain into small veins that leave the node via the hilum.")
 H&E (LP); (B) H&E (MP); (C) H&E (LP). The intrahepatic bile collecting system merges to form right and left hepatic ducts which join, creating a single large duct, the common hepatic duct. On leaving the liver, this is joined by the cystic duct which drains the gallbladder. The common bile duct so formed joins the pancreatic duct to form the short ampulla of Vater before entering the duodenum. Bile draining down the common hepatic duct is shunted into the gallbladder where it is stored and concentrated. The major bile ducts outside the liver are collectively called the extrahepatic biliary tree .The gallbladder is a muscular sac lined by a simple columnar epithelium. It has a capacity of about 100 mL in humans. The presence of lipid in the duodenum promotes the secretion of the hormone cholecystokinin-pancreozymin (CCK) by neuroendocrine cells of the duodenal mucosa, stimulating contraction of the gallbladder and forcing bile into the duodenum. Bile is an emulsifying agent, facilitating the hydrolysis of dietary lipids by pancreatic lipases. Micrograph (A) shows the wall of a gallbladder in the non-distended state in which the mucosa is thrown up into many folds. The relatively loose submucosa S is rich in elastic fibres, blood vessels and lymphatics which drain water reabsorbed from bile during the concentration process. The fibres of the muscular layer M are arranged in longitudinal, transverse and oblique orientations but do not form distinct layers. Externally, there is a thick collagenous adventitial (serosal) coat A , conveying the larger blood and lymphatic vessels. In the neck of the gallbladder and in the extrahepatic biliary tree, mucous glands are found in the submucosa. Mucus may provide a protective surface film for the biliary tract. At high magnification in micrograph (B) , the simple epithelial lining of the gallbladder is seen to consist of very tall columnar cells with basally located nuclei. Numerous short, irregular microvilli account for the unevenness of the luminal surface. The lining cells concentrate bile 5- to 10-fold by an active process, the resulting water passing into lymphatics in the lamina propria LP . Micrograph (C) illustrates the wall of the cystic duct, which is formed into a twisted mucosa-covered fold F known as the spiral valve of Heister . The flow of bile and pancreatic juice into the duodenum is controlled by the complex arrangement of smooth muscle known as the sphincter of Oddi . The components of this structure include the choledochal sphincter at the distal end of the common bile duct, the pancreatic sphincter at the end of the pancreatic duct, and a meshwork of muscle fibres around the ampulla. This arrangement controls the flow of bile and pancreatic juice into the duodenum and, at the same time, prevents reflux of bile and pancreatic juice into the wrong parts of the duct system. When the choledochal sphincter is closed, bile is directed into the gallbladder where it is concentrated.")

A 72-year-old patient with non-insulin dependent diabetes and peripheral vascular disease falls at home and suffers a complicated fracture of his right wrist. Which of the following factors will NOT delay fracture healing in this patient? (Select one answer)
Corticosteroid treatment
High serum glucose level
Fragments of dead bone at the fracture site
Surgery to align the bones and remove dead tissue
Infection
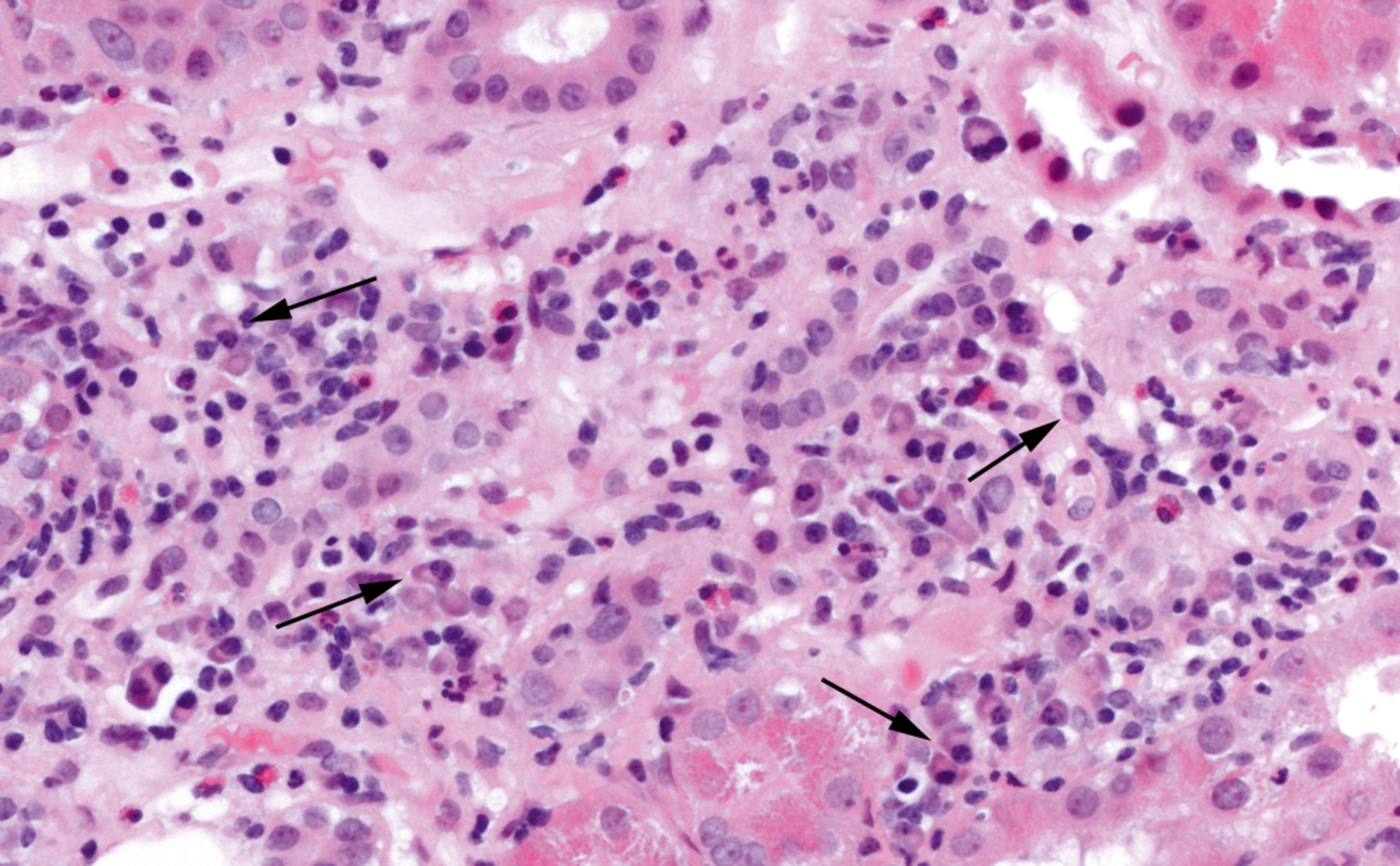
This image shows chronic inflammation in the kidney. Which cells are indicated by the arrows? (Select one answer)
Eosinophils
Macrophages
Neutrophils
Epithelial cells
Plasma cells
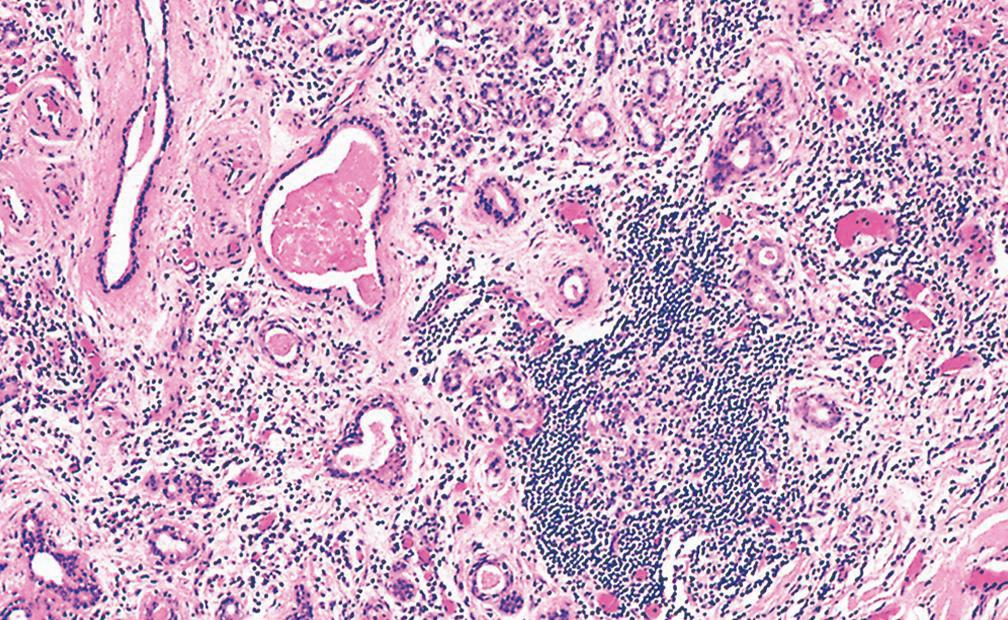
This image shows a salivary gland with typical features of chronic sialadenitis. Which of the following features is NOT illustrated? (Select one answer)
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here
