Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124


 Access video and video lecture content for this chapter online at Elsevier eBooks+
Access video and video lecture content for this chapter online at Elsevier eBooks+
Vascularized lymph node transplant (VLNT) is one type of physiologic surgical treatment for lymphedema that has been shown to be effective in reducing affected limb girth and decreasing reliance on decongestive therapy for patients with upper and lower extremity lymphedema. It has been employed for both primary, or congenital, lymphedema, as well as secondary lymphedema of the extremities that may result from infection, trauma, or oncologic resection. VLNT was described in 1979 by Shesol in a rat model and then in 1988 by Becker in an animal model utilizing inguinal node transplant. Shortly after, Chen and O’Brien described inguinal and omental node transplant in a canine model and showed improvement in affected limb volume. In humans, the first VLNT procedure to gain popularity was transplant of superficial inguinal nodes from the groin to the axilla in postmastectomy upper extremity lymphedema. However, concern was raised over risk of iatrogenic secondary lymphedema in the lower extremity with the groin donor site. To decrease or eliminate this risk, alternative donor sites, including submental, lateral thoracic, supraclavicular, and intra-abdominal nodes, were developed utilizing microsurgical free tissue transplant techniques.
VLNT is thought to have two main mechanisms of action – as a lymphatic pump and through stimulation of lymphangiogenesis. Within the lymph node, there is a plexus through which the lymphatic and venous systems communicate. Particularly when nodes are placed in a dependent, non-anatomic position within an affected extremity, lymph nodes have been shown to work through a catchment effect. Fluid is shunted from the diseased, high-pressure interstitium to the low-pressure environment of the lymph node flap. Experimental studies have supported this mechanism by demonstrating distal migration of indocyanine green (ICG) toward a transplanted flap, after proximal intradermal injection in an affected extremity.
The other proposed mechanism of action for VLNT is through lymphangiogenesis. Unlike the almost immediate results achieved as a lymphatic pump, this effect is expected to have longer onset. Transplanted nodes deliver growth factors such as VEGF-C to the recipient site, stimulating the generation of new lymphatic channels and repairing damaged lymphatics. Proximal, anatomic positioning of lymph nodes is typically proposed based on this mechanism, and postoperative imaging has demonstrated restored lymphatic vasculature following VLNT.
All patients considered for physiologic surgery to address lymphedema should be optimized non-surgically. This optimization includes weight loss, physical exercise, and effective decongestive therapy. A minimum of three months of active involvement in a physical therapy program is required, resulting in the reduction of limb fluid prior to surgery. Patients with both primary and secondary lymphedema are evaluated as candidates for lymphovenous bypass (LVB) and/or VLNT. LVB may not be appropriate for patients with more advanced disease or those with congenital lymphedema. In both instances, affected limbs demonstrate abnormal lymphatic development, structure, and/or function, resulting in inability to perform or failure of LVB. In contrast, VLNT does not rely upon functional native lymphatic vessels. Therefore, it may be used in these patients. Generally, VLNT is considered for patients with International Society of Lymphology (ISL) stage II–IV lymphedema, with earlier stages managed nonoperatively or with LVB. Patients with active malignancy should not undergo VLNT.
In the upper extremity, nodes may be transplanted to the axilla, elbow, or wrist, and in the lower extremity, to the groin, distal thigh, proximal leg, or ankle. Recipient artery and vein of appropriate caliber to match the flap pedicle should be identified. In the axilla, branches of the thoracodorsal or axillary system are usually appropriate, and in the groin, superficial branches from the femoral vessels just below the inguinal ligament can be used.
More proximal recipient sites in the axilla or groin are easily camouflaged, and there is typically sufficient surrounding tissue for closure without need for a skin paddle with a small lymph node flap. In cases of secondary lymphedema with previous lymph node dissection, tumor removal, or traumatic scar, proximal placement facilitates scar release. In these cases, lymph nodes may be harvested with an accompanying muscle, myocutaneous, or fasciocutaneous flap, with the additional soft tissue used to correct soft-tissue deficiency. For patients with a history of breast cancer and acquired amastia, VLNT may be combined with autologous breast reconstruction with either pedicled or free flaps.
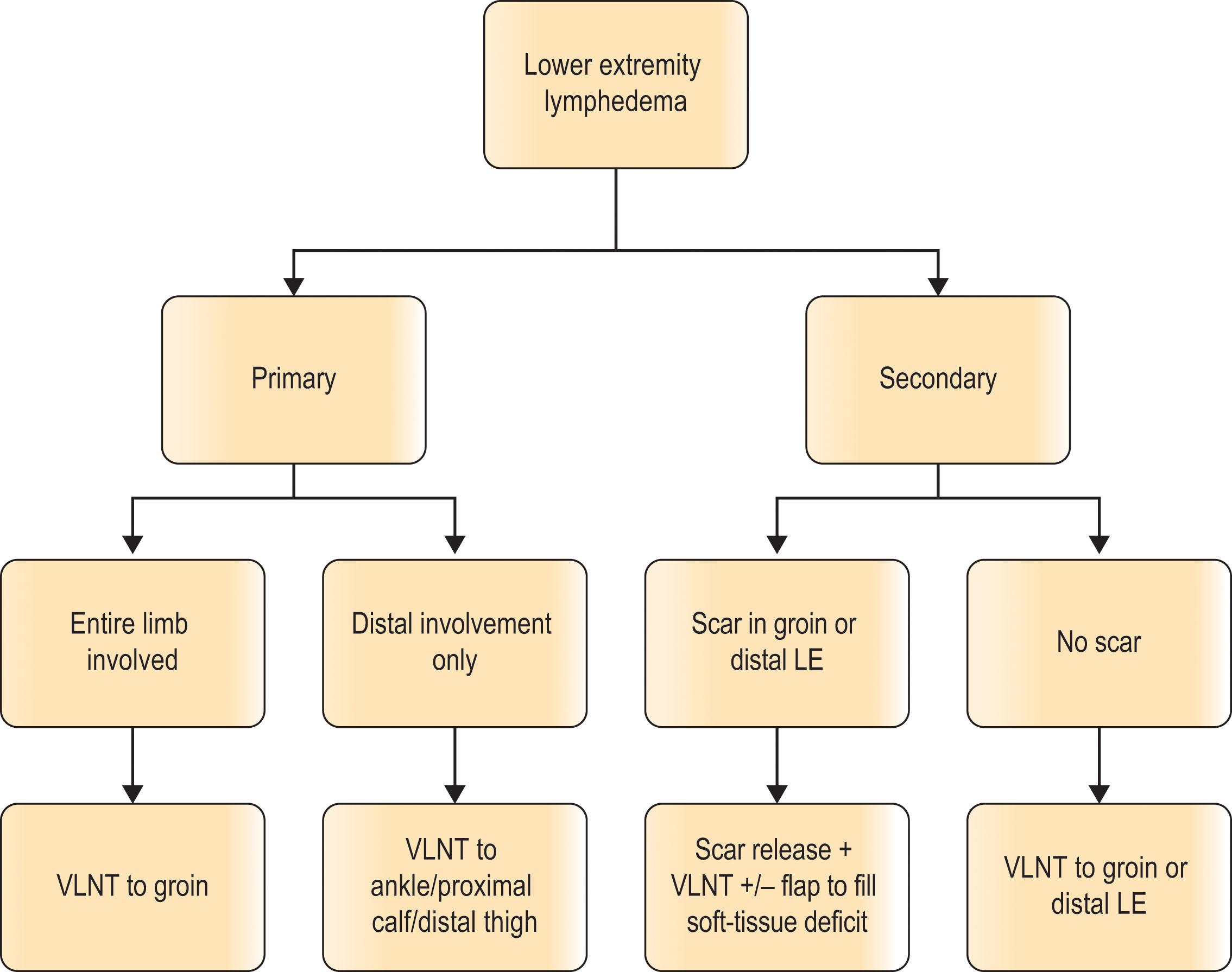
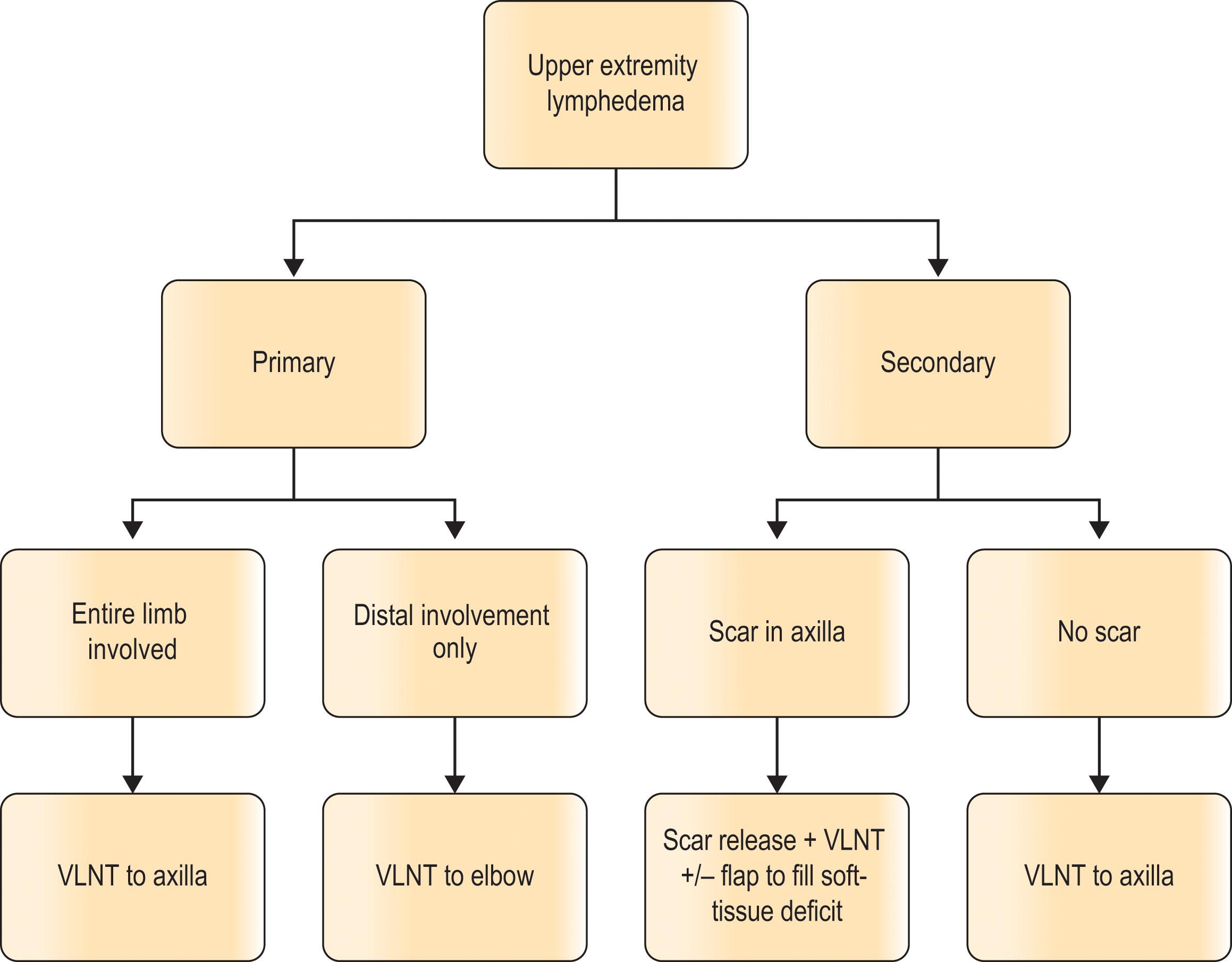
Distal, non-anatomic placement is also possible, but incisions are more difficult to hide. In these sites, the VLNT is more likely to act as a lymphatic pump. In our opinion, distal recipient sites are more appropriate for primary lymphedema or previous abdominal or pelvic node dissection without significant scar tissue at the recipient site. Another indication would be when a patient is not a candidate for effective lymphovenous bypass. In these cases, the recipient site may be selected based on proximal extent of lymphedema. For example, if a patient has primary lymphedema that affects only the foot and calf, lymph nodes may be placed in the distal thigh. But if the entire limb is involved, VLNT to the groin is typically recommended. Our approach to VLNT recipient site selection for the upper and lower extremity is presented in Algorithms 3.41 and 3.4.2 included in this chapter.
Donor site selection in VLNT is based on surgeon preference, as well as patient anatomy ( Table 3.4.1 ). In the case of upper extremity lymphedema, ipsilateral supraclavicular nodes are not recommended, but contralateral supraclavicular, ipsilateral lateral thoracic, groin, submental, or intra-abdominal nodes may be used. For lower extremity lymphedema, groin nodes are not harvested, but all other donor sites may be employed. A careful history of previous surgery and trauma should be taken for each patient, and patient preference for preferred donor site is also considered.
| Donor site | Advantages | Disadvantages |
|---|---|---|
| Supraclavicular |
|
|
| Submental |
|
|
| Groin |
|
Potential for donor site lymphedema |
| Lateral thoracic |
|
Potential for donor site lymphedema |
| Omentum/gastroepiploic | No risk for donor site lymphedema | Intra-abdominal surgery with associated risks |
VLNT may be combined with other forms of physiologic or non-physiologic lymphedema surgery. Because of their different mechanisms of action, VLNT is frequently performed in conjunction with LVB for patients who have functional lymphatics amenable to bypass. Non-physiologic debulking procedures may also be done, but the most appropriate timing of such a combination remains under debate. Some surgeons advocate debulking through excision or liposuction prior to VLNT while others recommend debulking after VLNT and only if desired volume reduction and symptomatic relief are not achieved with VLNT alone.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here