Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

The approach and utilization of radiation therapy (RT) for the treatment of hematologic malignancies have seen many changes throughout the years. Advances in imaging and technology have allowed for more precise delineation and targeting of disease. This, along with a reduction in radiation doses and treatment volume, have resulted in increased sparing of normal tissues and dramatically reduced short- and long-term toxicities previously associated with RT. With the majority of hematologic malignancies being highly responsive to radiation, RT plays a critical role in disease management. Use of RT ranges from definitive primary treatment to adjuvant therapy in combination with systemic therapies, as well as salvage or palliative therapy in the relapsed/refractory setting. This chapter will detail the historical changes in the application of RT for hematologic malignancies and focus on the current role of RT based on modern staging, systemic therapies, response assessment, and RT delivery. We will provide current recommendations based on clinical evidence and published guidelines. The goal is to equip the hematologist and oncologist with an evidence-based approach to understanding the overall role and clinical applications, including new concepts in modern RT for a wide variety of hematologic malignancies.
Technological advances that are associated with the diagnosis, treatment response evaluation, and delivery of RT in the last several decades have allowed for more precise and personalized treatment applications for patients. Even within the last 30 years, advances in the components of RT delivery have allowed for higher precision in dose composition. The use of more advanced imaging acquisition for staging and planning has allowed for better patient selection and smaller treatment volumes, resulting in high rates of long-term tumor control with reduced normal tissue exposure and the associated short- and long-term complications. The use of combined systemic treatments with RT, including chemotherapy and more recent targeted and immunotherapy, have resulted in improved locoregional control and overall survival (OS). This chapter aims to provide a framework through which the image of radiation will shift from a one-size-fits-all, to the individualized targeted therapy that is currently used in most radiation oncology practices.
In 1950, Vera Peters was the first physician to definitively show that RT could be used to cure early-stage Hodgkin lymphoma (HL). Until that time, HL was thought to be incurable. Dr. Peters not only showed that high doses of fractionated RT resulted in a 5- and 10-year survival rate of 88% and 79%, but also proposed the importance of a staging system in prognosis. Historically, RT alone was used to treat early-stage HL, through the use of 2D imaging set up to bony landmarks. Extended-field radiation therapy (EFRT) included total nodal irradiation (TNI), mantle and paraaortic/splenic RT, mantle field RT, and inverted-Y field RT. These large-field treatments were associated with significant long-term toxicities, including risks of second malignancy and cardiac diseases. In the 1990s, in the context of combined modality therapy, EFRT was replaced by involved-field radiation therapy (IFRT), which included only involved nodal regions. However, similar to EFRT, IFRT still relied on 2D planning using bony landmarks to set field borders, with largely anterior-posterior beam arrangements, resulting in unnecessary exposure of a large amount of normal tissue. Involved-site radiation therapy (ISRT), the current standard treatment field, uses 3D-based simulation to incorporate the pre-chemotherapy volume into the clinical target volume, while excluding uninvolved areas and previously displaced organs based on tumor response. Involved-node radiation therapy (INRT), is a special case of ISRT where staging imaging is acquired with the patient in the RT position, using the same breathing instructions and immobilization devices. This typically results in further reduction in the irradiated volume by allowing more accurate target delineation. Pictorial representations of the changes in HL treatment fields over the years are useful in visualizing the substantial changes that RT has encountered over the years ( Fig. 95.1 ). Detailed guidelines on ISRT/INRT approaches for HL have been published and recently updated by the International Lymphoma Radiation Oncology Group (ILROG), available at https://www.ilrog.org/main-st . A Mini-Atlas of case examples, focusing on the technical aspect of RT, has also recently been published by the group.

There have been significant technological advances since the days of 2D planning and predominantly anterior-posterior beam arrangements to large treatment fields. With the advent of 3D planning, advanced radiation planning and treatment delivery including intensity-modulated radiation therapy (IMRT), proton beam therapy, image-guided radiation therapy (IGRT), and motion management techniques, highly conformal treatment with significant sparing of normal tissue can be achieved while maintaining disease control. IMRT improves conformality of radiation dose to target structures, while limiting doses to surrounding normal tissues by using multiple beams of varying intensities and shapes that change throughout the treatment to precisely irradiate a target. For mediastinal cases, the use of deep-inspiration breath-hold technique displaces the lungs and heart away from the radiation fields and has been shown to result in significantly reduced lung and heart doses. IGRT via daily cone-beam CT imaging results in further reduced doses to critical structures by allowing a narrower expansion of the clinical target volume to planning target volume. More recently, the use of a Magnetic Resonance Linear Accelerator (MR Linac), with its better image quality, its use of non-ionizing radiation, and its ability to adapt the daily radiation as tumor responds, has the potential to further reduce RT volume and normal tissue exposure. For proton-beam therapy, its dose profile with a sharper fall off can decrease unwanted dose to critical cardiac structures. Guidelines on the use of proton therapy for mediastinal lymphoma have been published by ILROG. Ultimately, it is critical that these various advanced radiation treatment approaches be adapted to provide the greatest benefit by accounting for patient characteristic, needs, and treatment goals.
Numerous dosimetric and modeling studies have estimated and quantified the reduction in doses to normal organs, including heart, lung, and breasts, using modern fields, doses, and techniques. Fig. 95.2 is an example of a modeling study showing significantly reduced estimated breast cancer, lung cancer, and cardiovascular mortality risks when comparing the historical mantle field with more limited radiation fields and modern radiation technology. There is a growing effort to track volumetric dose estimates to critical normal organs, including cardiac substructures such as left anterior descending artery, heart valves, and cardiac chambers. This will facilitate work on correlating dose-volume exposure of normal organs with late effects, which in turn will guide future treatment and follow-up.

Guidance on optimal use of modern imaging techniques in the staging, planning, treatment delivery, and follow-up of hematologic malignancies was recently published by ILROG. A baseline pre-treatment, [18 F]-fluorodeoxyglucose (FDG) positron emission tomography-computed tomography (PET/CT) is best practice for not only staging but also for RT planning and assessment of response to systemic treatment. Magnetic resonance imaging (MRI) is recommended in tumors of the central nervous system (CNS), head and neck (orbits, paranasal sinuses, and skull base), and skeletal sites to determine and distinguish disease from inflammatory response. Thin CT slices (2 to 3 mm) with IV contrast are also recommended for treatment planning CT to assist in nodal and soft-tissue target delineation. IGRT for verification of accurate delivery of planned dose allows for smaller volume expansion and steeper dose gradients and is recommended for sites where critical organs at risk are in close proximity to the planning target volume, including mediastinum and head and neck regions. Adaptive IGRT with real time shifts are used when there are large changes anticipated in the anatomy or when small changes will result in significant impact on dose distribution.
HL may present as limited or advanced-stage disease. Limited stage is typically further categorized into favorable and unfavorable prognostic groups. Table 95.1 summarizes the definition of favorable-prognosis disease, according to the German Hodgkin Study Group (GHSG) and European Organization for Research and Treatment of Cancer (EORTC) (see the box with Case 1 ).
| GHSG | EORTC | |
|---|---|---|
| Age | — | <50 |
| Histology | — | — |
| Erythrocyte Sedimentation Rate (ESR)/B Symptoms |
|
|
| Large Mediastinal Adenopathy (LMA) | No | No |
| Extranodal Lesions | None | — |
| Number of Sites | <3 | <4 |
Table 95.2 summarizes the results of the GHSG HD10 and HD11 trials, conducted prior to the incorporation of FDG-PET in guiding treatment decisions. These two trials evaluated treatment de-escalation for early-stage, low-risk, and high-risk patients, respectively. The GHSG HD10 compared 4 versus 2 cycles of adriamycin, bleomycin, vinblastine, and dacarbazine (ABVD), followed by 30 versus 20 Gy IFRT. At a median follow-up of 98 months, no differences occurred in freedom from treatment failure (FFTF) and OS among the four arms, leading to a recommendation of 20 Gy after 2 cycles of ABVD in patients with limited stage, low-risk HL. The GHSG HD11 trial compared 4 cycles of ABVD versus 4 cycles of baseline bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone (baseline BEACOPP), followed by 20 Gy versus 30 Gy of IFRT. At a median follow-up of 106 months, there were no differences in outcome between 20 Gy versus 30 Gy after BEACOPP, but inferiority of 20 Gy after 4 cycles of ABVD could not be excluded. A radiation dose of 30 Gy therefore remains the standard in limited stage, unfavorable HL, after ABVD chemotherapy.
| GHSG HD10 | GHSG HD11 | |
|---|---|---|
| Number of Patients | 1370 | 1395 |
| Patient Characteristics | Low risk: 1–2 sites, non-bulky, no E-lesions, ESR <50 or <30 with B symptoms | High risk: ≥ 3 sites, bulky med, E-lesions or ESR >50 or >30 with B symptoms |
| Treatment Arms |
|
|
| Median Follow-Up | 90 months | 82 months |
| 8-year Freedom from Tumor Failure (FFTF) |
|
|
| 8-year Overall Survival (OS) |
|
|
| 10-year Progression Free Survival (PFS) |
|
|
More recent trials have explored using PET-guided response to chemotherapy to further de-escalate or escalate therapy. Table 95.3 summarizes results of these trials, focusing on the elimination of RT, based on PET-guided response or early PET-response to chemotherapy. The RAPID trial compared combined modality therapy with chemotherapy alone in stage I-IIA non-bulky patients with complete PET-response (Deauville 1–2) after 3 cycles of ABVD. At a median follow-up time of 60 months, by intent-to-treat analysis, the 3-year, progression-free survival (PFS) rate was 94.6% in the RT group and 90.8% in the non-RT group ( P = .16). Although the difference was not statistically significant, the pre-specified, non-inferiority margin of 7% points was not met and hence, non-inferiority of chemotherapy alone could not be concluded. Moreover, by per-protocol analysis, after excluding patients who were randomized to the RT arm but did not receive the treatment, there was a significant difference between the arms in favor of RT (3-year PFS 97.1% vs. 90.8%, P = .02). The EORTC/LYSA/FIL H10 trial examined adapting therapy in early-stage patients, according to early PET response to ABVD. For patients with favorable prognosis disease who achieved early complete PET response to ABVD, the 5-year PFS of the combined modality therapy arm was significantly higher than that of the chemotherapy alone arm (99%, vs. 87.1%). For patients with unfavorable prognosis disease, the corresponding 5-year PFS of the two arms were 92.1% and 89.6%, respectively. The difference was not significant but the pre-specified, non-inferiority margin was not met; hence, non-inferiority of chemotherapy alone could not be concluded. For patients with interim PET-positive disease, compared to the standard arm of ABVD followed by INRT, the 5-year PFS of intensifying therapy to dose-escalated BEACOPP or BEACOPP-14 followed by INRT was significantly higher (90.6% vs. 77.8%). However, escalating treatment to BEACOPP was associated with significantly higher rates of grade 3 and 4 hematologic toxicities. The GHSG HD16 trial randomized limited-stage, low-risk HL to 2 cycles of ABVD followed by 20 Gy IFRT, versus the PET-guided treatment arm of 2 cycles of ABVD, with omission of RT if PET negativity was attained after chemotherapy. At a median follow-up time of 45 months, among patients with PET-negative scan at the end of chemotherapy, 5-year PFS was 93.4% for the RT arm and 86.1% for the non-RT arm, leading to the conclusion, similar to the RAPID and EORTC/LYSA/FIL H10 trials, that RT cannot be safely eliminated despite complete PET response to ABVD chemotherapy. The GHSG HD17 trial randomized limited-stage, high-risk HL patients to 2 cycles of escalated BEACOPP and 2 cycles of ABVD, followed by 30 Gy IFRT, versus the PET-guided treatment arm of the same chemotherapy, with omission of RT if PET negative after the chemotherapy and 30 Gy INRT if PET positive. At a median follow-up time of 46 months, the 5-year PFS of the standard arm of combined modality therapy was 97.3% versus 95.1% in the PET-directed therapy arm, demonstrating non-inferiority for the PET-stratified treatment approach. This is the first randomized trial in early-stage HL that showed that RT can be eliminated if complete response to chemotherapy, though the chemotherapy that was used included escalated BEACOPP, which is not a commonly used regimen, especially among early-stage patients in the United States. Of note, the GHSG HD17 is also the first study comparing INRT with IFRT in a prospective randomized fashion.
| RAPID | EORTC/GELA/FIL | GHSG HD16 | GHSG HD17 | ||
|---|---|---|---|---|---|
| H10F | H10U | ||||
| Number of Patients | 420 | 551 | 594 | 628 | 1100 |
| Patient Characteristics | Stage I-IIA, non-bulky | Favorable per EORTC | Unfavorable per EORTC | Favorable per GHSG | Unfavorable per GHSG |
| PET Negative Definition | Deauville 1–2 | ≤ Mediastinal blood pool level | Deauville 1–2 | Deauville 1–2 | |
| Chemo Alone | ABVD × 3 | ABVD × 4 | ABVD × 6 | ABVD × 2 | eBEACOPP × 2, ABVD × 2 |
| 5 y PFSPer - Protocol |
|
87% | 89.6% | 86.1% | 95.1% |
| Combined Modality Therapy | ABVD × 3 + RT | ABVD × 3 + RT | ABVD × 4 + RT | ABVD × 2 + RT | eBEACOPP × 2, ABVD × 2 + RT |
| 5 y PFSPer-Protocol |
|
99% | 92.1% | 93.4% | 97.3% |
The role of RT for patients with advanced-stage HL is less well defined. The GHSG HD12 trial is a four-arm study for patients with bulky-stage IIB and stages III-IV disease, comparing two different BEACOPP variants with or without RT. Among the patients with initial bulky disease (>5 cm) or residual disease after chemotherapy (>1.5 cm), patients randomized to the non-RT arm had a significantly inferior 10-year PFS in comparison to patients on the RT arm (83.5% vs. 88.6%). In the subgroup of patients with residual disease (>1.5 cm), patients on the non-RT arm had both a significantly inferior PFS (83.4% vs. 89.7%) and OS (88.4% vs. 94.4%). Using PET-guided response to chemotherapy for RT decision in advanced HL was addressed in several trials. In the GHSG HD15 trial, after dose-escalated BEACOPP and its variants, RT was limited to patients with residual disease of 2.5 cm and with residual PET avidity. The 4-year PFS in patients with complete response or those with PET-negative disease/partial response, after chemotherapy and non-RT, were 92.6% and 92.1%, respectively, showing that in patients with complete metabolic response to BEACOPP, excellent results can be achieved without RT. In the GITIL/FIL HD 0607 trial, patients with a negative PET scan after 2 cycles of ABVD continued on to a total of 6 cycles of ABVD; those with a large nodal mass at diagnosis (≥ 5 cm), who continued to be PET-negative, were randomly assigned to RT or no further treatment. At a median follow-up of 3.6 years, there was no difference in 3-year PFS between the two arms (97% vs. 93%; P = .29). When the analysis was limited to the subgroup of patients with large nodal mass of greater than 10 cm, the 3-year PFS rates were 94% versus 86% ( P = .34), although the comparison in this subgroup may be limited by inadequate power. Routine addition of RT, after chemotherapy, in patients with advanced-stage HL is not supported by available data but should be considered in patients who lack complete metabolic response to modern chemotherapy.
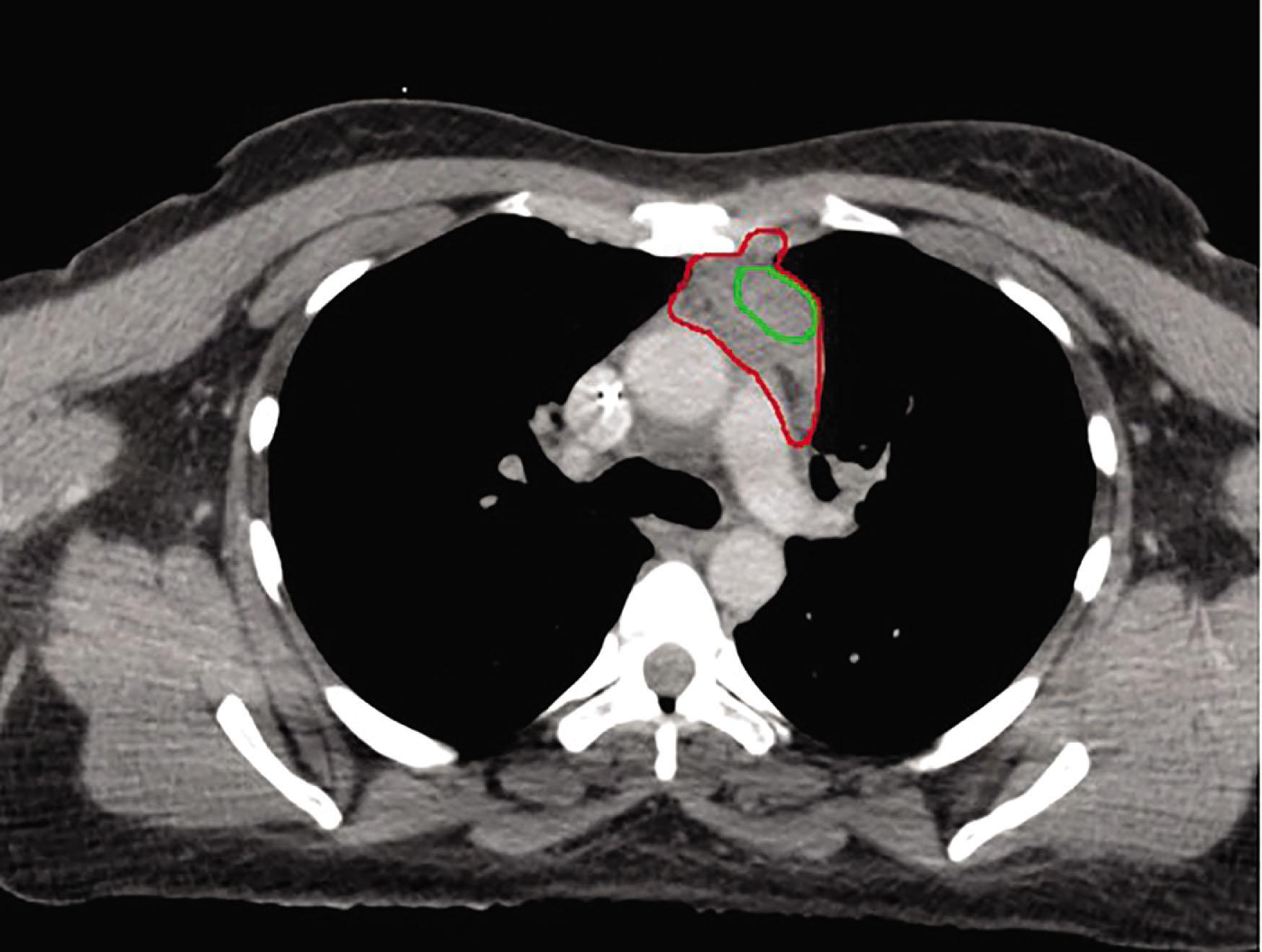
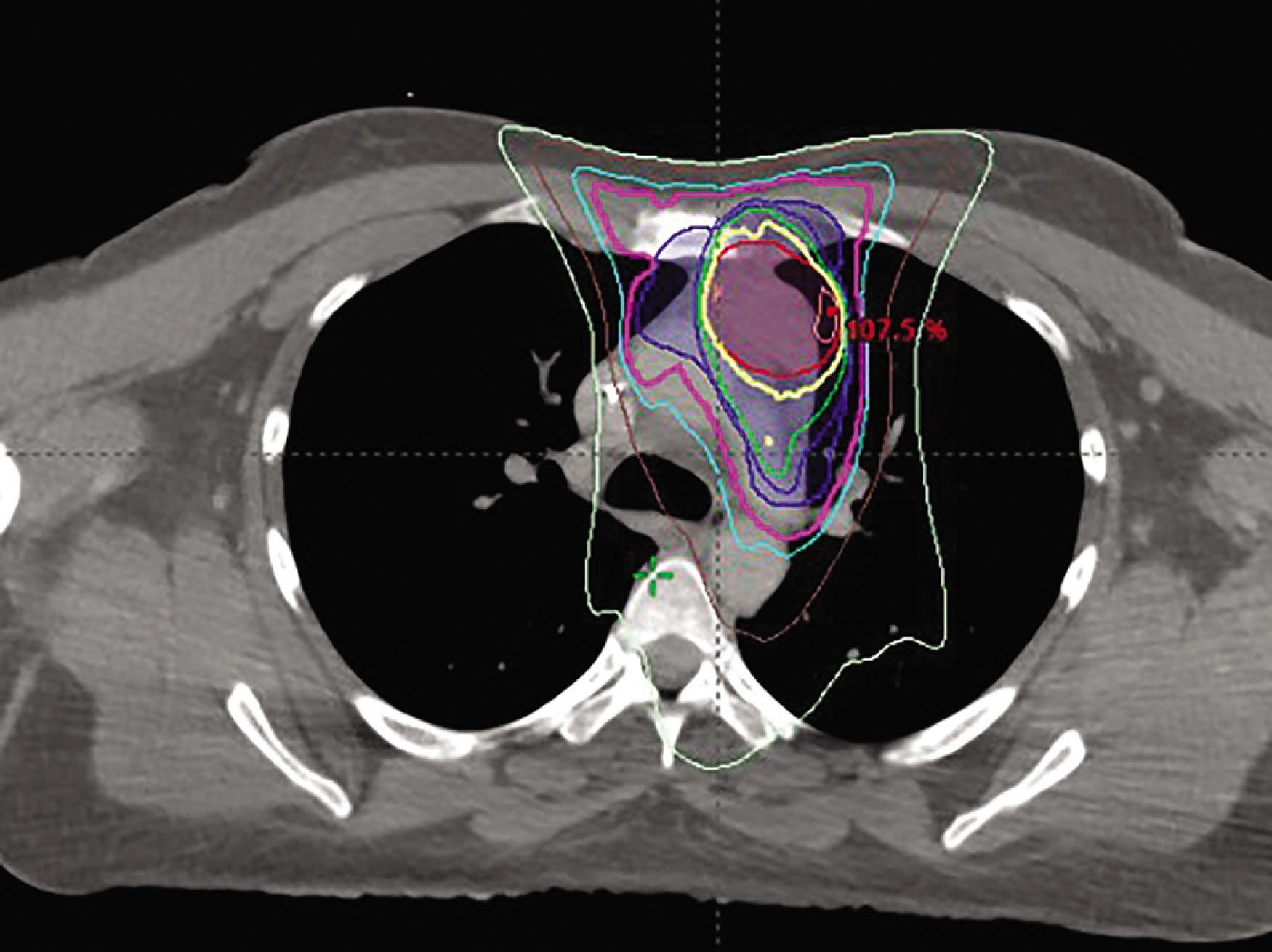
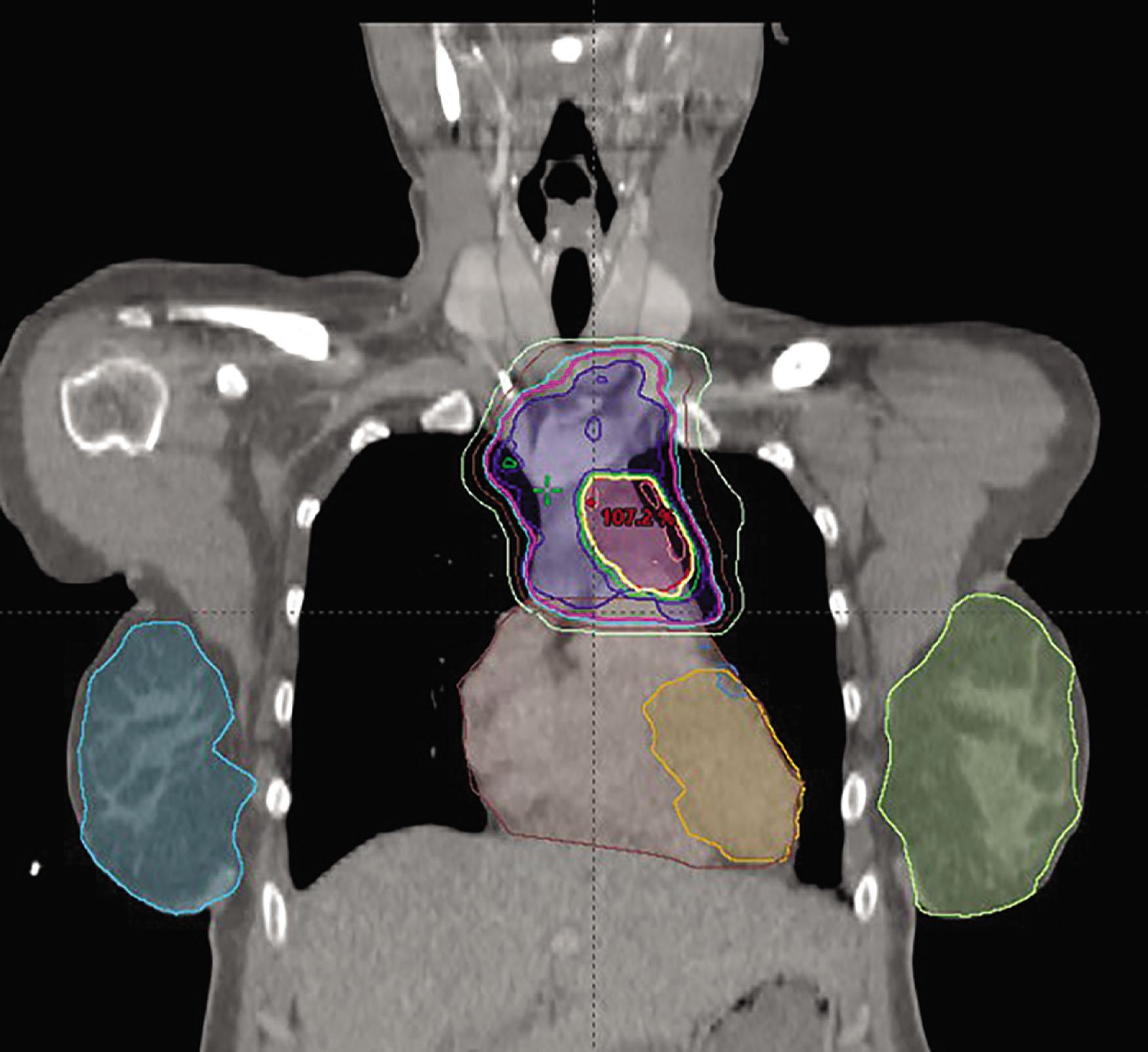
A 28-year-old female with classic Hodgkin lymphoma with Deauville 4 response to chemotherapy:
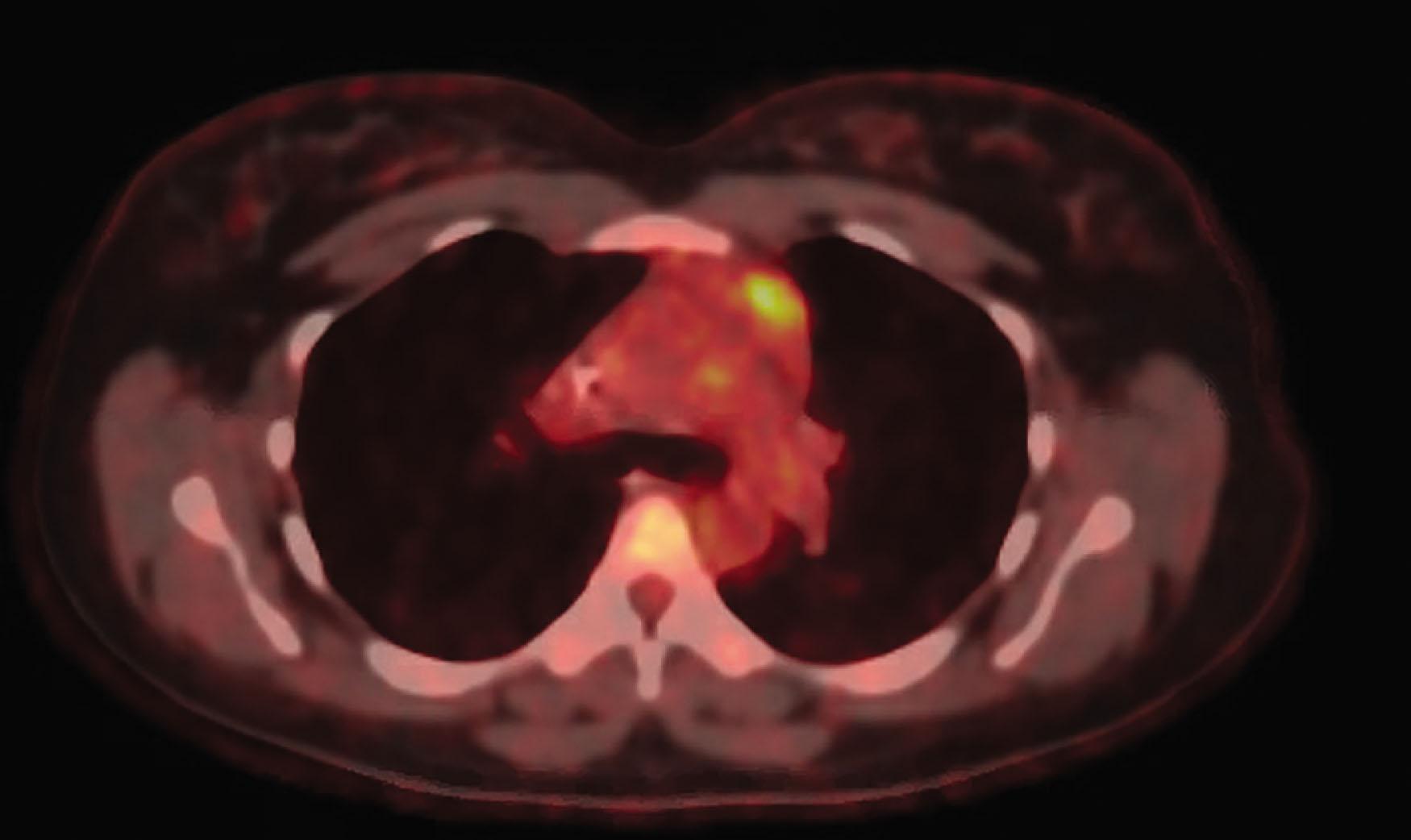
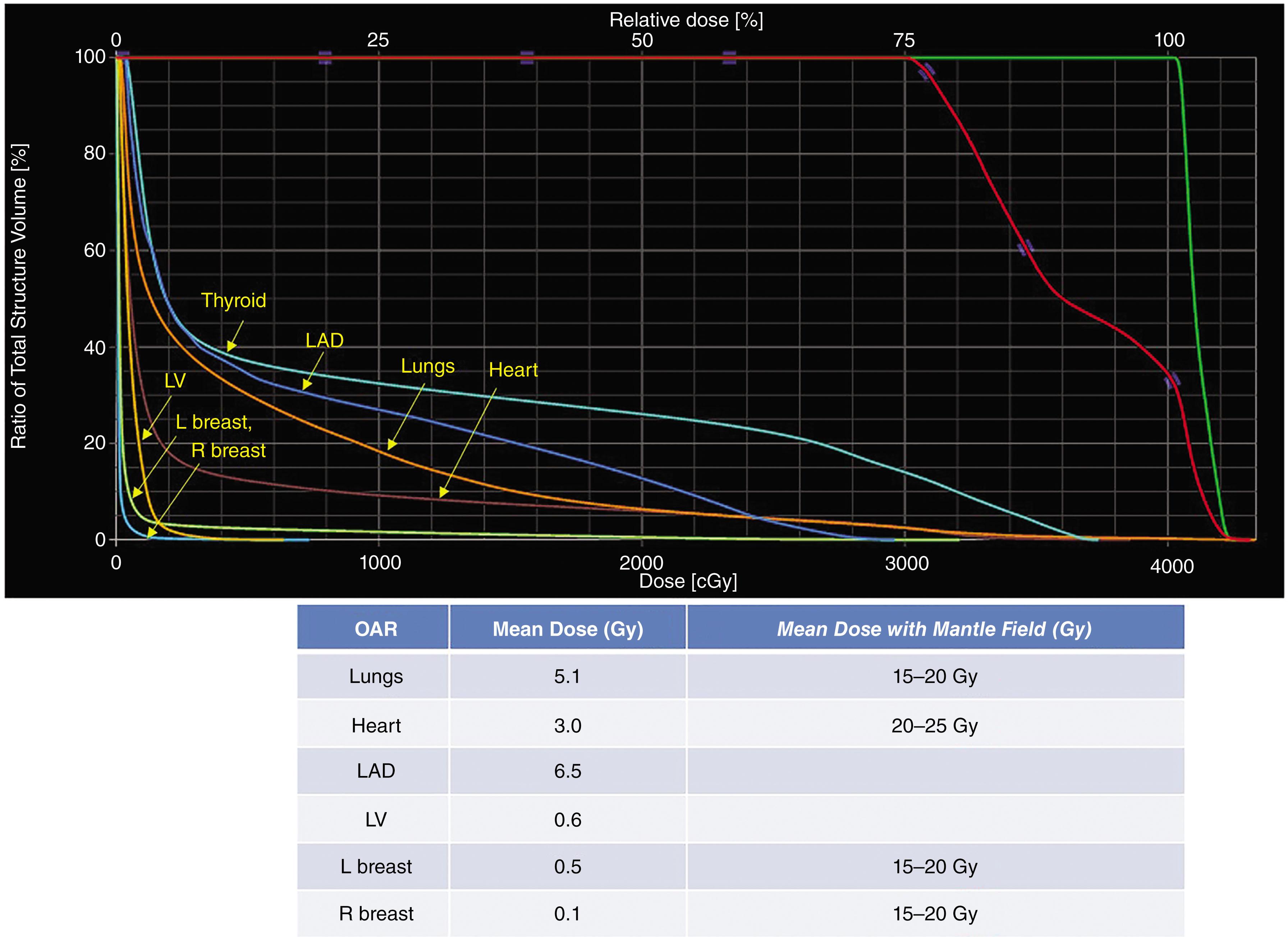
The patient received involved site radiation therapy (ISRT) to 30 Gy (in 1.5 Gy per fraction, CTV_30 contoured in red) with simultaneous integrated boost to residual fluorodeoxyglucose avid site to 40 Gy (in 2 Gy per fraction, CTV_40 contoured in green). Patient was planned in arms down position on 10-degree incline board to displace breast tissue inferiorly. Intensity modulated radiation therapy (IMRT) with butterfly technique was used (limiting arcs to narrow angles anteriorly and posteriorly to reduce low-dose bath to breasts and lungs):
Dose-volume histogram showing doses to organs-at-risk (OAR), and summary table comparing mean doses to OAR with this current ISRT, compared to the typical mean doses to the same OAR in a historical mantle field:
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here