Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

“Patient safety” refers to the healthcare discipline that strives to reduce the risk of medical errors and harm to patients receiving medical care. The World Health Organization (WHO) estimates that adverse events due to unsafe medical care is one of the top ten causes of death and disability in the world. Adverse events in healthcare affects patients in low- and high-income countries alike, as a systematic review of medical errors in high-income countries found that 9.2% of patients suffer in-hospital adverse events and that over 43% of these events were preventable. According to the WHO, the most concerning areas of patient safety include medication errors, healthcare-associated infections, unsafe surgical care procedures, unsafe injections practices, diagnostic errors, unsafe transfusion practices, radiation errors, sepsis, and venous thromboembolism.
In the US, the landmark report To Err Is Human: Building a Safer Health System was published by the Institute of Medicine (IOM) in 2000, and it highlighted the startling magnitude of adverse events in healthcare and also framed the occurrence of these events as resulting from systems that fail to prevent them rather than blaming individuals. Focus on the occurrence of adverse events during medical care has remained in the spotlight since the publication of the IOM report, propelled by groups such as The Leapfrog Group. The Leapfrog Group is a national watchdog organization in the US that was founded 20 years ago. It publishes an annual report that assigns safety grades to over 2700 hospitals. In 2019, The Leapfrog Group launched its Ambulatory Surgery Center Survey, after noting that over 60% of surgeries in the US are performed in hospital outpatient units or ambulatory surgical centers (ASCs). Furthermore, a hospital’s incidence of adverse events and its efforts to prevent medical errors are used to not only try to inform consumers of healthcare, such as patients and employers, but are also now tied to reimbursement. In the fee-for-service model, reimbursement was tied only to the quantity of services provided. In the past 5 years, payment has been increasingly tied to the value of services, which is termed value-based care. The most notable example of this is the Centers for Medicare & Medicaid Services (CMS) Hospital-Acquired Condition Reduction Program (HACRP), which aimed to improve healthcare quality in the inpatient setting. Beginning in 2015, hospitals that ranked in the worst-performing 25% of hospitals on measures of hospital-acquired conditions had their CMS payments reduced by 1%.
Although the patient population undergoing plastic surgery procedures is generally healthier than in some other surgical subspecialties, adverse events still occur with some regularity. Hernando-Boussard and colleagues used the 2005–2009 Nationwide Inpatient Sample database (NIS) of over 400,000 patient records to identify postoperative adverse events in patients who underwent a soft tissue reconstruction during an inpatient stay. The authors found a 4.06% overall rate of adverse events, with a higher rate amongst patients undergoing pedicled grafts or flaps (5.08%) and a lower rate among breast reconstruction patients (1.97%). This chapter focuses on many of the most important patient safety topics within the field of plastic surgery, and these are organized temporally according to preoperative, intra-operative, and postoperative settings.
The American Society of Anesthesiologist (ASA) physical status classification system was devised in 1941. This system has evolved over the intervening decades and presently includes six ASA physical status classes (see Table 9.1 ). ASA physical status has been shown to be predictive of perioperative risk in the inpatient setting. In addition, a recent study by Foley and colleagues determined that ASA physical status class was predictive of morbidity and mortality following outpatient surgery. Foley et al . examined medical and surgical complications in over 2 million patients who had ambulatory surgery using the 2006 through 2015 NSQIP data sets. They found that ASA physical status class predicts medical complications, readmission, and mortality across various surgical specialties, including an 89-fold increase in mortality in ASA physical status class IV patients compared with class I patients. ASA physical status correlates with anesthesia-related perioperative mortality, as demonstrated by Lagasse, who found 0 deaths in 8210 ASA Class I patients versus 71 deaths among 273 Class V patients (a 26% mortality rate). Therefore, to optimize patient safety, plastic surgeons ought to consider ASA physical status during preoperative consultations, both to assess the appropriateness of surgery and also to estimate risk of complications during the informed consent process.
| ASA I | Normal healthy patient without active disease |
| ASA II | Patient with mild systemic disease (e.g., hypertension under medical control) |
| ASA III | Patient with severe systemic disease |
| ASA IV | Patient with severe systemic disease that is a constant threat to life |
| ASA V | Patient who is moribund and is not expected to survive without surgery |
| ASA VI | Patient who has been declared brain-dead for organ donation |
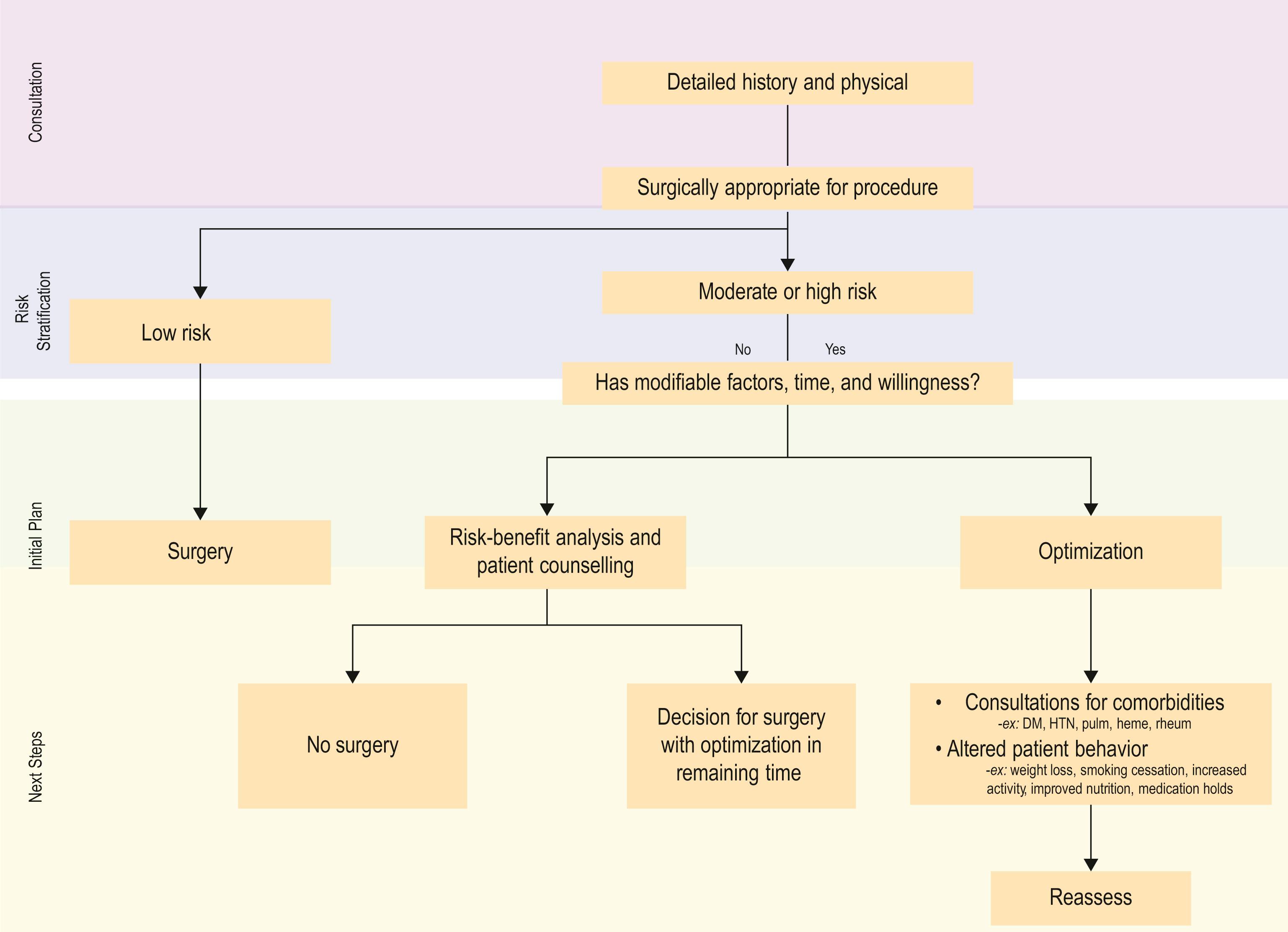
Providing safe care to the plastic surgery patient is contingent upon careful risk stratification and optimization of the patient preoperatively. A thorough history and physical allows determination of whether a patient is of acceptable or prohibitive surgical risk, although admittedly criteria for declining a patient for surgery vary widely among surgeons. Once a patient is deemed an appropriate candidate for surgery, optimization of existing medical conditions should occur with guidance from primary care providers and/or specialists. Optimization of glycemic control in diabetic patients, blood pressure control in hypertensive patients, and pulmonary function in patients with chronic obstructive pulmonary disease (COPD) are classic examples. Algorithm 9.1 outlined in this chapter puts forth a simple approach towards preoperative stratification and optimization.
Risk for venous thromboembolism (VTE) cannot necessarily be seen, which underscores the importance of patient-centric risk stratification through history and physical exam. The 2005 Caprini score is a widely validated VTE risk stratification tool that is formally recommended by the American Society of Plastic Surgeons and the American College of Chest Physicians. The tool creates an aggregate risk score based on the presence or absence of some 40 individual risk factors.
Individualized VTE risk stratification, and in particular using the 2005 Caprini score, assists the clinician to optimize VTE risk in the preoperative setting in several ways. These include:
Risk modification . Completion of the score can identify risk factors that are potentially modifiable prior to surgery, especially elective surgery. For example, the score may identify breast cancer patients with existing but unneeded chemo-ports, may identify oral contraceptive use and prompt a discussion about perioperative cessation (see below), or identify a strong family history (commonly missed, and present in 10–15% of plastic surgery inpatients ) that can be further evaluated.
Decision to refer for additional consultation . The score may identify patients with strong family history of VTE, or in women a history of ≥3 lost pregnancies. Each can be a marker of undiagnosed genetic hypercoagulability. Hypercoagulability panels can be more difficult to interpret amongst patients who recently received prophylactic anticoagulation. Thus, at surgeon discretion, and especially for the elective population, potentially high-risk patients may be referred for hematology consultation.
Assignment of percentage risk . For plastic surgery inpatients, the Caprini score identifies an approximately 20-fold variation in VTE risk (ranging from 0.3% to 8.5%) among the overall population. This allows surgeons to have a data-driven discussion with patients about baseline risk, and also to discuss opportunities for risk reduction, as described below.
Especially for elective surgery, consideration of VTE risk at the initial preoperative visit allows risk to be pre-emptively minimized or further evaluated. Importantly, an early consideration of VTE risk allows the surgeon to actively discuss candidacy for surgery with higher-risk elective patients.
Chronically anticoagulated patients (such as those with atrial fibrillation) require anticoagulation cessation for procedures. For these patients, level I evidence from the BRIDGE trial supports warfarin cessation 5 days prior to the procedure and re-initiation 24 hours after surgery or at surgeon discretion. Bridging therapy with low molecular weight heparin did not significantly reduce arterial thromboembolism (0.3% vs. 0.4%) but did increase major bleeding (3.2% vs. 1.3%). Thus, bridging therapy should not routinely be performed.
For cardiovascular drugs, including but not limited to antiplatelet agents, beta-blockers, and antihypertensives such as ACE inhibitors, optimal perioperative management should be undertaken in concert with the patient’s cardiovascular providers. Existing recommendations generally support continuation of drugs already being taken by patients in the perioperative period, but support a multispecialty conversation to understand the risks and benefits of medication continuation or cessation. For patients at high risk of cardiovascular morbidity, some therapies, including beta-blockade and statins, can be initiated prior to surgery, again guided by clinical circumstances. The perioperative management of cardiovascular drugs is well beyond the scope of this article. However, excellent guidance is available from regularly updated guidelines co-published by the American College of Cardiology and the American Heart Association.
Oral contraceptives and hormone replacement therapy are known to increase risk for blood clots, both at baseline and in surgical patients. Other outside sources of hormones like intrauterine devices (IUDs) and vaginal rings should also be considered. Discontinuation of exogenous sources of hormones for 3 weeks before and 3 weeks after surgery can allow risk to return to normal levels. However, discontinuation of oral contraception can have unintended consequence, including menstrual period irregularity or unintended pregnancy. Similarly, discontinuation of hormone replacement can promote hot flashes and other symptoms. For IUDs, women may discuss removal or exchange for a non-hormone IUD (copper IUD) with their gynecologic provider. VTE risk, including risk modification, is important to discuss with all patients. Engaging patients, especially low-risk patients, in an explicit discussion of the risks and benefits of oral contraception or exogenous hormone discontinuation is important and appropriate.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here