Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

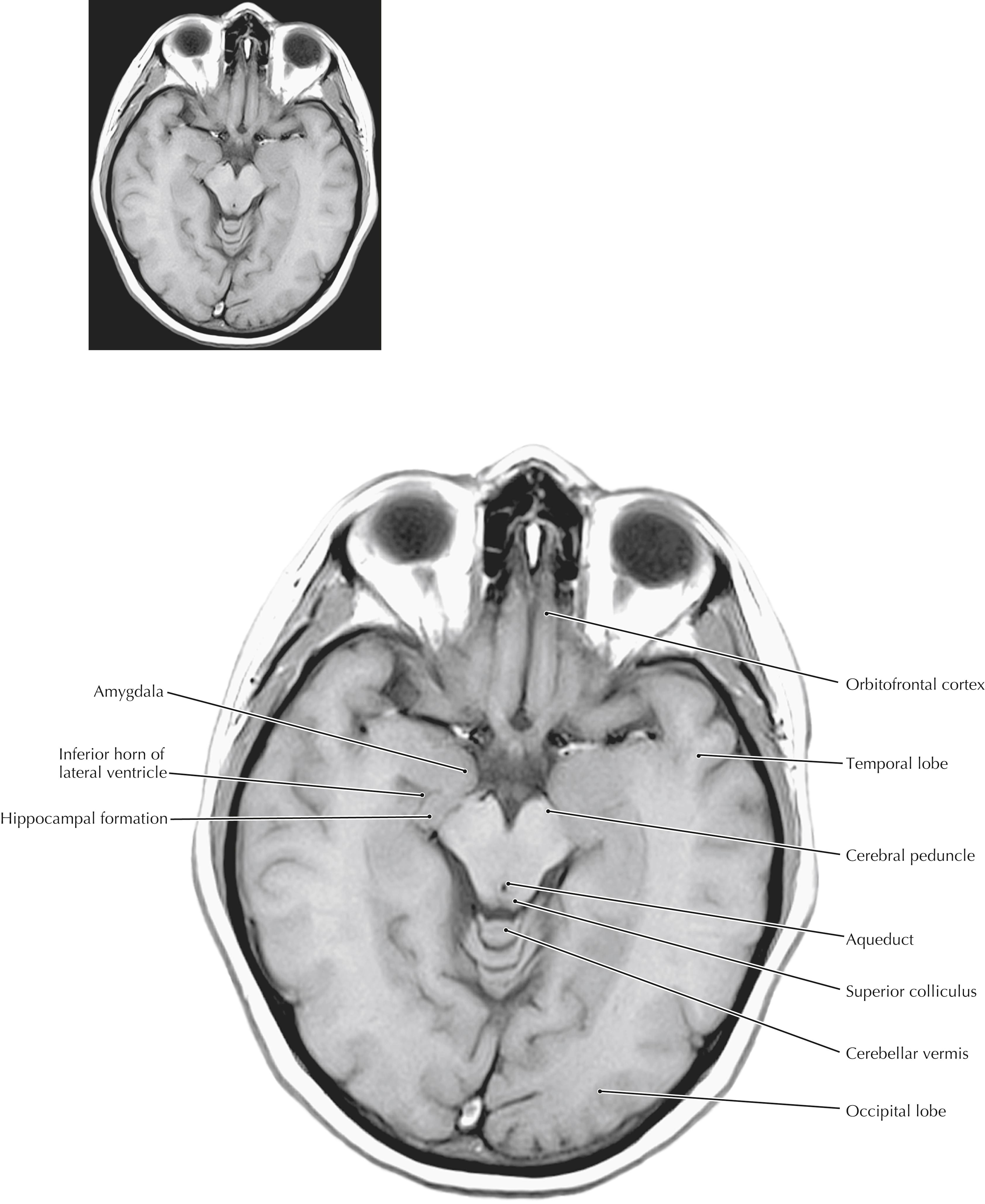
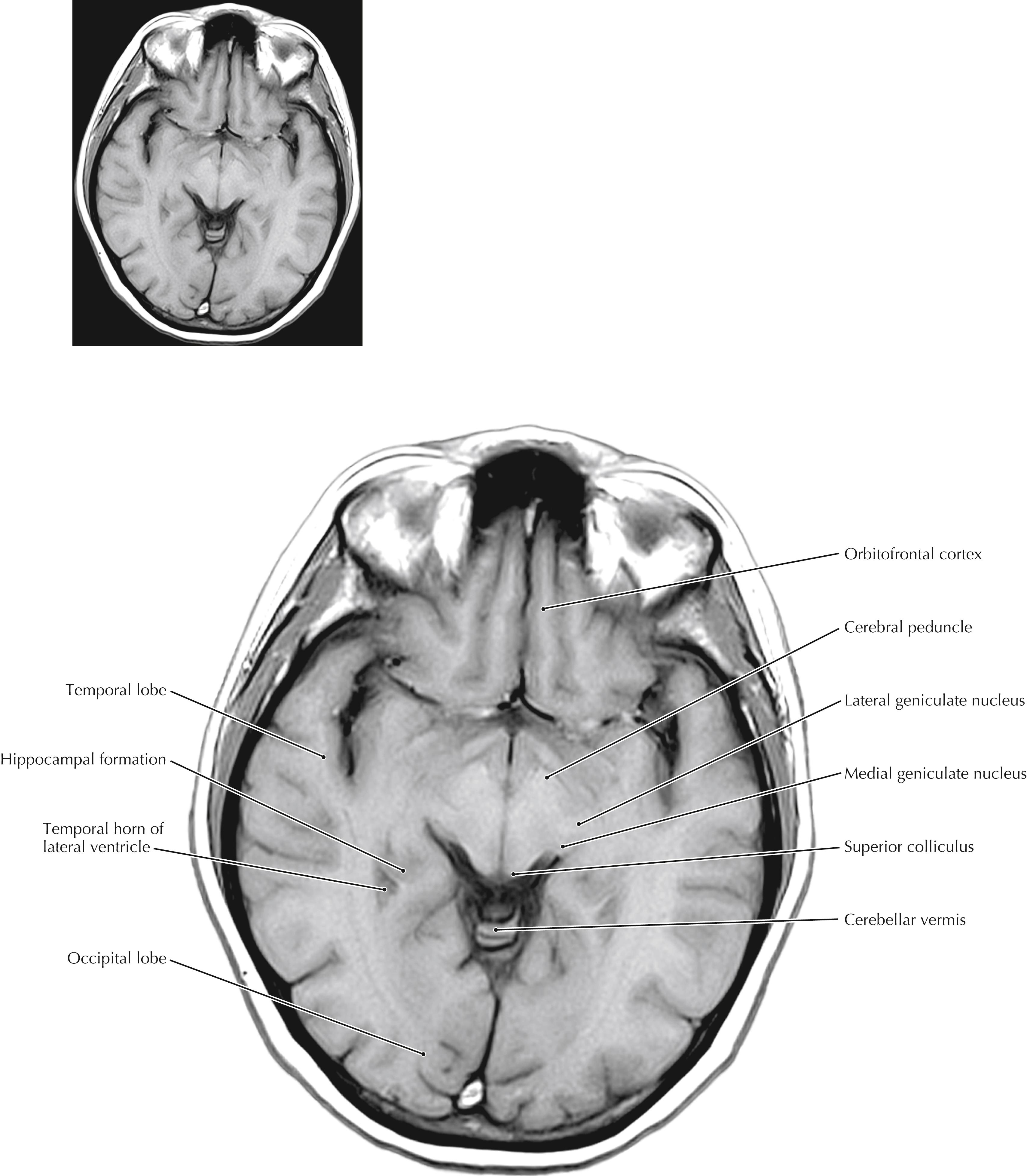
These axial (horizontal) sections compare anatomical sections and high-resolution magnetic resonance (MR) images. They are cut in the true horizontal (axial) plane, not in the older 25-degree tilt. The most important anatomical relationships in these sections center on the internal capsule (IC). The head of the caudate nucleus is medial to the anterior limb of the IC and forms the lateral margin of the frontal pole of the lateral ventricle. The thalamus is medial to the posterior limb of the IC. The globus pallidus and putamen are lateral to the wedge-shaped IC. The posterior limb of the IC carries the major descending corticospinal, corticorubral, and corticoreticular fibers and the ascending sensory fibers of the somatosensory and trigeminal systems. The most posterior portions of the posterior limb also carry the auditory and visual projections to their respective cortices. The genu of the IC carries the corticobulbar fibers. The anterior limb of the IC carries cortical projections to the striatum and the pontine nuclei (pontocerebellar system). The full-plate MR images are T1-weighted; the ventricles appear dark. The scout MR images that accompany the drawings are T2-weighted MR images, in which the cerebrospinal fluid (CSF) appears white.




The temporal lobe includes the amygdaloid nuclei, the hippocampal formation and associated cortex, the transverse gyrus of Heschl, some language-associated cortical regions (Wernicke’s area in the dominant hemisphere), Meyer’s loop of geniculocalcarine axons, the inferior horn of the lateral ventricle, and extensive cortical areas (superior, middle, and inferior temporal gyri). The temporal lobe can be damaged by trauma, infarcts, tumors, abscesses, and other pathological conditions. Such damage can result in auditory hallucinations, delirium and psychotic behavior, sometimes a contralateral upper quadrantanopia (if Meyer’s loop is damaged), and receptive aphasia (Wernicke’s aphasia) that involves a lack of understanding of verbal information (in a lesion of the dominant hemisphere). Some very specific lesions in the temporal lobe result in an agnosia for recognition of faces (prosopagnosia).


The basal ganglia assist the cerebral cortex in planning and generating desired programs of activity and suppressing undesired programs of activity. The most conspicuous arena in which these functions are observed is motor activity. Basal ganglia disorders produce movement problems that are often involuntary in nature and are commonly accompanied by cognitive and affective symptoms (e.g., Huntington’s disease). The principal route of information flow from the basal ganglia is from the thalamus and cerebral cortex to the striatum (caudate nucleus and putamen), then to the globus pallidus, then back to the thalamus and cortex, completing the loop. Disruption of this loop can produce excessive movements (e.g., choreiform and athetoid movements, tremor) or diminished movements (bradykinesia). In some instances, specific nuclei are known to be associated with such changes. A small lacunar infarct in the subthalamic nucleus results in wild, flinging (ballistic) movements in the contralateral limbs. However, a surgical lesion in the subthalamic nucleus may ameliorate some of the movement problems seen in Parkinson’s disease. The subthalamus most likely drives activity in the internal segment of the globus pallidus, which in turn can be modified by the external segment. A pathological lesion in the globus pallidus can produce rigidity and akinesia; a surgical pallidal lesion may reduce excessive movements in other basal ganglia disorders.

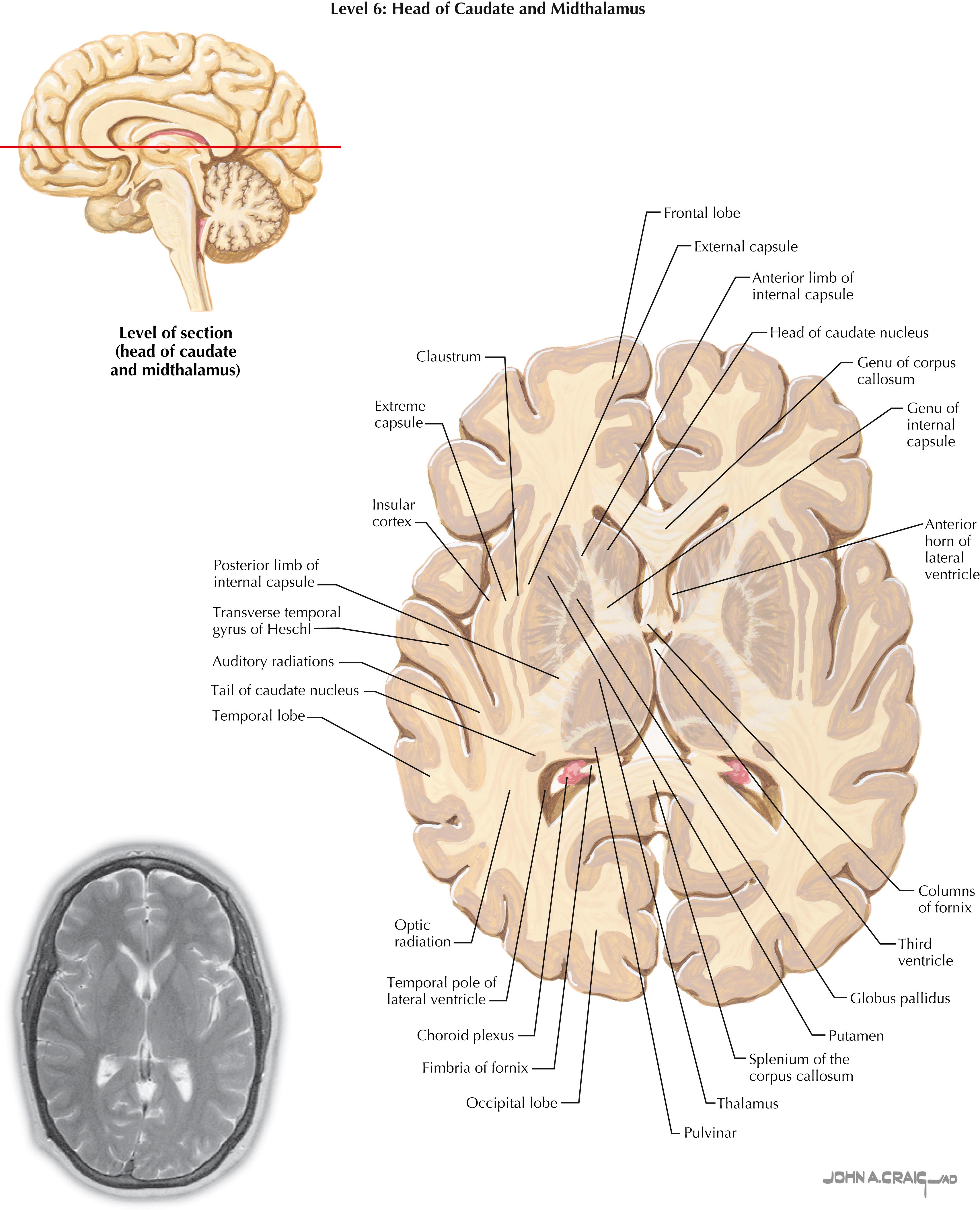


Huntington’s disease is an autosomal dominant disorder caused by a trinucleotide repeat (CAG) on the short arm of chromosome 4. It results in a progressive, untreatable disease that includes a movement disorder (choreiform movements: brisk, jerky, forcible, arrhythmic movements), progressive cognitive impairment, and affective disorders (such as depression, psychotic behavior). This disease progresses from a state of minor impairment (clumsiness) with minor behavioral problems (irritability and depression) to major impairment, dementia, and a decline that leads to incapacitation and ultimately to an early death. The anatomical hallmark of this disease is marked degeneration of the caudate nucleus (also the putamen). The characteristic bulge of the head of the caudate into the frontal pole of the lateral ventricle is lost. Most of the medium spiny caudate neurons that project to the globus pallidus degenerate as the result of damage from excess Ca 2+ influx caused by glutamate excitotoxic damage via activation of the N-methyl-D-aspartate (NMDA) receptors. The intrinsic cholinergic interneurons of the striatum also degenerate in Huntington’s disease.







Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here