Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

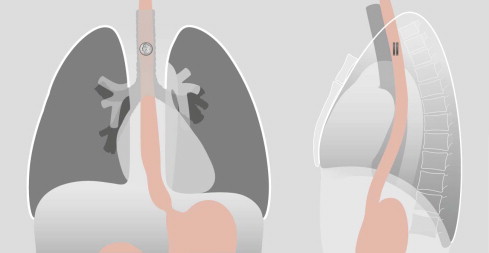
Coins may lodge in the oesophagus—slightly dangerous.
The CXR must include the neck.
Button batteries may lodge in the oesophagus—highly dangerous.
The halo sign is important.
Two magnets in the bowel—highly dangerous.
Use of a compass may be crucial.
X-ray machine.
Hand held metal detector.
A compass.
CT Scanner.
AXR, abdominal radiograph;
BB, button battery;
CXR, chest radiograph;
ED, Emergency Department;
FB, foreign body;
HHMD, hand held metal detector.
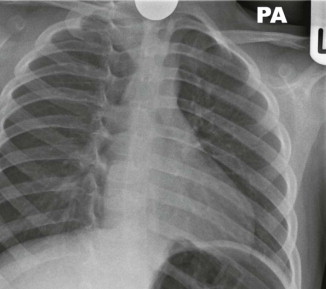
An AP chest radiograph (CXR) to include all of the neck below the angle of the mandible.
An abdominal radiograph (AXR) is not indicated .
Occasionally, a coin will lodge in the oesophagus. Some of these patients will be asymptomatic. An unrecognised coin can cause clinical problems including erosion of the mucosa which may result in an abscess or mediastinitis . It is important to confirm that any swallowed coin has passed beyond the oesophagus. If the CXR is clear then the parents can be reassured that the coin will be passed within a few days.
Does the stool need to be checked? Sometimes a coin will be overlooked in the stool; the parents would be better advised to return to the Emergency Department (ED) only if the child becomes symptomatic.
Coin composition: coins in the UK and in the European Union are made of steel or alloys of various metals and sometimes coated with copper. In effect, these coins are inert. This does not apply worldwide. For example, in 1982 because of the cost of copper the one cent coin in the USA (commonly referred to as the penny) was minted with a mainly zinc core and a thin copper coating. Interaction between gastric acid and zinc can cause ulceration in the stomach. This possibility led to various scares and the consequent overuse of routine AXR. The penny constituents were not changed, but eventually a practical recommendation was made and widely adopted: if a USA penny has been swallowed and the CXR is clear then an AXR need only be obtained in a child who subsequently developes intestinal symptoms. The latter is an exceptionally rare occurrence.
Consider this as an alternative to radiography. Advantages of a HHMD include:
It eliminates the need for a CXR.
There is no ionizing radiation.
It is accurate and easy to use with minimal training.
Patient and parent time spent in the ED is reduced.
It is cost effective.
Its efficacy is underpinned by a tried and tested diagnostic algorithm.
Pitfall. If using a HHMD, a definite history in relation to the swallowed foreign body being a coin is most important. If the history is uncertain and the foreign body could be a magnet or a cluster of magnets (see p. 359 ) then a false reassurance might be provided by the HHMD. A safety net: concern regarding a cluster of magnets masquerading as a swallowed coin can be eliminated by passing a compass over the abdomen . The lack of compass movement will exclude a magnet.
Pitfall (2). The majority of retained coins are situated in the upper oesophagus at the level of the cricopharyngeus muscle. An impacted coin can be missed if the whole neck below the level of the angle of the mandible is not included on the CXR.
Fish bones comprise more than 70% of all foreign body events that cause an attendance to some EDs . Complications resulting from an impacted fish bone are rare but can be serious. These include: neck abscess, mediastinitis and lung abscess.
Fish bone impaction is very different to that of other impacted foreign bodies .
Infrahyoid impaction is much less frequent. In one series approximately 90% of fish bones were situated in the oro-pharynx, whereas approximately 90% of other foreign bodies (poultry bones, dentures, wood splinters, coins, pork bones and lamb bones) were impacted more distally in the laryngeal pharynx or upper oesophagus.
Radiography.
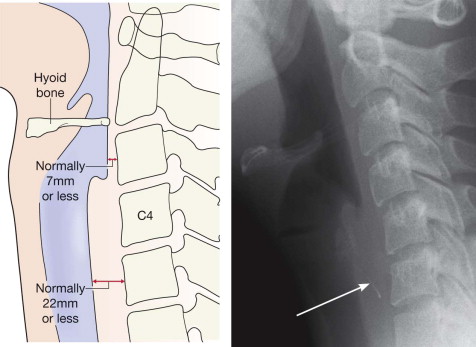
The soft tissues of the oro-pharynx and down to the level of the hyoid bone are dense on the lateral radiograph. A lateral neck radiograph will rarely detect a fish bone impacted in these dense areas.
The use of a lateral radiograph of the neck should be limited, selectively employed, and based on a diagnostic algorithm (see p. 353 ).
What to look for.
The occasional fish bone that does impact below the hyoid bone.
Evidence of a complication:
Gas in the soft tissues, either as a streak or as a pocket, suggests perforation.
Widening of the prevertebral soft tissues suggests an abscess.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here