Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

 Access video content for this chapter online at Elsevier eBooks+
Access video content for this chapter online at Elsevier eBooks+
Identifying and treating secondary cleft lip and palate deformities is a challenging endeavor for even the most experienced surgeon. Proper diagnosis involves an understanding of previous operations as well as a thorough physical examination. Surgical timing depends on deformity severity, age of patient, and understanding and willingness of family members.
Children born with clefts of the lip and palate should ideally be cared for by a multidisciplinary cleft team who adhere to the international standards set forth by the American Cleft Palate and Craniofacial Association. The standards set forth by this organization provide for the proper care and follow-up required to achieve successful long-term outcomes. Occasionally, children do not have access to these teams, and their care is performed outside of this standard. If these children are initially treated elsewhere and are referred into a team, there can be secondary deformities related to their initial treatment.
A thorough history, including an understanding of all previous interventions, must be obtained. Often, knowing where the operations occurred will help to understand what was previously done. Many parents are not familiar with repair techniques, but surgeons are often aware of the types of repairs performed in different areas of the world. The physical examination can provide further clues as to what was previously performed. Scars around the nose and lip can alert the examiner to the primary or secondary techniques. Animation can help the examiner understand the status of the underlying orbicularis oris muscle. Intraoral examination may reveal which operations were done on the palate and identify the presence of oronasal fistulas, the status of the levator muscles, the length of the soft palate as well as the presence of alveolar clefts. Intranasal examination will help determine if a primary rhinoplasty was performed, the status of the nasal septum and turbinates, and the patency of the nasal cavity. A proper speech assessment will determine the functionality of the palate and whether more tests need to be done.
Secondary unilateral cleft lip deformities are a common occurrence in cleft centers. The etiology of these deformities is varied and can result from any number of contributing factors, including but not limited to continued facial growth, scarring, infection, or inaccurate primary repair.
Secondary deformities frequently require surgical intervention for correction, spanning from minor revision to a complete takedown and re-repair. Many different techniques have been described, depending on the location and severity. Proper treatment begins with an accurate analysis of the deformities in relation to the involved anatomic structures.
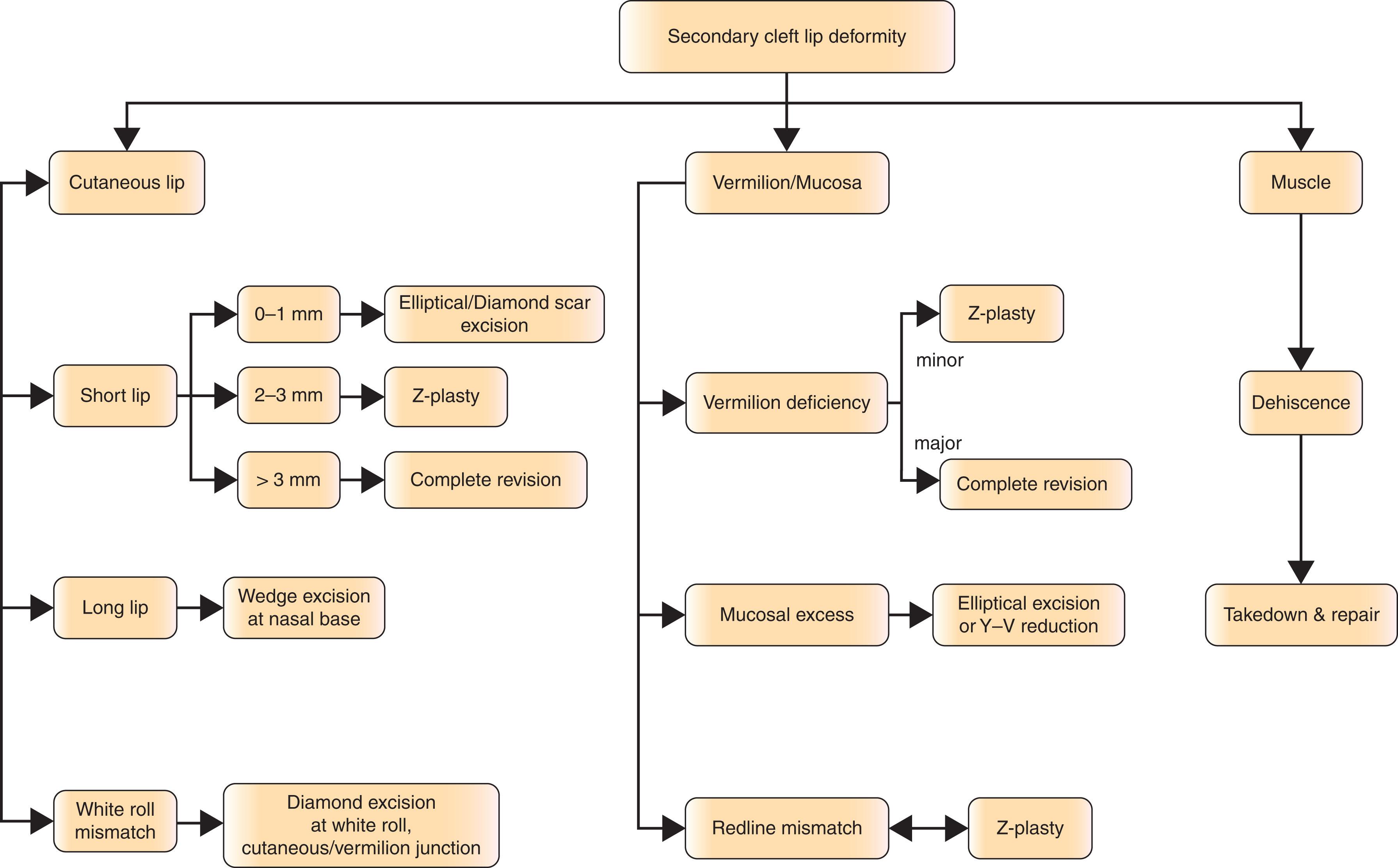
A thorough history and physical examination should be performed in a systematic fashion and documented in the medical record. 2D photographs should be performed in a standardized fashion so as to consistently and objectively capture pre- and postoperative data for evaluation and outcomes purposes. When examining the cleft lip deformity, a top down approach is advocated for simplicity’s sake. The examiner starts with the nose and ends with the mucosa of the upper lip. Care to evaluate symmetry between the affected and unaffected sides is of major importance. Review of the nose (dorsum, tip, alae, base, and sill), and lip (philtral unit, Cupid’s bow, vermilion, and mucosa) should all be done in a systematic fashion. A list of the involved anatomic structures is recorded. Treatment planning should consider the anatomy of all structures involved so that a plan to restore appropriate form and function can be made ( Algorithm 21.10.1 ).
The timing of cleft lip revision depends on the severity of deformity, the age of the patient, and the preference of the patient, family, and surgeon. Deformity severity and functional disability is relevant to surgical timing. If the lip repair is inadequate, affecting the ability to eat or drink properly, impacting speech production, or is socially unacceptable, a revision could be planned soon after evaluation. These findings would represent the more severe cases and not the norm, as most revisions can be delayed until pre-kindergarten years (4 to 5 years of age), or prior to full social integration. At this age, peer interactions begin to form and children become increasingly vulnerable to criticisms. This allows for the previous lip surgery scar to fully mature and the opportunity to combine other cleft-related operations if needed, such as speech surgery.
Proper alignment and repair of the vermilion is key to creating a symmetric and harmonious appearing lip. To accomplish this, the height of the vermilion on the cleft side should match the contralateral side. If this is not the case, and the vermilion height is less on the cleft side, a vermilion notch will result. The appearance of the lip with a vermilion notch can have the initial appearance of a short lip, but on further inspection, the vermilion discrepancy should be appreciated. The central or lateral incisor on the affected cleft side can be more noticeable than the opposite side. Furthermore, if mucosa, sometimes referred to as the wet vermilion, is displaced into the dry vermilion, an area of persistently dried, chapped lip will result. This becomes extremely bothersome to the patient and noticeable for the family.
Vermilion notching can occur despite a perfectly restored vermilion/mucosal “red line” junction. Scarring along the repair site may result in vermilion notching and may require revision. It is important to appreciate that this deformity is not necessarily a result of a loss or lack of tissue, but may be secondary to abnormal scarring or misalignment of the red line.
This deformity may be prevented by properly choosing the Cupid’s bow point on the lateral lip element (Noordhoff’s point). An incision placed too laterally compromises an already short lip in the transverse/horizontal orientation. An incision placed too medially compromises the vertical height of the lip and vermilion and also risks losing the white roll. Therefore, adhering to Noordhoff’s point during the primary repair is paramount in establishing the correct height of the lip’s vermilion.
If lip notching results from scar contracture, a Z-plasty may be used to break up the scar. The Z-plasty is also useful in realigning a malpositioned red line. Failure to initially repair the muscle or subsequent muscle dehiscence should be appreciated during the preoperative visit and addressed by dissection and re-suturing of the orbicularis oris. This can help prevent further scar contracture and notching during animation.
Augmentation with autologous fat has been used to correct notching as well as vermilion deficiency in cleft patients. This technique is indicated when the deformity results from soft-tissue discrepancy only.
The symmetry of the upper lip can be compromised by an increase in the amount of scar tissue produced, after the original repair, at the level of the mucosa ( Fig. 21.10.1 ). Scarring at the lip margin can be unpredictable and result in an asymmetric lip. Careful attention to aligning the mucosa directly below the level of the vermilion and up into the gingivobuccal sulcus is important. Furthermore, using a suture that does not cause an excess amount of inflammation can help prevent a large amount of postoperative scarring.
 with contour changes along the free vermilion border, as well as when smiling (B) .")
Mucosal thickening is a common occurrence and a hard problem to prevent. Often, mucosal excess develops during the healing process, and not being able to control how much scar tissue will form is frustrating. Excising this mucosa can be a satisfying operation, nonetheless resulting in an unsatisfying experience during the follow-up period. Secondarily, a simple transverse wedge or a Y–V advancement flap made at the level of the mucosa, inferior to the vermilion mucosal red-line margin, can be done to achieve balance. If mucosal thickening recurs after revisionary surgery, performing scar therapy and waiting a full year to 18 months for maturation is indicated. Oftentimes, with facial growth, this thickness will “even out” and further revisions may not be required.
The short lip, after a unilateral cleft lip repair, usually results from postoperative scarring, but can result from failing to balance the Cupid’s bow ( Fig. 21.10.2 ). This deformity is one of the most commonly seen and revised given its tendency to distort the normal lip architecture. All straight-line scars can shorten and, with time, a perfectly repaired cleft lip can shorten and result in an imbalanced repair and “under-rotated” Cupid’s bow. Prevention of this deformity can be achieved by “breaking up” the incision during the original repair.
 Classic secondary cleft lip and nose deformities associated with the unilateral cleft lip, including a short lip deformity, inferolaterally displaced alar base, as well as a depressed nasal tip. She also demonstrates midface retrusion.")
Minor vertical height deficiencies up to 1 mm can be corrected using an elliptical excision of the previous cleft scar at the red–white line. Due to the Rose–Thompson effect, this will elongate the lip the necessary 1 mm to match the opposite lip length and balance the Cupid’s bow. If a triangular flap repair was initially performed and the lip is moderately short (around 2–3 mm), a Z-plasty just above the white roll can be made to level Cupid’s bow and break up the scar. Alternately, an opening incision on the medial lip segment, above the white roll, can be made and a triangular flap from the lateral lip segment can fill the opening incision. Any major discrepancy in vertical height requires complete revision of the lip repair, including adequate release of all lip components from abnormal attachments, “un-bunching” of the lateral lip muscle, precise muscle alignment, and accurate leveling of the cleft-side peak of the Cupid’s bow. The use of permanent or long-lasting resorbable sutures should be considered for muscle repair to relieve tension on the closure and to prevent postoperative scar widening.
The appearance of a long lip as a secondary deformity in the unilateral cleft patient is an unusual occurrence. It is more commonly seen after a patient has been repaired with a Z-plasty type repair technique ( Fig. 21.10.3 ). This deformity occurs when the cleft-side height has been overcorrected and there has been over rotation of Cupid’s bow.

Minor vertical height excess can be reduced with a horizontal wedge excision along the nasal base. The incision is kept in this groove to prevent any noticeable scarring. Major vertical height discrepancy should be addressed with a complete revision and re-approximation of anatomic structures.
Misalignment of the white roll is another common problem seen in unilateral cleft deformities, and one of the most easily detectable from a conversational distance. A step-off at this level is readily detected by the human eye, given its position at the vermilion–cutaneous junction and its involvement in the harmony of the entire upper lip contour ( Fig. 21.10.4 ).
 . Markings were made to realign the white roll and excise the widened scar (C) , with the subsequent on-table result (D,E) .")
In cases of white roll mismatch, a diamond-shaped excision of the white roll scar, extending above and below the roll, will align the white roll. White roll mismatch may be associated with under-rotation or vertical height deficiency of the medial lip segment. Often, excising the scar in this fashion is enough to lengthen the lip and restore appropriate balance.
Poor postoperative scarring is an adverse event, which transcends the finest surgical technique and is completely unpredictable. Despite that, there are a few factors believed to be associated with poor scarring, including local wound tension, infection, and genetic predisposition. Measures are made to prevent or alleviate any factors that may contribute to a poor scar. To help relieve any unnecessary tension, complete dissection of involved structures, as well as a strong muscle repair, is performed. This should allow for the skin structures to be easily repaired without undue tension. Aggressive postoperative wound care is done to prevent infection. Scar management is employed to help achieve a thin, flat, and well-blended scar ( Fig. 21.10.5 ). This is normally done with taping, scar massaging and sun protection. Scar management lasts for 12–18 months, or until the scar has fully matured.
 . Surgical intervention required excision of the areas of hypertrophic scarring, as well as Z-plasty-based rearrangement of the red line (C,D) . The immediate postoperative outcome is demonstrated (E,F) .")
Choice in the type of suture material has been much debated and depends on the preference of the operative surgeon. Permanent sutures need to be removed in 5–7 days to prevent permanent scarring at the sutures sites. Removal usually occurs in the procedure room, requiring another anesthetic exposure. Patients, who get dissolvable sutures, do not need to have their sutures removed; however, sutures must be gone by the 5th–7th day. If they are not, notable scars along the length of the incision can result.
Scar location is another important consideration in cleft surgery. Most unilateral cleft lip operations attempt to place the repair scar along the cleft-side philtral column to match the normal side. Some repairs will incorporate a lateral rhinotomy incision to help reposition the alar base. This incision should be approached with caution due to its visibility and potential negative impact it can have on nasal alae growth.
Red or pink scars after surgery are expected and fall within the realm of normal scar maturation. Parents and families should be educated to prepare them for the amount of time it will take for this scar to fade. If, however, the scar begins to get thick, raised, and redder, a hypertrophic scar may be developing, and treatment can include taping and injections. More frequent follow-ups should be made to monitor the progress of the scar.
Unsightly scars can be addressed with scar revision by excising the scar down to underlying muscle and adequately mobilizing skin flaps for tension-free closure. The underlying muscle is assessed at the time of scar revision. If the muscle is scarred or abnormally oriented, then excision and full-thickness revision is advised. If the muscle repair is intact, then muscle imbrication, to reduce tension on the closure, can be performed. It is important to understand that scar revision also shortens an already deficient skin envelope and should be approached with caution to prevent unnecessary shortening.
It is important to assess the position of the alar base during revision. If the alar base is asymmetric, usually posterior and cephalic, the scar revision can facilitate correcting this problem. Access to the alar base and the nasalis portion of the orbicularis oris can be achieved, allowing for repositioning. During any revisionary operation, care to fully assess all other deformities should be performed with a mind towards an overall aesthetic subunit correction.
Failure to properly dissect and repair the muscle at the time of primary repair, or muscular dehiscence after surgery, can lead to lip asymmetry, unnatural animation, imbalance of the nasal bases, and vermilion notching. Muscle continuity can be assessed by evaluating for lateral muscle bulging during animation.
Failure to repair the marginal component of the orbicularis muscle, at the level of the muscle vermilion interaction, can result in notching of the vermilion. Failure to properly identify the nasalis portion of the orbicularis muscle, at the level of the nasal base, can result in an abnormally positioned alae and nasal asymmetry. Careful examination can reveal these very subtle but easy to correct problems.
Lip revision is recommended when muscle dehiscence is suspected. Revision should include complete dissection of the muscle and proper orientation of the nasalis, marginalis, and main portions of the orbicularis muscle. More so than in the primary repair, the use of permanent or long-lasting absorbable suture should be entertained to prevent muscle dehiscence and scar widening.
Treatment of patients with secondary bilateral cleft deformities requires an understanding of previous operations, as well as a thorough evaluation of anatomy. Recognition of common deformities will help facilitate the surgical planning process and assist the surgeon during future procedures. Timing of any surgical intervention is dependent upon the severity of the deformity, age of the patient, and the understanding and expectations of the family. There are characteristics specific to the bilateral cleft lip that make secondary deformities distinct from those seen in unilateral clefts, including a paucity of central lip tissue, the size of the columella, and the limited blood supply to the prolabium. It is helpful to think of bilateral cleft lip deformities in terms of issues within the layers of the lip: mucosa/vermilion, muscle, and skin. If these are taken into consideration, a successful secondary correction can be achieved.
As with unilateral clefts, the timing for bilateral lip revisions can be controversial and should be decided by communication with the patient’s family. Secondary revisions have both functional and aesthetic components. If significant issues with speech, nasal regurgitation, or socialization exist, revision should be considered sooner than later. If the revision is for aesthetic concerns, then it can be delayed until the patient and family are interested. Revisions should be delayed long enough to allow for maximal scar maturation. Revisions are often delayed until the pre-kindergarten years (age 4–5 years), unless there are functional concerns.
When revising a bilateral cleft lip, diagnosing the deformity and understanding the previous operations is of paramount importance. The nose, upper lip, and gingivobuccal sulcus should be considered in detail. Furthermore, the components of the lip, including skin, mucosa, vermilion, and orbicularis oris, should all be examined and addressed prior to devising the surgical plan. It is important to include the family in the operative plan so they are aware of what will occur.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here