Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Most histological stains are dyes which, when applied to tissues, form a chemical bond with proteins within the tissues. Staining tissue sections is essential to differentiate between the different cells and tissues on the slide, permitting examination by light microscopy. Many histological and pathological features can be identified using routine histological stains and by far the most commonly used is haematoxylin and eosin or ‘H&E’. This is regarded as the ‘bread and butter’ stain of both histology and pathology. Additional stains, as detailed below, can help to illustrate particular features within tissues such as collagen or mucin production and to identify infective organisms. If these routine stains do not provide an answer, there are further ancillary stains which can be applied such as immunohistochemistry and immunofluorescence. Further details are provided in the boxes below.
|
|
|
 |
|
 |
|
 |
|
 |
|
 |
|
 |
|
 |
|
 |
|
 |
|
 |
|
 |
|
 |
|
 |
|
 |
|
 |
|
 |
|
 |
A variety of immunohistochemical techniques are vital for diagnostic purposes in pathology as well as for research. The basis of the technique and some examples are given below. Further examples are also illustrated throughout this book to highlight specific histological features.
Immunohistochemistry (IHC; also known as immunocytochemistry) is a staining method based on the antigen–antibody reaction. IHC markers are antibodies that are produced commercially and target particular antigens (e.g. nuclear proteins, cytoplasmic proteins, cell adhesion proteins) in cells and tissues. There are hundreds of commercially available IHC markers which may highlight different components of tissues, e.g. smooth muscle markers (SMA, desmin and H-caldesmon) stain normal smooth muscle and smooth muscle tumours. IHC can provide useful information in normal histology to identify particular cells or identify the function of a cell/tissue and therefore this technique is often utilised in research laboratories. IHC is also extensively used by diagnostic pathologists for a variety of purposes such as identifying the site of origin of primary tumours, as prognostic and predictive markers in cancer and to screen for genetic diseases. Interpretation of IHC staining is complex and outwith the scope of this book, however some basic points are discussed below and throughout the organ system chapters. There is also more detailed information in Chapter 1 of Wheater’s Pathology (6th edition).
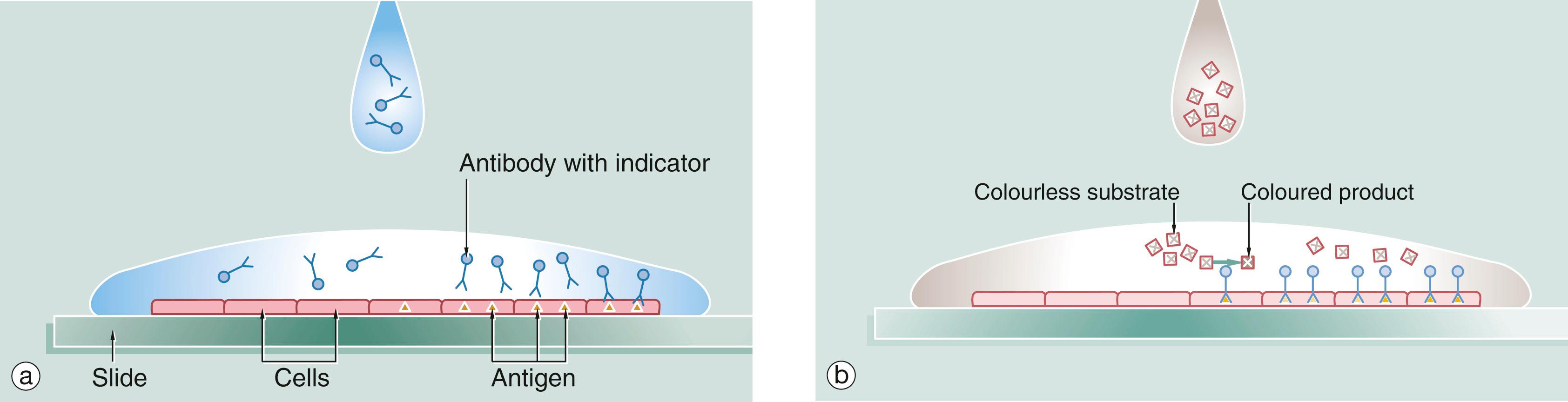
The basic technique of immunostaining is as follows: a section is placed on a glass slide (a) and a solution of antibody is laid over the issue. The antibody binds to the antigen of interest in the tissue and excess antibody is washed away so that only cells with the particular antigen have antibody bound to them. The antibody is pre-linked to an indicator substance (b). This is transformed by an enzyme from a colourless substrate to a coloured product which can be viewed by light microscopy. An enzyme commonly used for this purpose is horseradish peroxidase and the technique is known as the immunoperoxidase reaction. The substrate may also be a fluorescent substance such as fluorescein, in which the technique is known as immunofluorescence , and the position of the antibody can be viewed by a fluorescence microscope. A further modification of this principle for electron microscopy uses antibodies linked to gold which is electron dense and can be detected by EM (immunogold labelling). Further information on EM is given in Appendix 1 .
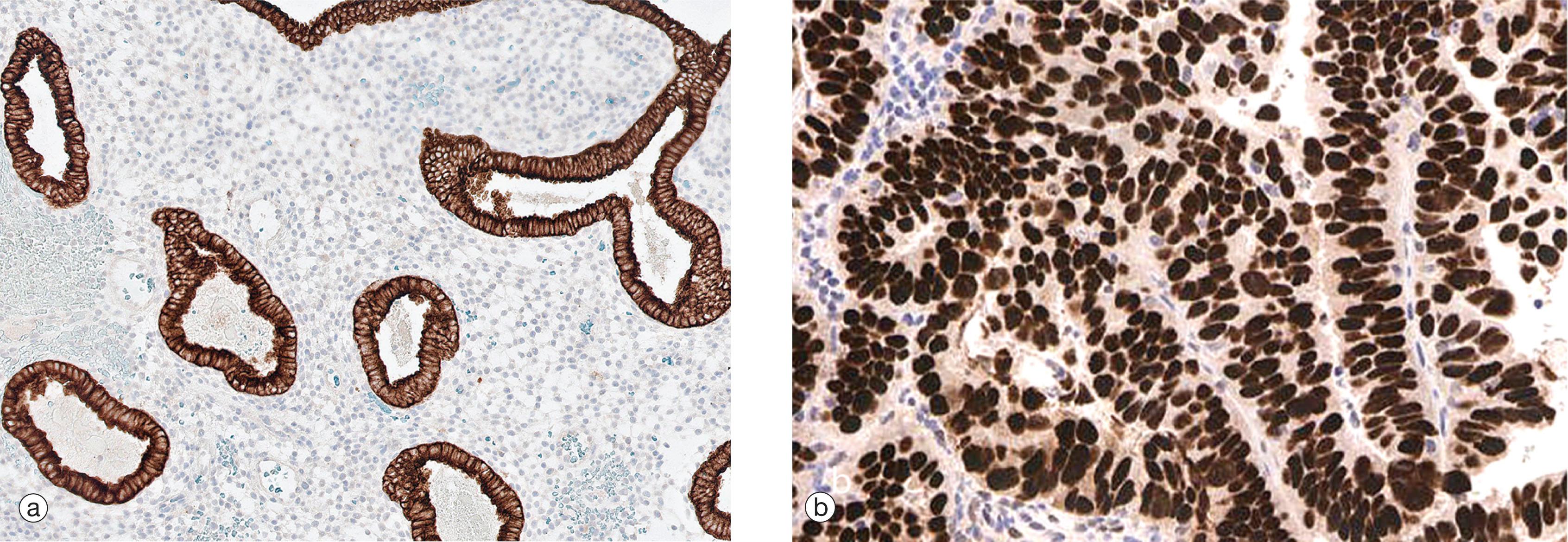
Immunostains can produce a variety of patterns of staining within the cell (nuclear, cytoplasmic, membranous or a combination). Image (a) shows endometrial tissue which has been stained with an epithelial marker (cytokeratin). The positive cytoplasmic brown staining of the glands contrasts to the lack of staining in the endometrial stroma where only the blue counterstain is seen. Image (b) shows a nuclear pattern of staining for the biomarker oestrogen receptor (ER) in a breast carcinoma.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here

