Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

; median section.")
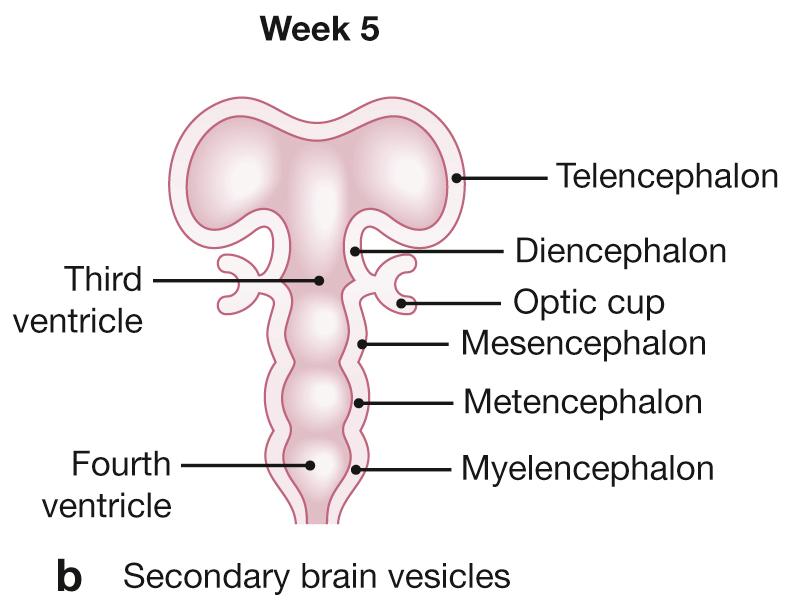
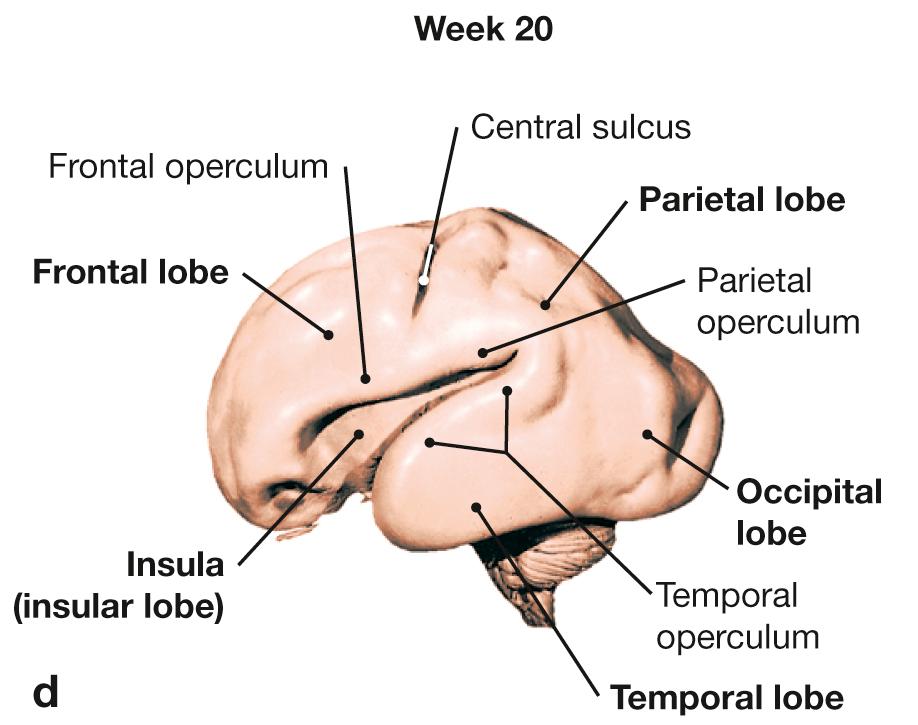
Development of the brain; a, b schematic frontal sections; c median section; d view from the left side.
Week 4: formation of three primary brain vesicles (forebrain [prosencephalon] , midbrain [mesencephalon] , and hindbrain [rhombencephalon] ).
Week 5: formation of six secondary brain vesicles (the paired vesicles of the telencephalon and the di-, mes-, met-, and myelencephalon); optic cups are formed.
Week 8: Thalamus and oculomotor nerve [CN III] are visible. The metencephalon with pons and cerebellum and the medulla oblongata [myeloencephalon] derive from the rhombencephalon .
Week 20 (fetal crown-rump length 20 cm [7.9 in]): fast growth of the telencephalon .
a, b [ E838 ]


 and the spinal cord are highlighted in color.")
, inferior view (b), view at the lateral surface of the left hemisphere (c), midsagittal view at the inner aspect of the right hemisphere (d).")

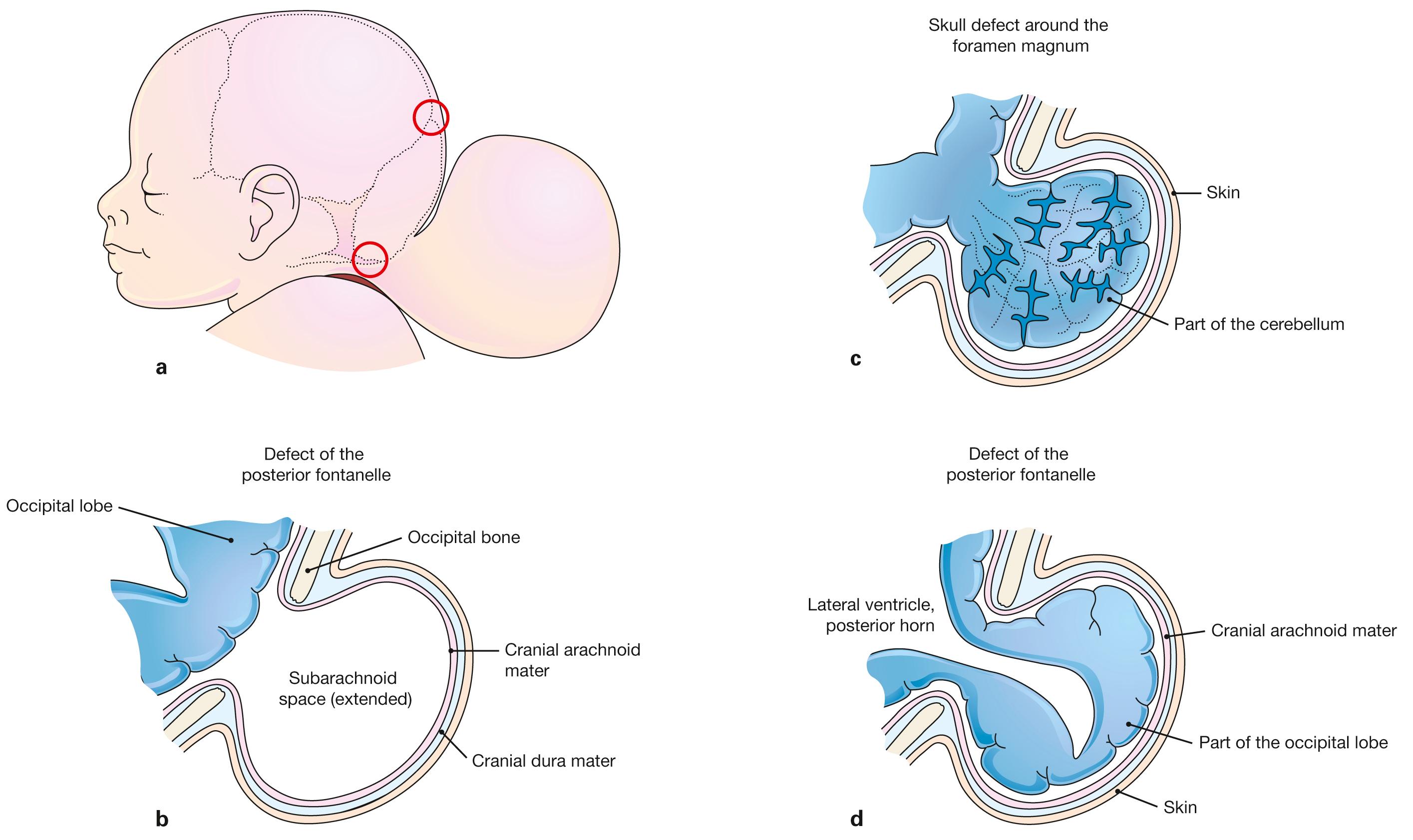
Schematic presentation of Cranium bifidum formation and various types of herniation of the brain and/or meninges.
a Head of a newborn with an extensive herniation in the occipital region. The red circles mark defects at the posterior fontanelle and foramen magnum, respectively.
b Meningocele : the hernial sac is formed by skin and meninges and is filled with cerebrospinal fluid.
c Meningoencephalocele: the hernial sac comprises prolapsed parts of the cerebellum and is covered by meninges and skin.
d Meningohydroencephalocele: the hernial sac consists of prolapsed parts of the occipital lobe and of the posterior horn of the lateral ventricle.
[ E247-09 ]


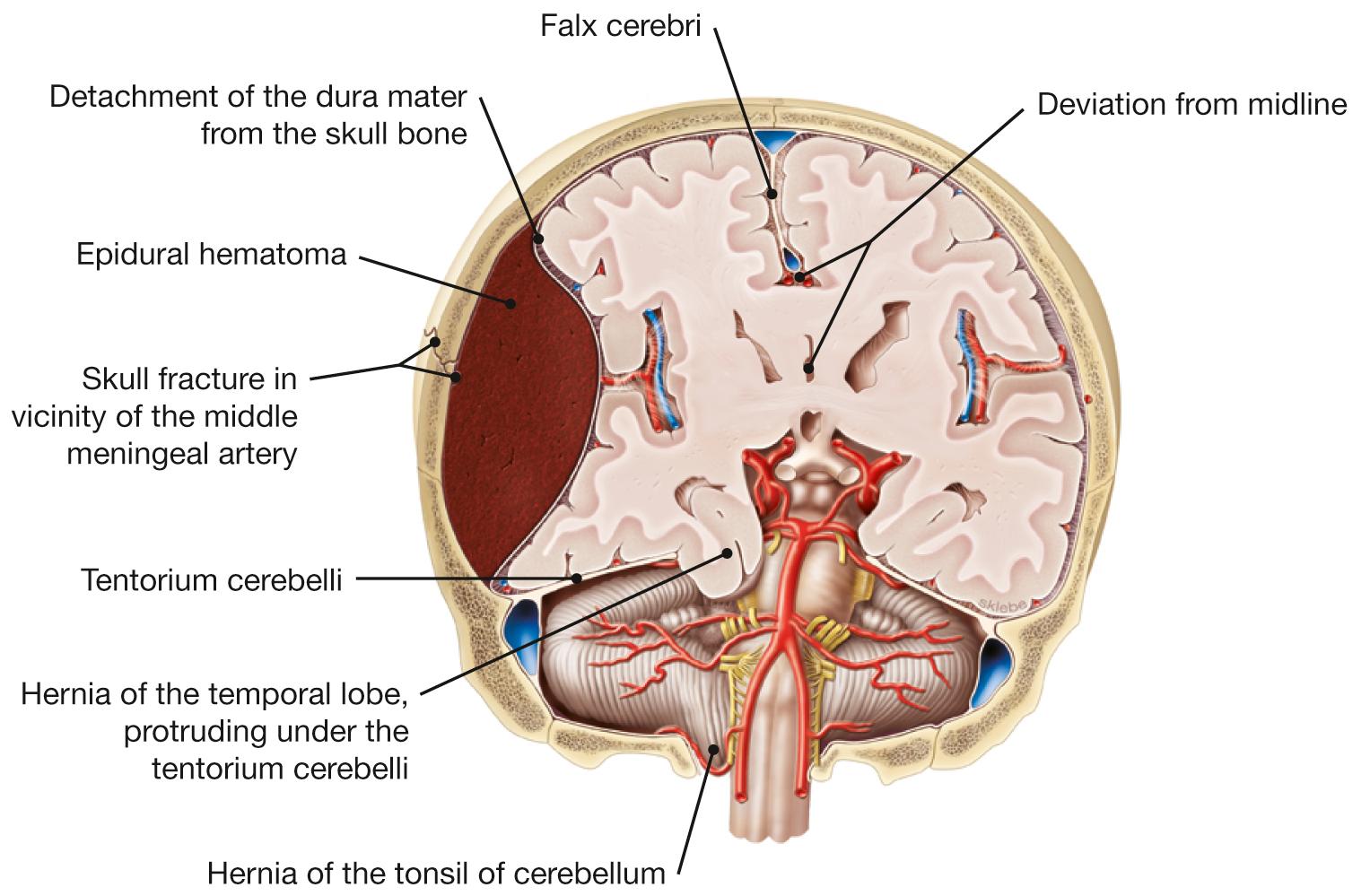
An epidural hematoma contains arterial blood due to injury to the middle meningeal artery. The ensuing pressure caused by the epidural hematoma can cause the midline to deviate sideways and results in parts of the temporal lobe being squeezed underneath the tentorium cerebelli through the tentorial notch. Compressed intracranial structures may also include CN III. As a result, on the side of the injury the eye is positioned ‘down and out’ and the pupil is fixed and dilated (see Chapter 9 (Eye) for more detail).
[ L238 ]




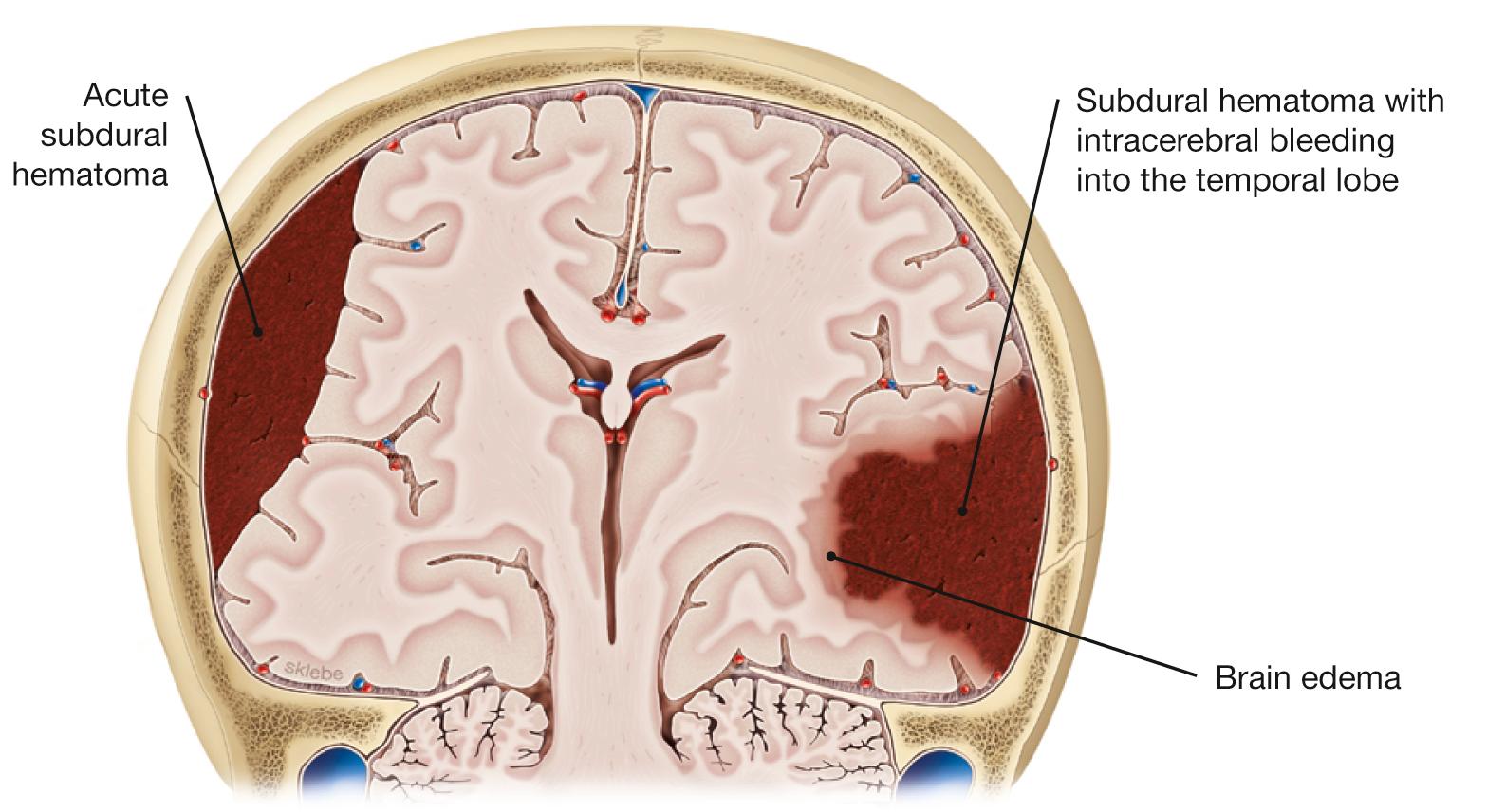
Traumatic brain injuries, e.g., car accidents, concussion, or even milder injuries to the head in elderly) can cause subdural hematomas which are caused by the rupture of bridging veins (connecting veins between cranial veins and dural venous sinuses). Acutely or in a more subtle way (sometimes over weeks!), venous blood collects between the dura mater and the arachnoid mater in the subdural space (left side). Patients show general and uncharacteristic symptoms like dizziness, headache, fatigue, listlessness, or confusion. Subdural hematoma can also coincide with intracerebral bleeding and corresponding acute neurological deficits (right side).
[ L238 ]


Injuries to the scalp can result in the spread of germs via the emissary veins and the diploic veins ( Fig. 12.9 and Fig. 12.10 ) into the dural venous sinuses and the intracranial space.


| Clinical Description of Segments of the Cerebral Arteries (used to describe the Location of Aneurysms) | ||||
|---|---|---|---|---|
| Cerebral Artery | Relation to Communicating Artery | Segment | Topographical Relationship | Tributary |
| ACA | Precommunicating | A1 | Precommunicating | Carotid |
| Postcommunicating | A2 | Infracallosal | ||
| A3 | Precallosal | |||
| A4 | Supracallosal | |||
| MCA | Precommunicating | M1 | Sphenoid/horizontal | |
| Postcommunicating | M2 | Insular | ||
| M3 | Opercular | |||
| M4 | Terminal | |||
| PCA | Precommunicating | P1 | Precommunicating | Vertebral |
| Postcommunicating | P2 | Postcommunicating | ||
| P3 | Quadrigeminal | |||
| P4 | No name | |||
 angiogram of the arterial supply to the brain.")

A cavernous sinus syndrome (CSS) can have multiple causes (cavernous sinus thrombosis, tumor, metastasis, aneurysm and fistulas of the internal carotid artery, inflammatory infiltration). CSS coincides with palsy of the abducens [CN VI], oculomotor [CN III], and ophthalmic [CN V/1] cranial nerves. A venous thrombosis and/or fistula between the ICA and the cavernous sinus (carotid-cavernous or C-C fistula) coincides with acute onset of these palsies and signs of impaired venous drainage: venous stasis in the orbit with swelling of eyelids and conjunctiva, and/or protrusion of the eyeball (proptosis, exophthalmus).
; superior view.")
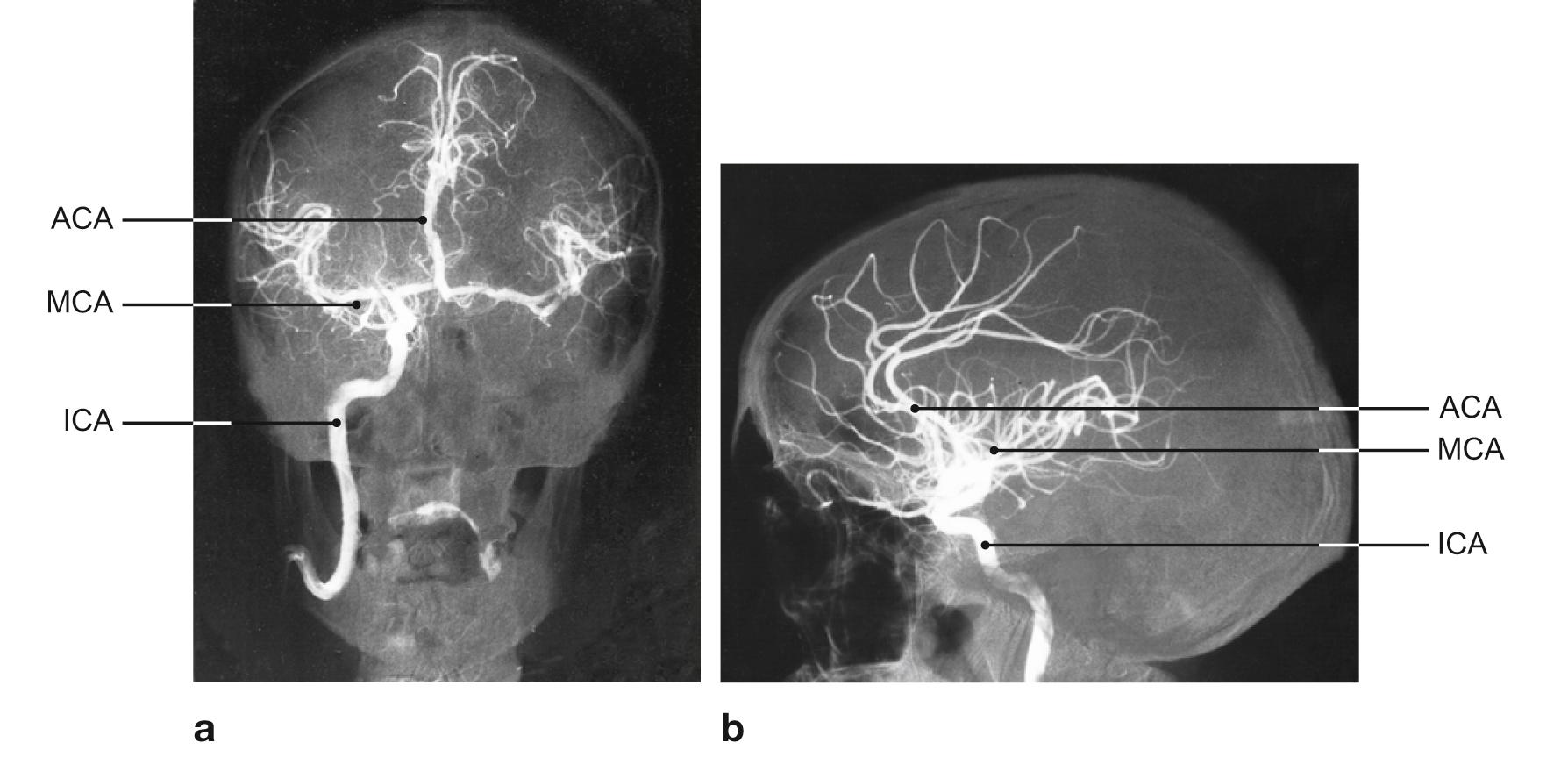
Angiogram after unilateral injection of a contrast enhancing medium into the internal carotid artery (ICA) followed by digital subtraction angiography (DSA). The ICA and its two major branches – anterior cerebral artery (ACA) and middle cerebral artery (MCA) – are shown. The contrast medium distributes to the vessels of the contralateral side via the cerebral arterial circle of WILLIS.
a A/P radiograph;
b Lateral radiograph
[ T913 ]
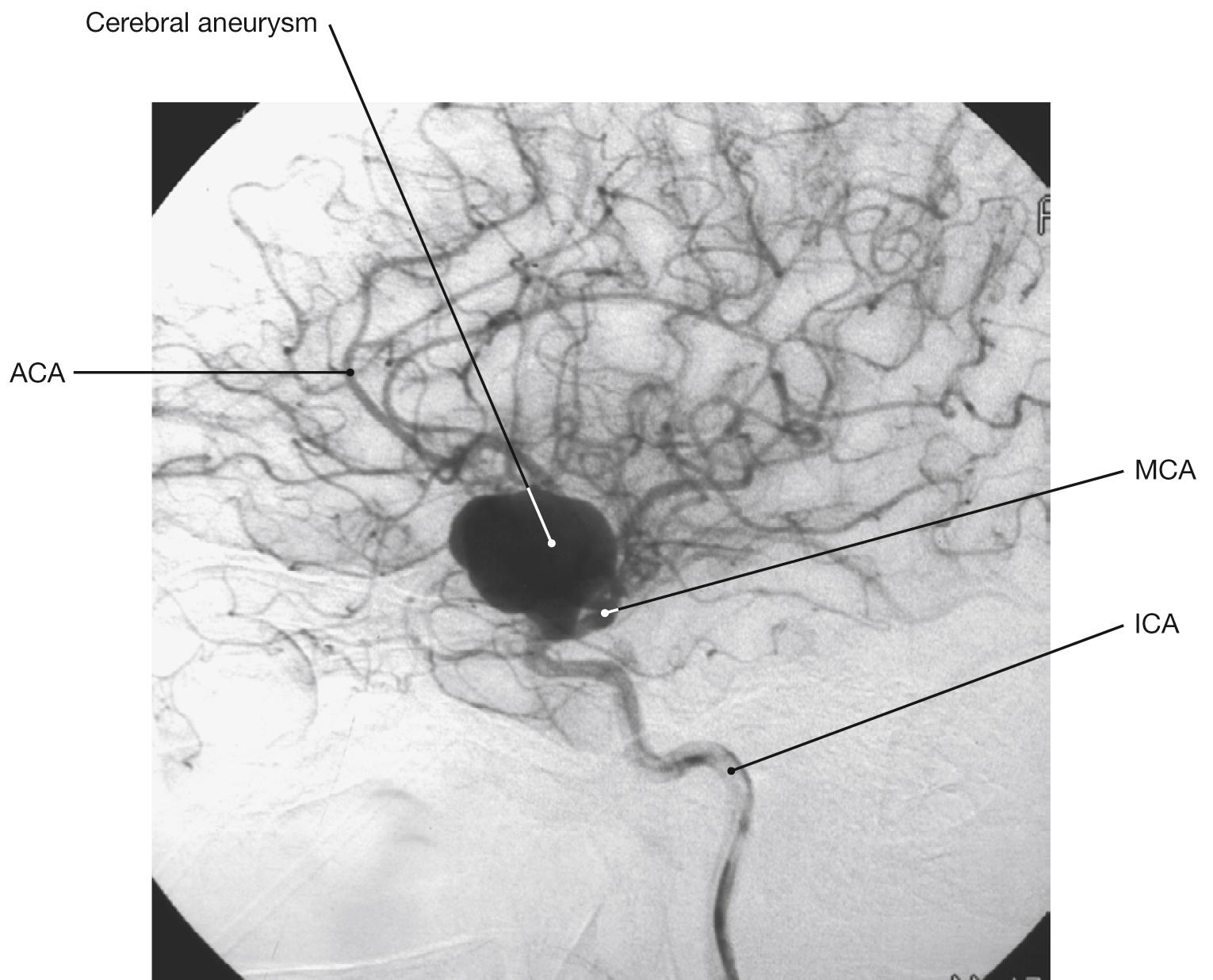
More than 90 % of all cerebral aneurysms involve the arteries of the circle of WILLIS. The anterior communicating artery (ACA), internal carotid artery (ICA), and middle cerebral artery (MCA) are frequently affected. Most cerebral aneurysms are the result of congenital defects in the vascular wall close to branching points. While most cerebral aneurysms are asymptomatic, they can compress neighboring cranial nerves and have a tendency to rupture. Cerebral aneurysms are the most frequent cause of subarachnoid bleedings . Rupture of a cerebral aneurysm causes immediate and strong headaches combined with vomiting and changes in consciousness.
[ G749 ]


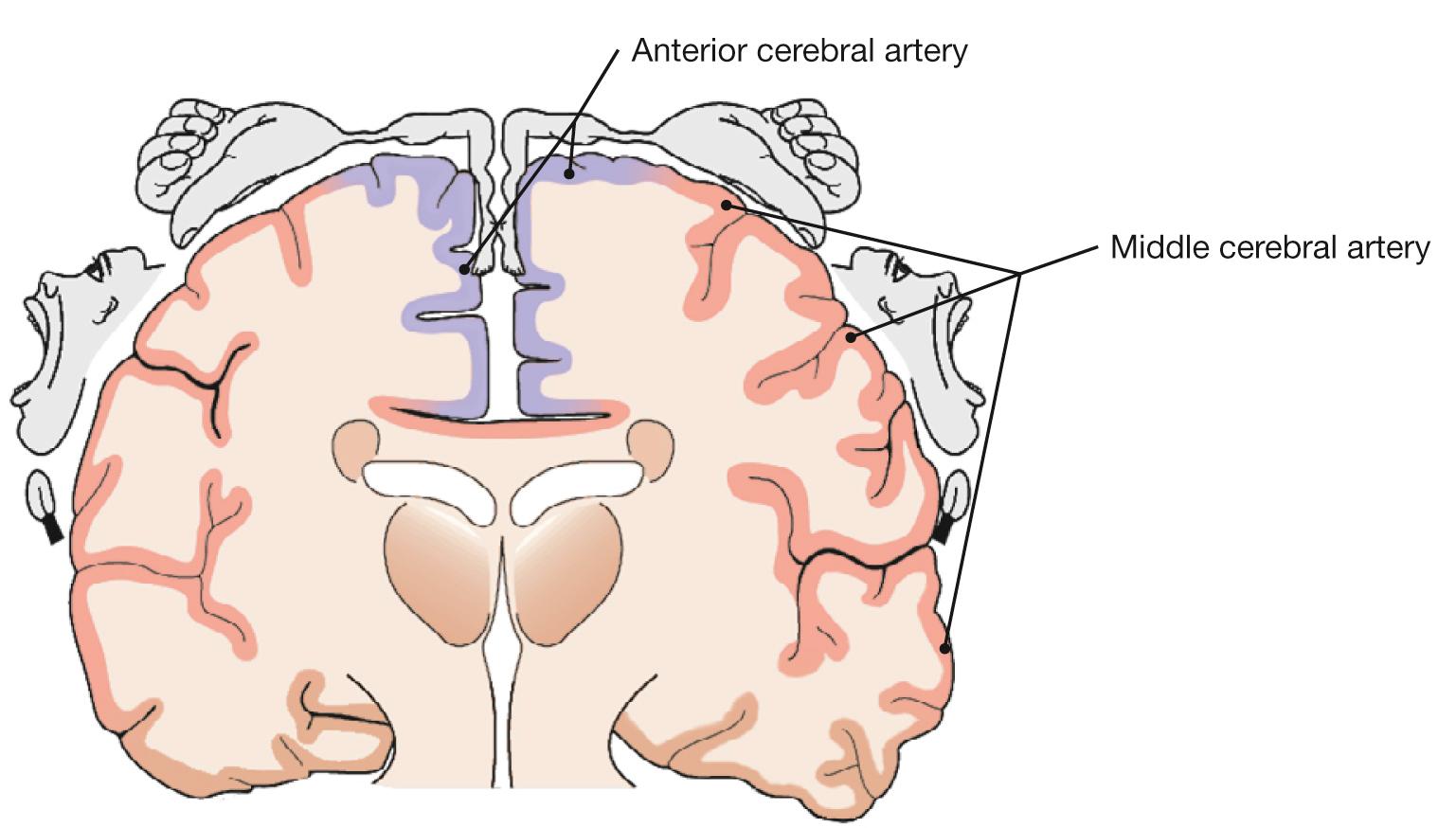
Paralysis of the lower extremity versus brachiofacial paralysis can indicate the affected cerebral blood vessel. A blockage of the anterior cerebral artery results in paralyses predominantly of the lower extremities. An impaired perfusion by the middle cerebral artery causes predominantly brachiofacial paralyses.
; lateral view (a) , frontal view (b) .")
The projections of functional regions of the cerebral surface (Homunculus) are shown in this frontal view of a coronal section of the brain. Occlusion of the middle cerebral artery shortly after branching off the internal carotid artery results in cerebral infarction (ischemic stroke) and can damage these functional regions of the brain. This explains the severe symptoms which include a contralateral, predominantly brachiofacial hemiplegia with weakness and loss of sensation (hypesthesia, local or general decrease in touch and pressure sensation of the skin). If the dominant hemisphere is affected, additional symptoms include aphasia (speech impairment), agraphia (inability to write words or text, despite existing motor and intellectual capabilities), and alexia (inability to read).
 , medial view (b) , frontal (c) and horizontal (d) sections.")


 ; schematic cross-section of a spinal cord segment (b) .")
Spina bifida is a congenital defective closure of the vertebral column and spinal cord caused by teratogenic factors (e.g. alcohol, medication) or missing induction of the chorda dorsalis.
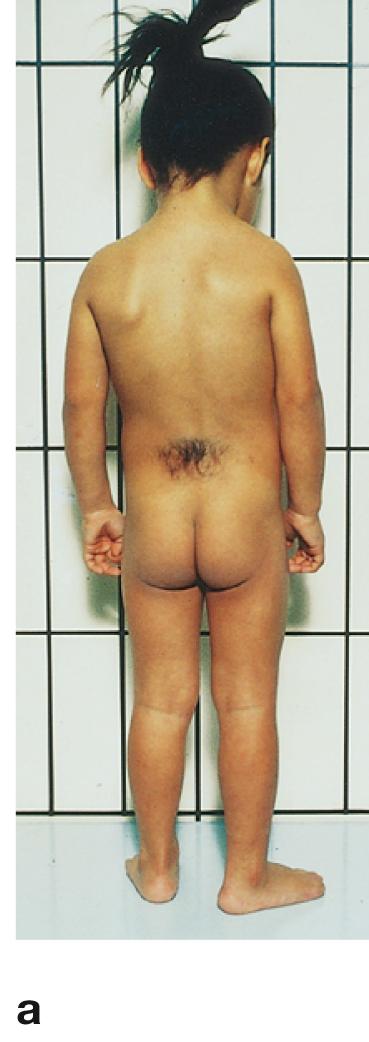
a The spina bifida occulta is the mildest form and exclusively involves the vertebral arches. In most cases, unfused arches are found in one or two vertebrae. The corresponding overlying skin is often covered with hair and is more intensely pigmented. Usually, these patients show no symptoms.
b In the case of a spina bifida cystica, the vertebral arches of a number of neighboring vertebrae are not closed; a cyst-like protrusion of the spinal meninges extends into the defect ( meningocele ). A meningomyelocele exists if the meningeal cyst contains spinal cord and nerves. This coincides with functional deficits.
Spina bifida aperta ( rachischisis, myeloschisis ) is the most severe form of spina bifida with underlying defect in the proper closure of the neural folds. With no skin cover to protect it, the undifferentiated neural plate is exposed on the back. Newborns with such defects usually die shortly after birth.
[ E247-09 ]



Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here
