Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

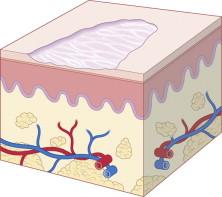
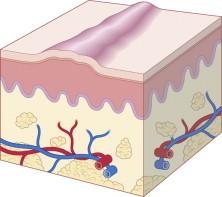
Newborn infant skin can manifest with an extraordinary array of conditions. Neonatal cutaneous findings may indicate transitory, benign processes such as erythema toxicum neonatorum, or may represent important harbingers of internal disease or genetic alteration, as might be observed in patients with herpes simplex virus infection or incontinentia pigmenti. Dermatologic manifestations are readily visible to the clinician, and it is often more efficient to first assess lesional morphology and then focus history-taking on the basis of the observed clinical findings. The timely identification and accurate diagnosis of skin findings in the newborn infant therefore relies on combining a comprehensive history with a meticulous physical examination, as well as on a proper understanding of physiologic differences between neonatal, pediatric, and adult skin that will influence both the diagnosis and the management of skin conditions appropriate to the neonate. This chapter reviews the principles of morphologic assessment in the term and preterm infant.
An understanding of the specialized reaction patterns is outlined in Tables 3.1–3.3 and Box 3.1 and, in conjunction with a comprehensive history and assessment of cutaneous morphology, will aid the clinician in making the proper dermatologic diagnosis.
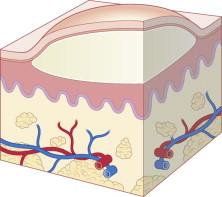
To the untrained eye, the appreciation of subtle variations in color is often the most difficult concept to grasp. Fortunately, this assessment does not carry the diagnostic weight of the primary or secondary lesions. When evaluating the color, one must take into account the background pigmentation of the patient. In infants with darker skin type, subtle erythema or jaundice may be difficult to appreciate. Likewise, pigment dilution is more difficult to evaluate in lighter skin. The most prominent colors seen in cutaneous pathologic processes are described below.
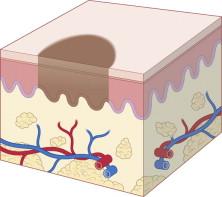
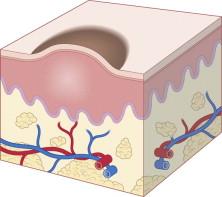
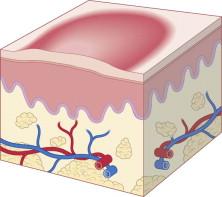
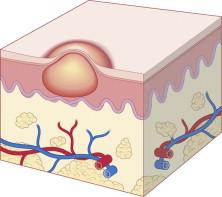
Red color can be the result of vasodilation or hyperemia caused by inflammation. Deeper red or purple hues suggest extravasation of red blood cells. Diascopy is a diagnostic maneuver to help differentiate these possibilities. By applying pressure to the lesion, one can see whether the lesion blanches, which suggests rubor due to vasodilation or inflammation. Conversely, nonblanching lesions suggest vascular damage, with consequent extravasation of blood into the dermis.
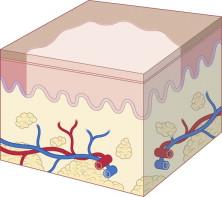
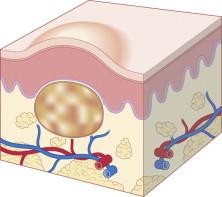
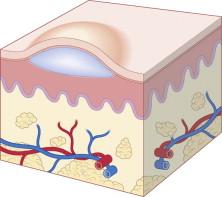
White color can be the result of loss of pigment within the epidermis or the accumulation of white material such as purulent exudate or keratinous material. One should not use the term white to describe skin-colored lesions.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here