Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Access video and video lecture content for this chapter online at Elsevier eBooks+ 

Botulinum toxin is produced by Clostridium botulinum , an anaerobic, gram-positive, spore-forming rod. The bacterium produces eight distinguishable neurotoxins. Although both types A and B are currently US Food and Drug Administration (FDA) approved, only type A toxin has indications for cosmetic use ( Table 8.3.1 ). The toxin is composed of a 100-kDa heavy chain and a 50-kDa light chain, inked by a disulfide bridge. The heavy chain binds the presynaptic neuron, allowing entry of the light chain into the cytoplasm. The light chain in turn binds and deactivates a component of the soluble N -ethylmaleimide–sensitive factor attachment protein receptor (SNARE) complex. A functioning SNARE complex is needed to release stored acetylcholine from the presynaptic neuron. Botulinum toxin types A and B have different targets within the SNARE complex. Aside from a unique mechanism of action, each commercially available type of neurotoxin has unique composition, complexing proteins, buffers, sugars, manufacturing, dosing, and clinical efficacy. Products are available in different vial sizes and can be reconstituted to various concentrations. Because of these dissimilarities, there is no standardized international dosing and dose-response equivalence between different botulinum toxin products. The area of diffusion of botulinum toxin widens with increasing volume and concentration. Studies have shown that the field effect (action halo on muscular and sweat gland activity) is comparable among the various products if using equal volumes and equipotent doses. The approximate dose conversion in Table 8.3.1 has been obtained from experimental studies and consensus guidelines. Of note, daxibotulinumtoxinA (DAXI), yet to be FDA approved, is a 150-kDa botulinum toxin type A in clinical development for aesthetic and therapeutic conditions. DAXI is formulated with a novel proprietary stabilizing peptide excipient, which is highly positively charged and binds to the negatively charged core neurotoxin. This unique peptide allows DAXI to be formulated without human serum albumin and ensures stability at room temperature before reconstitution. The safety and efficacy of a single administration of DAXI 40U for the treatment of moderate or severe glabellar lines was studied in two identically designed, pivotal, multicenter, randomized, placebo-controlled, phase 3 trials (SAKURA 1 and SAKURA 2). The primary efficacy end point was achieved in both the SAKURA 1 and 2 trials, and the median duration of none or mild glabellar line severity was 24 weeks after a single injection. Safety and efficacy results were confirmed with an open-label SAKURA 3 study. For the remainder of this article, recommended doses are based on onabotulinumtoxinA (OBA), unless otherwise specified.
| Generic name | OnabotulinumtoxinA | AbobotulinumtoxinA | IncobotulinumtoxinA | PrabotulinumtoxinA-xvfs |
|---|---|---|---|---|
| Brand name | Botox (Botox Cosmetic, Allergan, Irvine, CA) | Dysport (Galderma Pharma SA, Lausanne, Switzerland) | Xeomin (Merz Pharmaceuticals, Frankfurt, Germany) | Jeuveau (Evolus, Newport Beach, CA) |
| Mechanism | Synaptosomal-associated protein 25 (SNAP-25) | SNAP-25 | SNAP-25 | SNAP-25 |
| Aesthetic FDA indications (approval year) |
|
Glabella (2009) | Glabella (2011) | Glabella (2019) |
| Vial sizes | 50 U100 U | 300 U | 100 U | 100 U |
| Reconstitution volume (concentration) | 2.5 mL for 100 U vial (4 U/0.1 mL) | 3.0 mL (10 U/0.1 mL) | 2.5 mL for 100 U vial (4 U/0.1 mL) | 2.5 mL for 100 U vial (4 U/0.1 mL) |
| Relative strength (onabotulinumtoxinA/product) | 1:1 | 1:2–1:3 (likely closer to 1:2) | 1:1 | 1:1 |
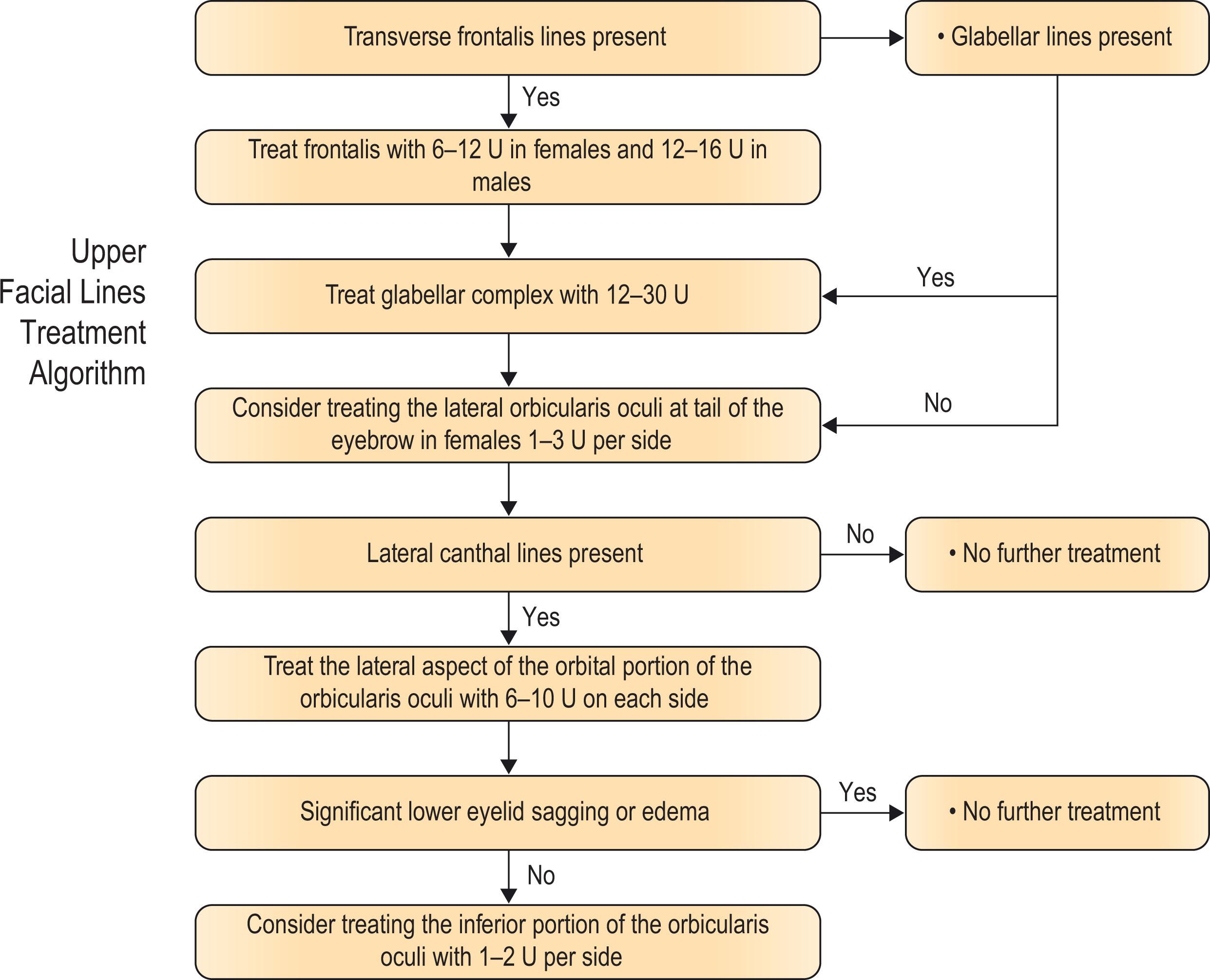
Neurotoxin can be used in the frontalis muscle to decrease the presence of transverse forehead lines produced by the muscle ( Algorithm 8.3.1 ).
The frontalis is a broad thin muscle spanning across the forehead region; it is the only brow elevator. The muscle originates from the galea aponeurotica in the scalp, and inserts into the subcutaneous tissue and deep dermis above the superciliary arch. Some fibers interdigitate with the corrugator supercilii, procerus, and orbicularis oculi muscles.
Neurotoxin can completely immobilize the forehead, thus goals must be discussed with the patient. The goal for the treatment of forehead wrinkles is to soften the undesirable lines without causing brow ptosis ( Fig. 8.3.1 ). In men, the brow should sit at the level of the supraorbital rim, whereas in women, the brow should lie well above the rim. Another description of ideal brow position noted the top of the brow to lie 2.5 cm lateral to the mid-pupillary point, with the brow-to-hairline position to equal 5 cm in women and 6 cm in men.
.")
A conservative approach is preferred, informing patients preoperatively that more than one treatment may be needed to reach the desired level of wrinkle reduction while avoiding undesirable side effects. Any discrepancy of brow asymmetry or brow position as it relates to the superior orbital rim at baseline or at maximal contraction should be noted and brought to the attention of the patients. An arched brow is more desirable in females; however, it can feminize the male face. On the other hand, a brow that sits too low can interfere with vision, cause a heavy sensation, and impart an aged and antagonistic appearance. Over-injection in the forehead should be avoided, especially in female patients who present with low and flat eyebrows or those who have significant dermatochalasis or lid ptosis, where the levator palpebrae superioris and/or frontalis muscle tone is increased to overcome inferior displacement of the upper eyelid. A recent observation by Cotofana et al. was the bidirectional movement of the skin of the forehead; the skin of the lower forehead moved cranially, whereas the skin of the upper forehead moved caudally. Both motions met at a static, nonmoving line termed the line of convergence (C-line). The C-line was identified at 61% of the total mean forehead length, identified clinically at the second horizontal forehead line when counting from superior to inferior. Injecting neurotoxin above the C-line can mitigate the risk of eyebrow ptosis.
Over-injection of neurotoxin may lead to a frozen appearance of the forehead, brow asymmetry, or medial and/or lateral eyebrow ptosis. The injection sites should be extended far enough laterally to avoid excessive elevation of the lateral part of the eyebrow, termed the “Spock” appearance. Eyebrow position results from a balance between eyebrow elevator muscles (primarily frontalis) and depressor muscles, including the procerus and corrugator muscles, which make up the glabellar complex, as well as the superolateral fibers of the orbicularis oculi muscle. To avoid eyebrow ptosis, it is important to also treat the depressors of the glabellar complex in both men and women and the tail of the brow to preserve a more arched appearance to the brow in women. For women, the consensus recommendation is of a dose ranging from 10 to 20 U for the frontalis. Gender differences in muscle mass allow a higher starting dose in men. Also, men accept and prefer a flatter, less-arched brow. For men, the consensus recommendation is 20–30 U. Injection of the frontalis is usually done in 4–6 sites, with 1–5 units per injection site, at least 2.5–3.0 cm above the orbital rim. It is recommended to inject 1–3 units into the lateral orbicularis (depressor muscle), particularly in women, to allow eyebrow elevation. This application also tends to neutralize the potential brow depression that can occur when individuals receive frontalis injections.
The musculature of the glabellar complex is the most common site for neurotoxin injection.
Two corrugator supercilii, depressor supercilii, and a procerus are the primary muscles of the glabellar complex and they contribute to glabellar lines. In addition, the medial fibers of the orbicularis oculi and the frontalis can contribute, as fibers from these muscles may interdigitate with those of the corrugators. The corrugators originate from bone in the medial brow ridge and run along the orbital rim, ending more laterally and superiorly onto the frontalis muscle. Vertical glabellar lines are formed by the action of the corrugators. Anatomic studies have shown that the depressor supercilii originates from the frontal process of the maxilla, about 1 cm above the medial canthal tendon, traveling superiorly 4–5 mm before inserting into the dermis in the medial brow. It acts as a brow depressor and may contribute to oblique glabellar lines. The procerus fibers originate from tendons in the inferior nasal bone, and interdigitate superiorly with the frontalis. Contraction of the procerus causes transverse glabellar lines.
Unlike other areas of the face, total effacement of glabellar lines is often desired in patients. Immobilizing the glabella alone can result in lifting of the lateral brow, because of unopposed action of the frontalis.
Most commonly utilized injection techniques when treating the glabellar involve a 5- to 7- point injection depending on individual variables ( Fig. 8.3.2 ). For example, men have larger muscle mass on average. Thus, men usually require more injection points than women. Another example is that in Asian patients more conservative treatment is often sufficient with possibly only three injection points needed. As the distance between both brows needs to be considered, and relaxation of the corrugators not only effaces glabellar wrinkles but will shift the most medial point of the brow superolaterally. The ideal medial brow position should begin on the same vertical plane as the lateral extent of the ala and the inner canthus. A recent study by Cotofana et al. described a 3- point injection technique with injections positioned more inferiorly than previously reported in clinical studies to match the anatomic origin of the procerus and the corrugator supercilii muscles The authors proposed that such injection technique resulted in absence of adverse events like eyebrow ptosis, upper eyelid ptosis, medial eyebrow ptosis, and lateral frontalis hyperactivity due to avoiding the eyebrow-elevating segment of the frontalis muscle.
.")
The median total dose of neurotoxin injected into the glabellar complex is 20 U, with dose ranging from 10 to 80 U. A dose-ranging study in female subjects confirmed that 10 U was less effective than 20 U, 30 U, or 40 U injected in seven points in the glabellar complex. The investigators concluded that in female patients, the glabellar complex should be treated with at least 20 U. Carruthers and colleagues injected the glabella of 80 male patients with 20, 40, 60, and 80 U of OBA (reconstituted with non-preserved saline to final dilutions of 50 U/mL, 100 U/mL, 150 U/mL, and 200 U/mL, respectively). They found doses of 40–80 U were most effective and had the greatest duration compared with 20 U, without an increase in adverse events. The peak responder rate for all treatment groups was observed between weeks 2 and 4.
When injecting the corrugators, stay at least 1 cm above the orbital rim to prevent diffusion into the levator palpebrae superioris. For the medial injection, identify the point of greatest muscle contraction. For the tail of the corrugator, Bloom and colleagues recommend identifying the most lateral aspect of the corrugator (presence of dimpling) and placing the lateral injections just medial to this insertion point in the skin. Avoid injecting the glabella alone in order to prevent exaggerated lateral brow peaking ( Fig. 8.3.3 ).

The orbicularis oculi is a sphincter-like muscle encircling the eyes. The muscle is broad and thin. Neurotoxin treatment for crow’s feet is generally directed at the lateral orbital portions of the muscle.
The orbicularis oculi is a spherical muscle consisting of a lacrimal, palpebral, and orbital portion. The orbital portion controls voluntary closure of the eyelids, creating dynamic lateral canthal lines. With time, these lines become static. In addition, the orbicularis oculi contributes to the palpebral aperture and infraorbital shelving and rhytids. There has been four identified patterns of lateral canthal lines at rest and at maximal smile: lower-fan, central-fan, full-fan, and upper-fan patterns. Full-fan and lower-fan patterns were more common in severe versus moderate lateral canthal lines at maximum smile; full-fan pattern increased with age. Lower-fan pattern was more common in males.
Lateral canthal lines present at smile but absent at rest occur naturally in mid-teenage years and reflect a positive emotional connection that is not directly tied to perception of age. The presence of lateral canthal lines at rest is tied to the perception of aging. The goal of patients is to soften the appearance of those lines at rest ( Fig. 8.3.4 ). Of note, men will tolerate more smile-associated wrinkles at rest than women and may also desire less brow elevation. Thus, the goal in men is to soften dynamic wrinkles rather than to efface the lateral canthal lines. The palpebral part of the orbicularis muscle closes the eyelid and controls the eye aperture. The muscle is targeted by neurotoxin to achieve widening of the eye aperture at rest and on smiling ( Fig. 8.3.5 ).
.")

The FDA approved the use of OBA for lateral canthal lines in 2013. A phase 2 dose-ranging study showed that there was a greater responder rate with a total dose of 24 units between both sides rather than 6 or 12 units. The consensus recommendation for lateral canthal lines is 8 to 16 U per side in women and 12 to 16 U per side in men.
The most used technique for lateral canthal lines involves three injections ( ). One injection is placed at the level of the lateral canthus, 1 cm lateral to the orbital rim. The other two are placed 1.0–1.5 cm both superiorly and inferiorly, angled at 30° anterior to the first injection. In patients with a lower-fan pattern, the other two injections can be placed anterior and inferior to the first injection, with the most antero-inferior injection made lateral to a line drawn vertically from the lateral canthus and superior to the maxillary prominence. Some investigators add microdroplets (0.5 U) of neurotoxin to the lateral inferior orbicularis oculi for lower fanning lines. It is important to inject superficially, because the zygomaticus major may be as shallow as 0.41-cm deep to the orbicularis oculi. Diffusion into the zygomaticus major or levator labii superioris can affect the smile. Men can have greater lateral fanning of the orbicularis oculi; a second row of injections is sometimes used.
Applying 1–2 U at two points per side of neurotoxin to the infraorbital eyelid – one point 2–3 mm inferior to the lower lid margin along the mid-pupillary line and the other where a line drawn from the lateral canthus inferior meets the orbital rim (inferior orbicularis oculi muscle) – can decrease lower eyelid rhytids and shelving, and increase the palpebral aperture. In a study of 15 women, this injection was shown to increase the palpebral aperture at rest by a mean of 0.5 mm, and by 1.8 mm if combined with treatment of lateral canthal lines. Before this injection, the physician should assess for lower scleral show and perform a snap test for skin elasticity. Greater degree of lower eyelid sagging increases the risk of adverse events with an inferior eyelid injection. In addition, the presence of lower eyelid and malar mound edema should be noted. Neurotoxin injection to the lower eyelid caused lower eyelid edema in 1% of patients in phase 3 trials, as the orbicularis oculi muscle participates in periocular lymphatic flow medially to laterally.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here