Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

A number of infections may be diagnosed from the characteristic appearances seen in biopsy specimens. In some cases, the diagnosis may first be suspected when a biopsy is examined by light microscopy. In other cases, the clinician suspects an infective agent and seeks confirmation by biopsy as well as by other means. Although histological appearances are often characteristic, it is usually necessary to confirm the presence of the infective agent by other techniques such as microbiological cultures or serology. In addition, the pathologist may employ a wide variety of techniques such as electron microscopy, immunohistochemical staining with specific monoclonal antibodies and a range of special stains to confirm the diagnosis.
Many infections that are otherwise difficult to diagnose arise in immunosuppressed patients, for example patients with HIV/AIDS and organ transplant recipients and, as the number of such patients increases, so the role of histopathology in diagnosis of infection expands. This chapter aims to give an overview of infections that are important in routine diagnostic pathological practice, to illustrate the appearances of these organisms in the tissues and to consider the patterns of tissue damage they cause. As prion disease specifically affects the central nervous system, this is discussed in Ch. 23 .
Most bacteria cause disease by exciting an acute exudative inflammatory response (pyogenic bacteria) . This inflammatory exudate is responsible for many of the clinical features of the disease (e.g. lobar pneumonia, see Fig. 3.3 ; bronchopneumonia, see Fig. 12.7 ). The pattern of tissue damage is similar irrespective of the pyogenic bacteria causing it and the organism can only be identified by microbiological methods. More complex mechanisms are involved in the tissue damage caused by infection with bacteria such as Helicobacter pylori , which cause inflammation by interfering with the normal physiological regulation of gastric acid secretion (see Figs 4.2 and 13.9 ). Other bacteria cause disease by producing toxins, which induce necrosis of cells and tissues (e.g. Clostridium difficile toxins destroy the surface epithelium of the colon ( E-Fig. 5.1 G ) ( Fig. 5.1 ), and some bacteria initiate a type IV hypersensitivity reaction (e.g. Mycobacteria and some Treponema organisms) and so produce characteristic changes.

A Actinomyces C colonic crypts E inflammatory exudate FB filamentous bacteria P pus

Infections caused by various Mycobacteria can frequently be diagnosed histologically because of the tissue reaction to their presence. The organisms are difficult and slow to grow in microbiological culture and therefore biopsy often plays an important role in early diagnosis. Mycobacterium tuberculosis causes tuberculosis , a disease that is increasing in incidence because of the emergence of drug-resistant strains. Mycobacterium leprae is the cause of leprosy ( Fig. 5.9 ). There are other pathogenic Mycobacteria (called atypical Mycobacteria ) that cause a range of disorders.
Important points to note about the histology of mycobacterial infections are:
Most show a granulomatous pattern of chronic inflammation (see Ch. 4 ) due to a delayed type hypersensitivity reaction.
Caseous necrosis ( Fig. 5.3 ) is particularly associated with M. tuberculosis infection.
Suppurating granulomas (with neutrophils in the central necrotic area of the granuloma) may occur in infections by atypical Mycobacteria ( Fig. 5.8 ). These organisms are also referred to as Mycobacteria other than tuberculosis (MOTT) or non-tuberculous Mycobacteria (NTM).
The causative organism can sometimes be identified in histological sections by the use of special stains (Ziehl–Neelsen, Wade–Fite) as shown in Appendix 1 .
CN caseous necrosis F fibroblasts L Langhans’ giant cell M epithelioid macrophages W fibrous wall
 Early tubercle (MP); (B) early tubercle (HP); (C) later tubercle (MP); (D) later tubercle (HP).")
.")
.")
In all cases of suspected tuberculosis, material should be submitted for culture. Culture of M. tuberculosis is difficult and time-consuming and may take 6 weeks or more. When the organisms have been cultured successfully, this allows assessment of antimicrobial resistance and sensitivity. It is often necessary to begin treatment empirically whilst awaiting microbiological confirmation and so initial histological findings supportive of this diagnosis can be very valuable. Histological identification of the organisms using special staining techniques is dependent upon the nature of the mycobacterial cell wall. This lipid-rich coating allows the organisms to retain certain dyes, even upon heating with acid and alcohol solutions, and therefore mycobacteria are often called acid and alcohol fast bacilli (see Fig. 5.10 ). Another name for M. tuberculosis which is sometimes used in clinical practice is the eponymous designation Koch’s bacillus .
B bronchiole Bo bony trabeculae C caseous necrosis D destroyed wall G granuloma L Langhans’ giant cell T tubercle
.")
C carbon pigment DN dermal nerve E epithelioid macrophages G granuloma N neutrophils
The major form of spirochaete infection worldwide is syphilis , due to Treponema pallidum . Yaws and pinta are further important treponemal infections, but these are rare except in specific tropical regions. Although now relatively uncommon, late-stage syphilis is still regarded as one of the classical examples of specific chronic inflammation. The infecting organism, the spiral-shaped spirochaete T. pallidum , resists usual tissue defences and excites a progression of fascinating pathological and clinical phenomena, which represent typical chronic inflammatory responses with superimposed hypersensitivity reactions mounted by the immune system. The condition usually proceeds through three stages over a long period.
In brief, the organism usually gains access to the body by penetrating the genital mucosa where it produces a single, small primary lesion known as a chancre . The chancre is a raised, reddened nodule caused by an intense local accumulation of plasma cells and lymphocytes in the subepithelial connective tissue. The chancre may ulcerate at this stage, but it is often painless and may easily pass unnoticed. By the time the chancre has developed, the organism has multiplied extensively and has been disseminated to regional lymph nodes and thence into the bloodstream, causing a generalised bacteraemia. The chancre and concomitant bacteraemia (primary syphilis) are followed some weeks or months later by a transient secondary stage . This is characterised by a widespread, variable skin rash, often with moist, warty, genital lesions and ulceration of the oral mucosa. These various mucosal lesions are histologically similar to the primary chancre and are full of treponemal organisms. The disease is now at its most contagious, yet the patient usually feels well and the only other evidence of a generalised infection is a widespread lymphadenopathy and positive serological findings.
In most untreated cases, the infection is effectively resolved by body defences and, in many of these patients, even serological evidence of previous infection disappears. Unfortunately, a proportion of untreated cases proceed from the secondary stage to develop tertiary syphilis , after a variable interval from one to many years. The lesions of tertiary syphilis may be either focal or diffuse and it is the focal lesion of tertiary syphilis, known as the gumma , which exhibits many of the features of a granulomatous inflammation. Tertiary lesions may occur in almost any organ or tissue and the clinical consequences vary enormously. The diffuse form of tertiary syphilis most notably involves the cardiovascular system, particularly the ascending aorta and, less commonly, the central nervous system; the well-known tabes dorsalis and general paresis of the insane (GPI) are two of the manifestations of neurosyphilis. In the focal form of tertiary syphilis, gummas may develop in the liver, bone, testes and other sites. The clinical outcome depends upon the nature and extent of local tissue destruction.
 Syphilitic gumma of the liver (LP); (B) syphilitic aortitis (MP).")
Viruses cause disease in three main ways:
By causing death of the cell they infect, either by a direct effect or by modifying the genome such that the host cell is recognised as foreign and is destroyed by the host immune system.
By causing excessive proliferation of the infected cell line, which may result in the development of malignant tumours. Human papillomavirus (HPV) is particularly important in this respect.
By integrating themselves in the cell nucleus where they produce latent infection.
Although viral culture and the demonstration of rising titres of antibodies against the virus remain the mainstays of diagnosis, some viral infections can be diagnosed by characteristic histological appearances. Individual viruses are too small to be seen by light microscopy, but when congregating together in enormous numbers within the host cell, they are visible as viral inclusion bodies and may be either intranuclear, intracytoplasmic or both. Inclusion bodies provide a histological clue to the causative virus and this can be confirmed by electron microscopy and immunohistochemistry.
One viral infection of particular importance is the human immunodeficiency virus (HIV),which is the cause of the acquired immune deficiency syndrome (AIDS). As well as producing certain characteristic histological changes, particularly affecting lymph nodes, HIV compromises the host immune system and so a range of other unusual infections may result. HIV-1 is a lymphotropic virus that gains access to cells by way of the CD4 surface protein, normally found on T helper cells as well as on most monocytes and other macrophages. Infection with HIV-1 is associated with several clinical and pathological syndromes. Some patients develop fever, weight loss, diarrhoea and generalised lymph node enlargement (lymphadenopathy) in which there is generalised follicular hyperplasia. In patients with the full-blown immunodeficiency state of AIDS, lymph nodes show loss of follicles, lymphocyte depletion, vascular proliferation and fibrosis.
E elastin I inclusion body L lymphocytes around vessels N necrosis S syncytial cells V vesicle
The two main consequences of the immunodeficiency state seen in AIDS are:
Predisposition to opportunistic infections, particularly
Predisposition to certain tumours, particularly
Kaposi’s sarcoma ( Fig. 11.11 )
Non-Hodgkin’s lymphoma, especially diffuse large B-cell lymphoma (see Ch. 16 ).
Herpes simplex virus types 1 and 2 (HSV-1 and HSV-2) cause the common skin eruptions known as cold sores and genital herpes, whilst the chicken pox virus (Herpes zoster) is responsible for shingles . In immunocompetent individuals, Herpes viruses may remain latent in nerve cells with intermittent episodes of reactivation when the virus replicates within and destroys either epidermal cells or the epithelial cells of mucous membranes. Clinically, this gives rise to the typical appearance of groups of vesicles on an erythematous background. Most lesions heal spontaneously although the latent viral DNA remains in the nerve cells and can emerge in subsequent clinical episodes. In immunosuppressed patients, such as those with AIDS or those on immunosuppressive treatment, herpetic infection may result in widespread skin or visceral infections, rather than the self-limiting rash seen in the immunocompetent.
 Skin (LP); (B) oesophagus (HP).")
.")
.")
Fungal infections range from minor localised skin infections to life-threatening systemic diseases in immunosuppressed patients. The inflammatory reaction in fungal infections may have one of three patterns. The classical appearance is of a granulomatous inflammation, which may exhibit central suppurative necrosis. A second pattern is of acute inflammation with an infiltrate consisting primarily of neutrophils. This pattern is seen in Candida infection of the oesophagus. The third is a very minimal inflammatory response, as in superficial infections of the skin by dermatophytic fungi.
Fungi are not usually obvious on routine H&E staining, but the thick cell walls are highlighted by special stains such as periodic–acid Schiff (PAS) or silver stains. Some fungi are easily recognised histologically because of the characteristic shape and structure of the hyphae and the pattern of budding of the yeast forms. Despite this, culture techniques are preferable for definitive identification of fungal species. An important diagnostic point is that the presence of fungal yeast forms, such as Candida at a mucosal surface or on the skin, does not necessarily indicate active infection, as these agents are common commensals. Evidence of active invasion must be demonstrated and, in most cases, there is an appropriate inflammatory response.
Many superficial forms of fungal infection are very indolent and slow growing and, as a result, treatment with anti-fungal drugs may need to extend over a prolonged period. It may be important to identify the precise type of fungus that is causing infection in order to ensure that the organism is sensitive to the form of treatment chosen. As fungi tend to have different growth requirements from bacteria, the microbiology laboratory must be informed if fungal infection is suspected so that appropriate cultures can be undertaken.
B binucleate cell D dyskeratotic cell G giant cell H hyphae I inclusion body K koilocyte ND necrotic debris Y yeast forms
 Oral candidiasis (PAS) (HP); (B) oesophageal candidiasis (PAS) (HP); (C) myocardial candidiasis (PAS) (HP).")
A Aspergillus hyphae E exudate F fruiting bodies H hyphae I inflammatory cells L lymphocytes N necrotic tissue S septa
Zygomycosis (also termed mucormycosis ) is a form of opportunistic fungal infection caused by one of a range of environmental fungi of the class Zygomycetes . These organisms pose no threat to immunocompetent individuals but can cause very serious and often life-threatening infections in those who are immunocompromised, particularly in patients with diabetes in whom the organisms may infect the nose and paranasal sinuses, invading from this site to involve the orbits and cerebrum (rhinocerebral mucormycosis) . In cases of mucormycosis, the hyphae are broad and irregular, branching at near right angles (in contrast to the acute angles seen in Aspergillus infection). Also, the hyphae typically appear open and non-septate in routine preparations. Often, the fungi invade into artery walls and may then give rise to thrombosis and tissue necrosis.
 MP; (B) HP; (C) HP; (D) silver stain (HP); (E) Aspergillus niger (MP).")
Of the wide range of protozoa that are of pathological importance, only a few are usually diagnosed histologically. Many of these organisms are major causes of morbidity and mortality in particular geographic regions in the developing world. Increasingly, such infections may be seen elsewhere as a result of more widespread travel and migration. Protozoa are unicellular organisms that may reproduce asexually or sexually. Many have a complex life cycle involving one or more animal hosts. Giardia lamblia is a common protozoan infecting the small intestine in communities worldwide ( Fig. 5.19 ). Trichomonas vaginalis is another protozoan parasite that is a common cause of female genital tract infection ( Fig. 5.20 ). This organism is frequently encountered in cervical cytology screening. Malaria and amoebiasis are also described in this chapter ( Figs 5.21 and 5.22 ). A wide variety of helminths infect humans, many primarily infecting the gut, although they may pass through other anatomical sites en route. Some helminths, such as the nematodes Enterobius vermicularis and Toxocara canis , are found worldwide, while others, such as Wuchereria bancrofti , have a more limited tropical distribution. Enterobiasis is fairly commonly seen in routine practice ( Fig. 5.24 ) and Schistosomiasis is of particular histological importance ( Fig. 5.23 ). These infections are illustrated.
| Disorder | Main features | Figure |
|---|---|---|
| Bacterial infections | ||
| Clostridium difficile E-Fig.5.1 G |
Pseudomembranous colitis with focal epithelial necrosis due to toxin. ‘Volcano’ pattern with inflammatory exudate | 5.1 |
| Actinomyces | Filamentous bacteria forming ‘sulphur granule’ colonies with encrusted proteinaceous material | 5.2 |
| Mycobacterium tuberculosis E-Fig. 5.3 G |
Granulomatous inflammation with caseation and Langhans’ giant cells Ghon complex. May progress to miliary disease if immunosuppressed | 5.3–5.7, 5.10A |
| Atypical mycobacteria (MOTT, NTM) | Often in immunocompromised patients. Suppurative granulomas | 5.8 |
| Mycobacterium leprae | Pattern depends upon immune status (tuberculoid/lepromatous). Granulomatous inflammation of skin and dermal nerves | 5.9, 5.10B |
| Treponema pallidum | Primary, secondary and tertiary syphilis. Chancre, gumma, endarteritis obliterans | 5.11 |
| Viral infections | ||
| Herpes simplex virus | Types 1 & 2. Oral and genital herpes. Disseminated in immunosuppressed. Vesiculation with syncytial giant cells and intranuclear inclusions | 5.12 |
| Varicella zoster virus | Cause of chickenpox and shingles. Morphology similar to HSV | Like 5.12 |
| Cytomegalovirus | Non-specific symptoms normally. Disseminated in immunosuppressed. Very large cells with intranuclear and intracytoplasmic inclusions | 5.13 |
| Human papillomavirus | Many types, causes common wart. Oncogenic forms cause cervical cancer Koilocytosis, binucleation, dyskeratosis and dysplasia (CIN) | 5.14, 17.6, 17.7 |
| Fungal infections | ||
| Candida | Common, often affects mucous membranes. Typically neutrophil response. Yeast forms and branching pseudohyphae | 5.15 |
| Aspergillus | Mostly lung disease. Allergic, colonising and invasive forms Narrowing septate hyphae with branching at acute angles | 5.16 |
| Zygomyces | Mucormycosis. Typically sinonasal disease in diabetic patients. Invades vessels. Broad and non-septate hyphae with right-angle branching |
|
| Pneumocystis | Environmental fungus, pathogenic in immunocompromised, e.g. AIDS. Foamy exudate in alveoli, cup-shaped organisms on silver stains | 5.17 |
| Cryptococcus | Mostly in immunocompromised patients. Can cause lung disease in normal people. Yeasts with thick outer capsule | 5.18 |
| Protozoa and helminths | ||
| Giardia lamblia | Cause of infective diarrhoea. Protozoan parasite infecting small intestine. Small sickle-shaped organisms on mucosal surface | 5.19 |
| Trichomonas vaginalis | Common cause of vaginal discharge and irritation, often seen in cervical smear tests. Pear-shaped protozoan parasites with flagellae | 5.20 |
| Plasmodium sp. | Cause of malaria. Intracellular parasites with complex life cycle, spread by mosquito. Pigmented organisms in erythrocytes, vascular complications | 5.21 |
| Entamoeba histolytica | Very common cause of dysentery worldwide. Invades colorectal mucosa. Flask-shaped ulcers and organisms larger than macrophages, PAS positive | 5.22 |
| Schistosoma sp. | Important worldwide. Complex lifecycle involving snail. Eggs lodge in various tissues and cause granulomatous inflammation |
5.23 |
| Enterobius vermicularis | Threadworm or pinworm. Common, colonises ileocolic area. Worms do not invade. Eggs cause perianal irritation. Often seen in appendix | 5.24 |
C Cryptococci Cap capsule E erythrocytes G Giardia O Trichomonas organism S squamous cell V villus
.")
A amoebae AP alar projection C cuticle E epithelioid cells G giant cell L longitudinal section through worm M mucosa SE schistosome eggs W transverse section adult worm
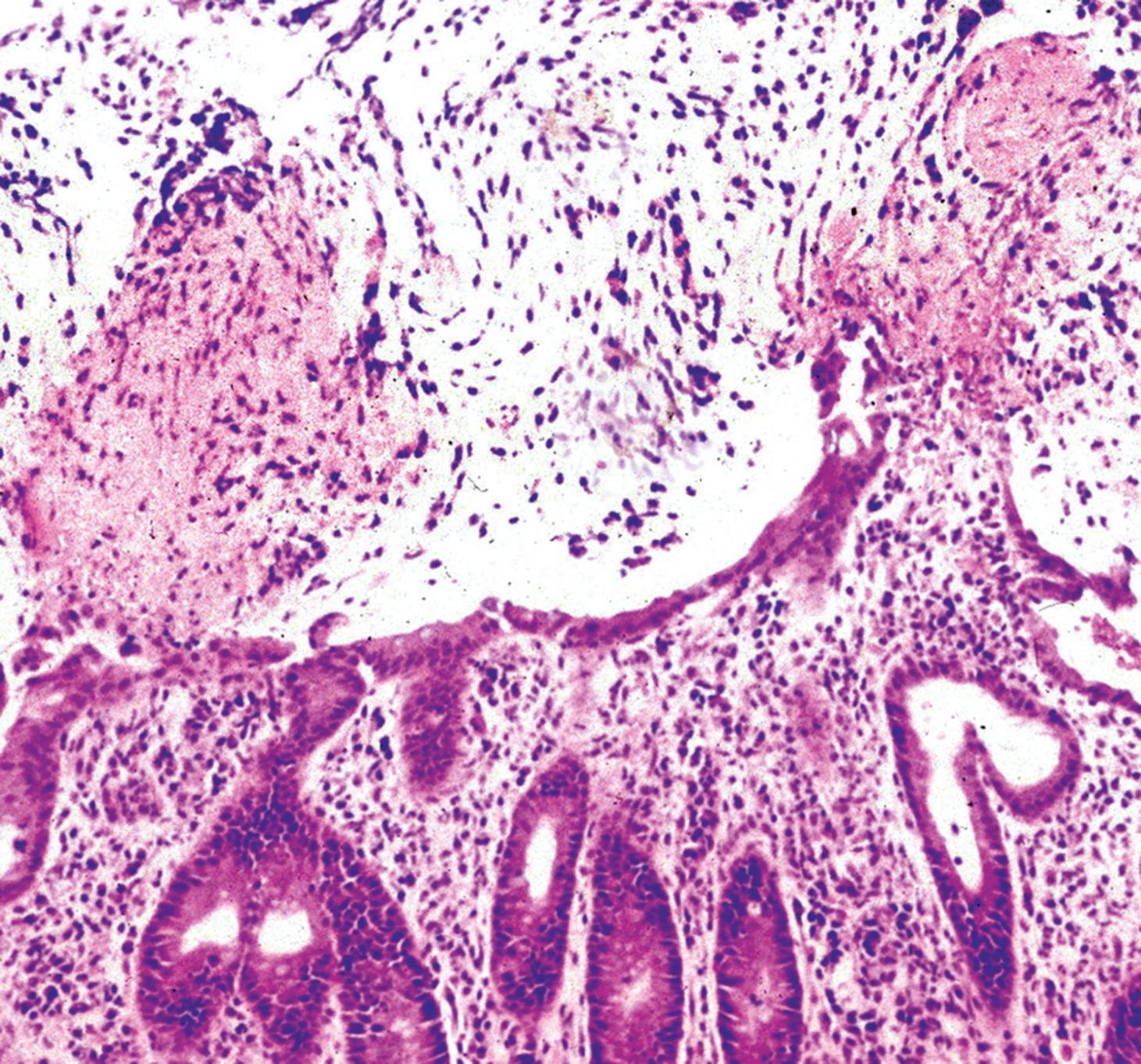
A 75-year-old man is treated by his general practitioner with antibiotics for a urinary tract infection. One week later, he develops severe blood-stained diarrhoea and is admitted via the emergency department. A colonoscopy is performed, showing severe inflammation. The biopsy appearance is shown above. Which ONE of the following statements is correct?
The organism causing his urinary tract infection is now affecting his colon.
He has amoebic colitis.
He has ulcerative colitis.
Testing for Clostridium difficile toxin should be performed.
He has diverticular colitis.
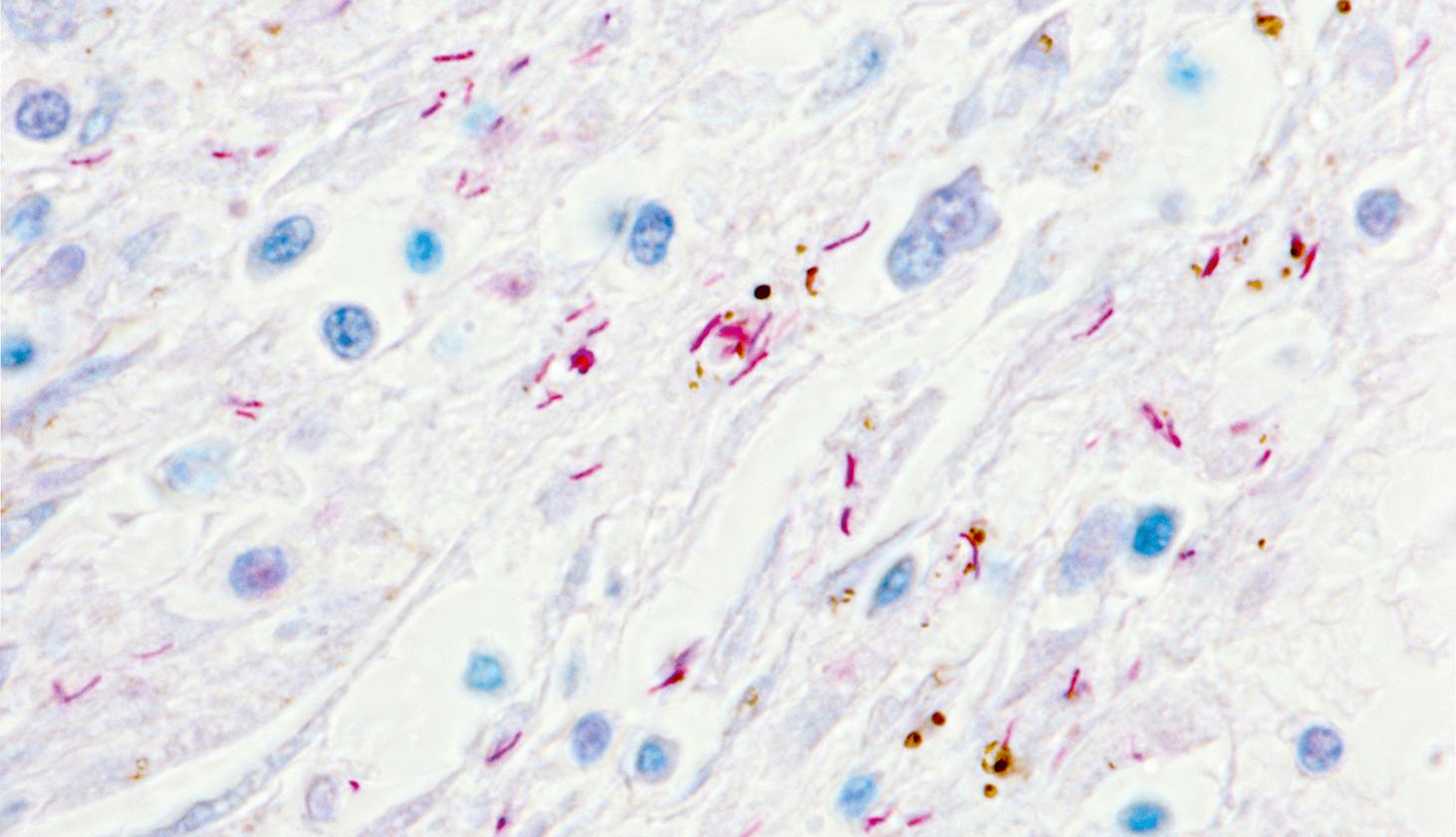
This is a lung biopsy from a 67-year-old patient with a history of chronic cough, night sweats, weight loss and haemoptysis. The biopsy has been stained by a special method to demonstrate the diagnosis. Which ONE of the following statements is correct?
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here
