Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Diagnosis of hand fractures and joint injuries requires history, examination, and adequate imaging studies.
Treatment decisions are based on fracture geometry, stability, and individual patient needs.
Nonoperative principles include reduction, maintenance of reduction through casting, splinting or buddy taping, followed by protected motion.
Operative treatment includes closed reduction with or without percutaneous pinning, external fixation, and open reduction and internal fixation (ORIF).
Rehabilitation is an important aspect of caring for patients with hand fractures and joint injuries and involves splinting and restoring motion.
Secondary procedures may be considered when the desired outcome is not achieved. These include correction of malunion, tenolysis, and capsulotomy.
Access video and video lecture content for this chapter online at Elsevier eBooks+ 

Phalangeal and metacarpal fractures are estimated to account for 16.2 and 12.5 fractures per 10,000 persons, respectively. Appropriate diagnosis and treatment can minimize deformity and improve outcomes. Although many finger and hand fractures can be managed nonoperatively, appropriate follow-up is crucial for a good outcome. These injuries can result in time away from work and activities and can be complicated by stiffness and weakness. The decision to operate depends on multiple factors, including fracture stability, location, geometry, configuration, and associated injuries. Surgery is ultimately chosen when the anticipated outcome is better than nonoperative management.
The goal of treatment of fractures in the hand is to reduce and stabilize the fracture, maintain the reduction, and begin rehabilitation to restore function (  ). The treating physician must take into account the vocation and avocation of the injured patient, as this may affect the treatment.
). The treating physician must take into account the vocation and avocation of the injured patient, as this may affect the treatment.
The metacarpals and proximal and middle phalanges are anatomically divided into the head, neck, shaft, and base. The distal phalanx is divided into the tuft, shaft, and base. The carpometacarpal (CMC) joints of the index and middle fingers have little mobility, while the ring and small fingers have some motion to allow for grasp and power grip. The metacarpophalangeal (MCP) joints are stabilized by the volar plate and the collateral ligaments: the proper collateral ligaments are thicker and run between the head of the metacarpal and the base of the proximal phalanx, while the accessory collateral ligaments are thinner and have a more vertical direction, running from the metacarpal head to the volar plate. The cam shape of the metacarpal head contributes to the tightening of the collateral ligaments when the joint is flexed, stabilizing the joint and decreasing abduction and adduction, whereas in extension, the collateral ligaments are lax and allow some radial–ulnar motion. The thick intermetacarpal ligaments stabilize the second through fifth metacarpals distally, often providing stability for fractures of the metacarpal shaft. The MCP joint articulation of the thumb is hinged, allowing flexion and extension whereas MCP joints of the index through little fingers are condyloid in nature and allow flexionextension, abductionadduction, and circumduction.
The proximal phalanx acts as an intercalated segment, with tendons running on all sides, but nothing inserting on this bone. The collateral ligaments of the proximal interphalangeal (PIP) joint contain a proper and accessory component, with insertions into the base of the middle phalanx and the volar plate, respectively. They function to provide lateral stability. The head is bicondylar in shape (as opposed to the cam shape of the metacarpal head) and the collateral ligaments of the PIP joint are tightest with the joint in extension. The middle phalanx has insertions of the extensor mechanism (central slip) and flexor tendon (flexor digitorum superficialis – FDS). The distal interphalangeal (DIP) joint is anatomically similar to the PIP joint and the distal phalanx contains the insertion of the terminal portion of the extensor mechanism and the flexor digitorum profundus (FDP).
The volar plates of the MCP joints differ from the IP joints in that the MCP joint volar plate has more of an accordion-like structure, allowing for the volar plate to be compressed with flexion and expanded with extension. The volar plates of the IP joints have stout proximal extensions known as checkrein ligaments. When contracted, these can contribute to PIP flexion contractures.
The thumb has a greater degree of motion at the CMC joint, allowing for opposition to the fingers. The CMC joint of the thumb is classified as a saddle joint allowing flexionextension, abductionadduction as well as circumduction. The shape of the thumb metacarpal head (radial condyle has greater dorsal–volar dimension) allows for pronation of the thumb to assist with opposition.
Fractures of the phalanges and metacarpals may occur through the joints (articular) or along the shaft (extra-articular). Articular fractures are more common in the PIP and DIP joints than the MCP joints and may occur through the head or the base. Fractures through the head of the phalanges are classified as unicondylar or bicondylar and can occur in the sagittal andor coronal plane. Fractures through the shaft can occur in transverse, oblique, or spiral planes. In addition, fractures can be classified as comminuted when there are multiple fragments.
The angular deformity of the fracture is dependent upon the forces acting on the distal bones. The deformity is classified according to the position of the distal fracture segment relative to the proximal segment. Metacarpal fractures most commonly have an apex dorsal angulation while fractures of the proximal phalanx tend to have apex volar angulation secondary to the pull of the interosseous muscles. Fractures of the middle phalanx have a variable deformity, depending on the location of the fracture. Those proximal to the insertion of the FDS have dorsal angulation due to flexion of the distal portion of the bone from the FDS, while fractures distal to the FDS insertion have apex volar angulation due to flexion of the proximal fragment ( Fig. 7.1 ).
 Metacarpal fractures typically have apex dorsal angulation secondary to the location of the interosseous muscles, while the proximal phalanx fractures (B) have an apex volar angulation. The angulation of middle phalanx fractures is dependent on the location of the fracture, relative to the insertion of the flexor digitorum superficialis tendon: fractures proximal to the insertion (C) will have apex dorsal angulation while those distal (D) will have apex volar angulation.")
For a dislocation to occur, the stabilizing structures (collateral ligaments, volar plate, dorsal capsule) must be disrupted. Dislocations are similarly described by the location of the distal bone and are classified as dorsal, volar, radial, or ulnar.
Fracture dislocations commonly occur at the PIP joints of the fingers, and the base of the thumb and ringsmall metacarpals. PIP joint and ulnar-sided CMC joint fracture dislocations are most commonly dorsal. Thumb CMC joint fracture dislocations are referred to as Bennett or Rolando, depending on the configuration and size of the fractured segments.
The goal of fracture treatment in the hand is to reduce the fracture and to maintain the reduction while restoring motion. Prolonged immobilization will lead to stiffness and should be avoided. Open reduction requires exposure of the fracture sites and stripping of the periosteum. This will induce scarring that impedes motion, so when open reduction is performed, it is important that fixation be stable enough to allow early motion.
For non-displaced fractures, often protection with buddy straps and active motion without resistance is adequate. For displaced or unstable fractures, reduction and fixation is necessary. Rigid internal fixation with plates andor screws can provide an anatomic reduction, and the fractures can heal by primary bone healing, but this is not always necessary for hand fractures. This can be particularly problematic for proximal and middle phalanx fractures as there are tendons on all sides that must glide for full motion. The presence of plates and screws in this area will produce scarring and often require removal to maximize motion and function.
Functionally stable fixation implies the fracture is stable enough to begin motion. This can often be accomplished by closed reduction with percutaneous Kirschner wire (K-wire) insertion. The K-wires can be removed, leaving no internal hardware and minimizing additional scarring.
Pediatric fractures, or fractures in patients with open growth plates require special attention. The physes are located in the metacarpal neck regions in the index, long, ring, and small fingers and at the metacarpal base in the thumb. The physes of the phalanges are located at the base. Growth plate fractures are described by the Salter–Harris classification ( Fig. 7.2 and Table 7.1 ), with type II being the most common. An extra-articular fracture of the proximal phalanx is the most common pediatric fracture of the proximal phalanx. This is a Salter–Harris type II fracture with angulation distal to the physis. The physeal fracture is secondary to the proximal attachment of the collateral ligament.

| Type 1 | Fracture is confined to the physis, often with normal radiographs |
| Type 2 | Fracture starts in the physis and extends through the shaft (away from the joint) |
| Type 3 | Fracture starts in the physis and extends into the joint |
| Type 4 | Fracture starts in the shaft and extends through the physis and into the joint |
| Type 5 | The physis is crushed, and there may be shearing through the physis |
General principles include early reduction and stabilization. An initial reduction attempt should be completed for displaced fractures, but repeated manipulation of a fracture involving the growth plate should be minimized as this can lead to physeal arrest and premature closure of the growth plate. Generally, the use of plates and screws is avoided, and hardware is removed when the fracture is healed. Stabilization of fractures can be accomplished with smooth K-wires and if necessary to cross the physis, effort should be made to minimize the number of passes and thus further injury to the growth plate.
Open fractures of the distal phalanx are treated with irrigation and debridement. If the circulation is intact and the patient is immunocompetent, antibiotics are not necessary. Open fractures of other bones in the hand are treated with antibiotics in addition to irrigation and debridement. Cephalosporins are generally used and with crush injuries or heavy contamination, an aminoglycoside is added. Bite wounds (human or animal) should have penicillin added to cover anaerobes ( Eikenella in human bites) and Pasteurella in animal bites (see Chapter 15 , Infections of the hand).
In high-energy injuries such as gunshot wounds, the hand surgeon may be faced with a bone defect. Historically, these defects are divided into non-critical (less than 6–8 cm) and critical (greater than 6–8 cm), but this is more applicable to long bones than those in the hand. For defects in the hand, reconstruction with autologous bone graft allows rigid fixation to promote optimal healing. Free vascularized bone flaps may be necessary when treating complex defects, such as combined soft-tissue defects, substantially scarred beds, or radiated tissue. Osteoconductive substrates such as calcium phosphate cement and demineralized bone are contraindicated in infected or potentially infected wounds; they also require a previously stabilized defect, as they will add no structural support.
The diagnosis of hand injuries begins with a history, including hand dominance and occupation as well as the mechanism of injury. The appearance of the hand should be evaluated with the fingers extended as well as flexed. The alignment of the digits may appear normal in extension, but the patient should be asked to flex the fingers as a rotational deformity may become apparent, even with limited flexion.
Specific areas of edema, ecchymosis or tenderness are noted as well as any wounds that may be present. While general screening radiographs of the hand may be beneficial for initial evaluation, specific X-rays provide better detail and should be used once the diagnosis is made (radiographs of the injured finger are preferred over radiographs of the hand for phalangeal fractures). Three views of the injured part are required to adequately evaluate a fracture in the hand.
Occasionally, additional studies will be necessary for diagnosis or to further define the injury. For example, a collateral ligament injury at the metacarpophalangeal (MCP) of the thumb may not be apparent with plain radiographs but will become apparent with stress views when the joint space is increased. Magnetic resonance imaging (MRI) can also be used to evaluate collateral ligament injuries and determine if a Stener lesion is present, guiding treatment ( Fig. 7.3 ). Computed tomography (CT) scans can be used to determine bony alignmentfracture configuration and may be helpful in some joint injuries.
 and MRI (B) demonstrating thumb MCP joint ulnar collateral ligament injury.")
Once the diagnosis of a fracture has been made, a decision must be made regarding the best treatment. Options include protection with early motion, immobilization alone or reduction by closed or open techniques. The goal should be to reduce the fracture, maintain the reduction, and return the patient to function with early motion, while minimizing stiffness.
Fractures of the distal phalanx are among the most common fractures encountered. They can involve the tuft, shaft, or base, often extending into the articular surface of the DIP joint. Tuft fractures are often associated with nail bed injuries, and repair of the nail bed often reduces and stabilizes the fracture. Shaft fractures are often stable, and patients may function well after healing with a fibrous union. For those cases where the fibrous union is symptomatic, correction of the non-unionfibrous union can be performed.
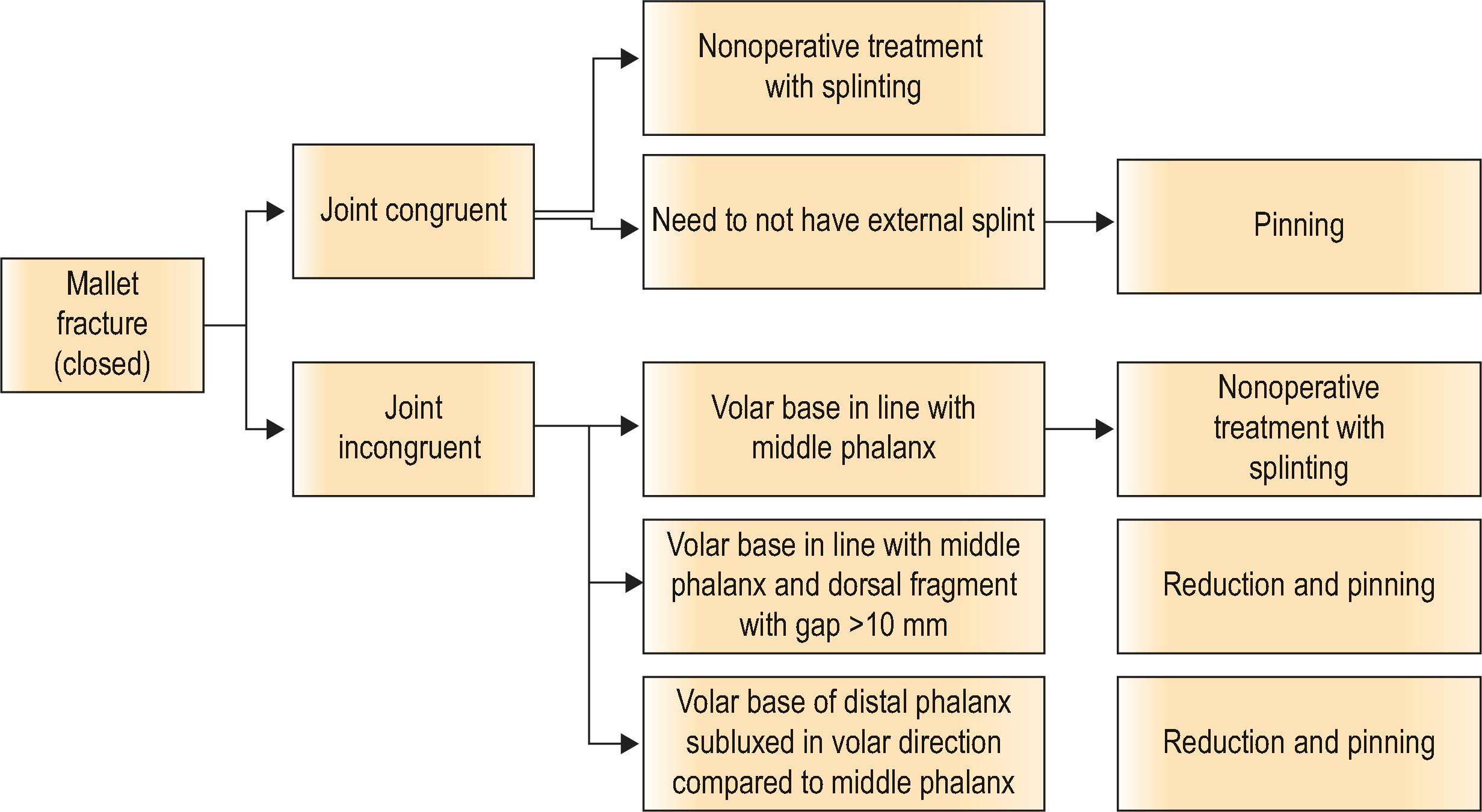
Bony mallet fractures involve the dorsal aspect of the base of the distal phalanx ( Algorithm 7.1 ). The dorsal aspect contains the terminal extensor tendon, and the goal of treatment should be to allow healing of a congruent joint without an extension lag. Most of these can be treated with a splint, maintaining the alignment of the joint. These fractures tend to have palpable and sometimes visible prominence along the dorsal aspect of the finger following healing, even when the radiographic alignment is anatomical, but this typically does not adversely affect their function. Fractures with volar subluxation of the distal phalanx should be reduced and often require pinning of the joint to maintain the reduction. Several techniques have been described, but all involve reduction of the joint surface. Attempted screw placement into the fragment is difficult, even when the fragment appears large on radiograph, and often results in fragmentation of the dorsal bone. Surgical treatment of stable fractures without subluxation is generally reserved for patients who cannot wear the splint continuously during the healing process. Complications such as pin breakage, pin tract infections, and subsequent osteomyelitis can occur, and the risks must be carefully considered.
DIP joint dislocations are typically in a dorsal direction (distal phalanx is dorsal to the middle phalanx). Acute dislocations can often be managed by closed reduction. Flexing the wrist and MCP joints to take the tension off the flexor tendons and applying distal pressure to the base of the distal phalanx will often reduce the joint. If this is unsuccessful, it is often due to tissue interposed in the joint – most commonly the volar plate – and an open reduction is necessary. This can be completed through a volar zigzag incision or midlateral incisions. The joint is exposed, any intervening tissue is removed taking care to avoid damaging the articular cartilage, and the joint is reduced. Late presentation of DIP joint dislocations will usually require open reduction, using the same technique. Following reduction, these injuries are typically stable and immediate motion can be started using a dorsal blocking splint.
Fractures involving the proximal aspect of the DIP joint can occur as isolated middle phalanx articular fractures, involving one or both condyles and may extend proximally into the shaft (diaphysis). Stable fractures can be managed with protective splinting and followed closely with radiographs. If alignment is maintained, buddy taping and range-of-motion (ROM) exercises can begin around 3 weeks and can be continued for an additional 3 weeks or until radiographic healing is present. Unstable or displaced fractures should be reduced and stabilized either with K-wires or screws.
Treatment of middle phalanx shaft fractures depends on stability and fracture pattern (transverse versus obliquespiral). Stable, non-displaced fractures can be managed with a short period of immobilization (typically 2–3 weeks) followed by protected motion with buddy taping. They should be followed closely, checking for displacement and clinical signs of malrotation, which is best evaluated with the fingers in flexion. Any malrotation is an indication for reduction and stabilization.
Oblique fractures tend to be unstable, even following closed reduction, and often result in shortening, which is poorly tolerated by the extensor mechanism. Spiral fractures shorten and rotate. Therefore, these fractures are usually best treated with stabilization. Stiffness is common following these injuries, making postoperative rehabilitation important to optimize the outcome. Plate and screw fixation can provide good stability and allow early motion, but hardware tends to irritate extensor tendons, often resulting in adhesions, necessitating removal and tenolysis to improve tendon gliding. Lag screws are better tolerated than plates, but still require soft-tissue dissection, which can result in adhesions and limit postoperative motion. K-wire fixation can often be accomplished with minimal soft-tissue stripping, providing functional stable fixation, and can easily be removed following healing. The fixation is not rigid, so the rehabilitation program cannot be as aggressive, generally focusing on active motion without resistance. These fractures take longer to heal due to the higher ratio of cortical to cancellous bone (in comparison to the proximal phalanx and metacarpal) but are usually stable enough for K-wire removal between 4 and 6 weeks. Radiographic healing may take up to 4 months. A removable orthosis for protection and protected motion with buddy strapping is instituted to maximize motion.
Injuries around the PIP joint are challenging to treat and good outcomes can be difficult to obtain. Stiffness is common and causes difficulty with gripping and grasping activities, as well as fine dexterity. The small size of the articular fracture fragments can make it difficult to maintain reduction. The goal in treating injuries of the PIP joint is to create a congruent joint and begin a rehabilitation program aimed at restoring motion.
The PIP joint functions as a hinge joint with approximately 100° of motion in the sagittal plane (flexionextension) and minimal motion in the coronal or axial planes. The base of the middle phalanx is a biconcave surface with a central ridge. The volar lateral aspects of the bone are the sites of insertion of the proper collateral ligaments. The volar plate is a fibrocartilaginous structure, which provides additional stability to the joint. It has thicker fibers that insert laterally and thinner fibers that insert centrally to the base of the middle phalanx and proximal extensions (checkrein ligaments), which attach to the periosteum on the proximal phalanx. The volar base of the middle phalanx and its curvature play an important role in stability, preventing dorsal subluxation of the middle phalanx.
The head of the proximal phalanx contains two condyles, separated by a groove or sulcus. There is a slight difference on the size of each condyle, allowing the fingers to converge in flexion. The index and middle fingers have a slightly larger radial condyle while the small finger has a slightly larger ulnar condyle.
Injuries involving the PIP joint can involve fracture of the base of the middle phalanx, the head of the proximal phalanx, a pure dislocation, or any combination of these. Fractures involving the base of the middle phalanx include dorsal base fractures (involving the insertion of the central slip of the extensor mechanism), the volar base, resulting dorsal subluxation of the middle phalanx, avulsion of the collateral ligaments, or pilon type of fracture involving the dorsal and volar margins, with a depressed central articular fragment ( Fig. 7.4 ). Fractures involving the proximal phalanx head can involve one or both condyles and can occur with or without proximal extension.
 Volar base fracture resulting in dorsal subluxation of the middle phalanx. (B) Dorsal base fracture resulting in volar subluxation of the middle phalanx. (C) Pilon type fracture with dorsal and volar base fractures and comminuted, depressed central articular surface.")
Pure dislocations result from hyperextension and an axial load. They are often dorsal dislocations and are managed similar to the DIP joint, with an initial trial of closed reduction (with the wrist and fingers flexed and distal pressure on the base of the middle phalanx). When successful, a dorsal blocking splint and early active flexion can produce good results. When reduction cannot be completed by closed means, open reduction is indicated, either through a volar or midlateral approach.
Volar dislocations are less common but can lead to late deformities if not recognized and treated. The central slip is often injured and can result in late boutonnière deformities. Following reduction, splinting the PIP joint in extension and active flexion of the DIP joint will allow gliding of the lateral bands. Active flexion can be started around 3 weeks, as further immobilization of the PIP joint may result in permanent stiffness. Irreducible dislocations are due to an interposed central slip or collateral ligament and require open reduction through a dorsal approach, allowing direct inspection of the central slip.
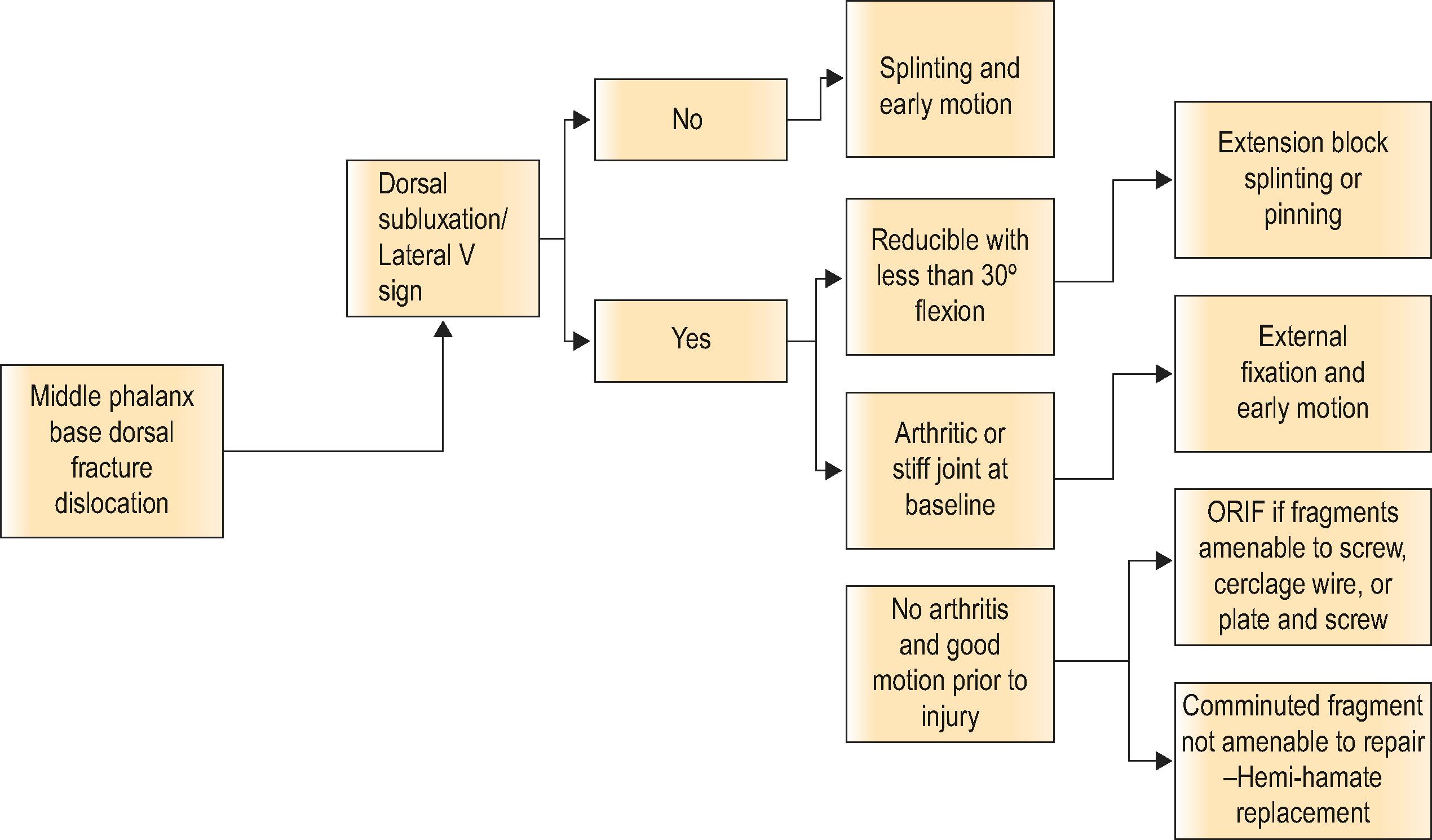
Dorsal fracture dislocations of the PIP joint result from an axial load in a dorsal direction or longitudinal direction when the finger is slightly flexed ( Algorithm 7.2 ). These are much more common than volar fracture dislocations, which result from an axial load in a volar direction or hyperextension and axial load. The dorsal fracture dislocations are classified according to the amount of the articular surface involved. Fractures involving <30% of the articular surface of the base of the middle phalanx are typically stable and can be managed nonoperatively. Fractures involving 30–50% of the articular surface are tenuous and often are unstable. Fractures involving >50% are unstable and result in dorsal subluxation of the middle phalanx ( Fig. 7.5 ).

Lateral radiographs should be carefully evaluated for the “V sign”, indicative of dorsal subluxation ( Fig. 7.6 ). The two condyles of the proximal phalanx should be superimposed, and the base of the middle phalanx should be collinear with the head of the proximal phalanx. There should be a smooth curvature of the joint surface, with a consistent space between the proximal and middle phalanx. If there is convergence of the joint space creating a dorsal “V”, the patient may be able to flex the digit at the PIP joint, but this occurs through a hinge process rather than rotation, and the joint surface will degenerate.

Treatment is directed at recreating a congruent joint surface and restoring motion. Stable fractures and those which are classified as tenuous but maintain stable reduction and a congruent joint with no more than 30° of flexion can be managed nonoperatively with a dorsal extension block splint. Active flexion is initiated and extension is allowed short of the point of subluxation. These patients should be followed closely to ensure that subluxation of the joint does not develop. Unstable fractures, or those in which a congruent joint cannot be established with <30° of flexion, require operative treatment.
A variety of techniques have been described, including extension block pinning, open reduction and internal fixation, volar plate arthroplasty, replacement arthroplasty, and external fixation. All of these techniques have case reports or small series illustrating good outcomes, but there are no prospective studies indicating one technique is better than others for a particular injury.
Fluoroscopy can be helpful to determine stability of PIP dorsal fracture dislocations.
Using live fluoroscopy and the lateral view of the finger, have the patient actively flex and then bring the digit into extension. There should be a congruent motion and then a “jump” when the dorsal subluxation occurs. This point should be noted and used to determne whether nonoperative treatment is likely to be successful.
If this is <30°, an extension blocking splint with active flexion can be used.
If this is >30°, operative treatment is indicated.
A variety of devices have been described for management of PIP joint fracture dislocations. The common principle is to produce distraction across the joint, allowing alignment to be maintained through ligamentotaxis. In addition, some devices provide a volar directed force on the middle phalanx to assist in maintaining alignment. They all allow immediate PIP joint motion. Careful attention should be paid to the fragments along the volar base of the middle phalanx as dorsal subluxation can recur if these do not heal in proper position (the volar lip of the base of the middle phalanx is a restraint to dorsal subluxation, so healing of the fracture fragments must recreate the normal curvature). In general, impaction or pilon type fractures can be managed with external fixators that provide distraction of the joint and only require two K-wires. Fracture dislocations often benefit from a third k wire to provide a volar directed force on the middle phalanx (dorsal fracture dislocation).
External fixation systems can be fabricated from K-wires with or without the use of rubber bands, or commercially available devices can be used. Fig. 7.7 illustrates an example of a PIP joint fracture dislocation in the small finger managed with an external fixator fabricated from K-wires.
 Fabrication of external fixator from K-wires. (B) Preoperative radiograph of PIP fracture dislocation involving the small finger. (C) Radiograph with external fixator in place, allowing motion. (D) Postoperative results in flexion.")
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here