Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Dementia is a group of symptoms affecting memory, thought processes, and social interactions to a sufficient extent to interfere with daily life. It is accompanied by cognitive changes such as memory loss, confusion, getting lost, inattention, diminished problem-solving ability, impaired reasoning, loss of organizational skills, and loss of coordination. Psychological changes also are seen, such as depression, anxiety, agitation, anger, inappropriate behaviors, and personality changes. The onset of dementia is usually subacute or chronic. Altered consciousness does not occur until late in the disease. Psychotic behavior is uncommon in dementia.
Alzheimer’s disease (AD) is the most common form of dementia. The cortex commonly demonstrates atrophy, with sparing of sensory, motor, and occipital cortices. The cortex and other areas such as the hippocampus demonstrate aberrant amyloid-beta deposits, extracellular neuritic plaques, and intracellular neurofibrillary tangles. See Plates 17.2 and 17.3 for details of AD and its pathology.
Frontotemporal dementia is characterized by frontal and temporal lobe atrophy, with loss of neurons and neuronal connections. Patients demonstrate altered cognition, altered decision making and judgment, disinhibition and impulsivity, altered language capabilities, and personality and behavioral changes.
Dementia with Lewy bodies , constituting 10% to 15% of dementias, is accompanied by abnormal changes in the synaptic protein alpha-synuclein (Lewy bodies) in the brainstem (especially substantia nigra, pars compacta) and many areas of cerebral cortex. Lewy bodies are sometimes found with plaques and neurofibrillary tangles in AD. Patients often experience visual hallucinations and striking images of animate objects and may exhibit cognitive impairment. Symptoms of Parkinson’s disease (rigidity, resting tremor, bradykinesia, postural instability) may occur, along with depression, anxiety, and autonomic dysfunction (orthostatic hypotension, dizziness, syncope).
Vascular dementia is the second most common form of dementia and may accompany small and/or large vessel disease. A single stroke may precipitate dementia. Gradual occurrence of small vessel disease may precipitate damage to subcortical white matter from multiple lacunar infarcts and bring about progressive cognitive impairment, including loss of attention and ability to focus, slowed thinking, impaired organizational ability, and diminished problem-solving ability. Vascular dementia is sometimes referred to as multi-infarct dementia (caused by multiple strokes) or Binswanger’s disease (subcortical arteriosclerotic encephalopathy [SAE]), small vessel disease caused by damage to white matter, such as seen in longstanding hypertension.
Treatable dementias , appearing with cognitive decline and intellectual impairment, may occur from other causes such as traumatic brain injury (TBI), brain tumors, subdural hematomas, normal-pressure hydrocephalus, metabolic encephalopathy, or depression. Such dementias may be accompanied by headache, seizures, gait disturbances, past history of TBI, changes in consciousness or presence of sleepiness, and incontinence.
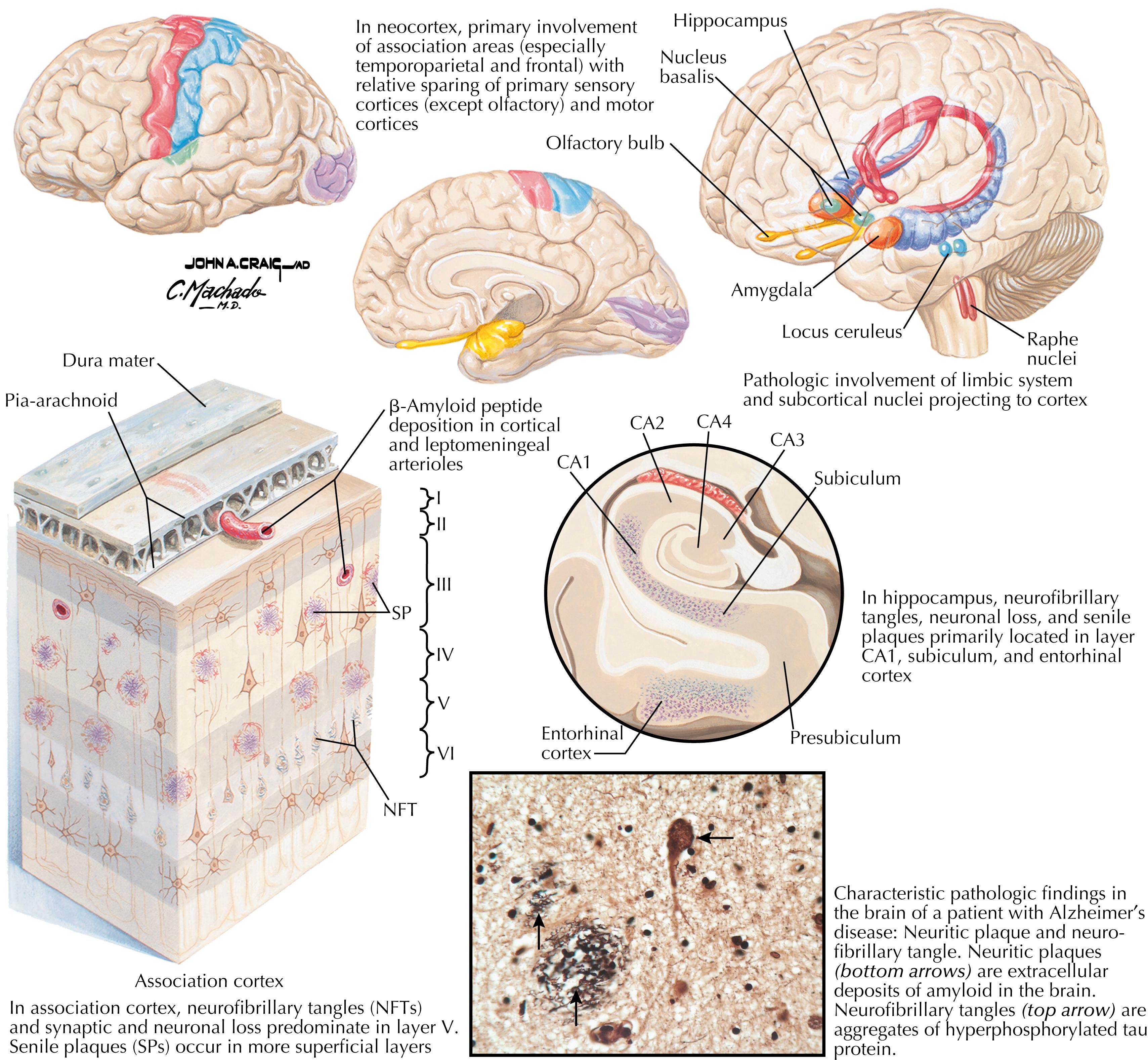
The characteristic pathology in the brain in AD is neuritic (amyloid) plaques (extracellular deposits) and neurofibrillary tangles (intracellular aggregates of hyperphosphorylated tau protein in neurons). Although these are described as the characteristic pathologic features of AD, some severely cognitively impaired individuals have normal amounts of plaques and tangles, and some individuals with extensive autopsy-confirmed plaques and tangles were cognitively intact before death.
Neuritic plaques are usually abundant in AD, particularly in frontal and parietal cortical regions, found particularly in upper layers of the cortex. Neurofibrillary tangles are abundant in neurons in AD, starting in the medial temporal lobe (amygdaloid region, entorhinal cortex), expanding into the hippocampal formation and cingulate cortex, and in late stages affecting widespread areas. Neurons with intracellular tangles are abundant in layer V of affected regions of cortex.
Clinical findings accompanying these pathologies include cognitive impairment, memory deficits, poor judgment and decision making, disorientation, and language impairment.
In early stages of AD, the CA1 sector of the hippocampus, the subiculum, and the entorhinal cortex are susceptible to neuronal damage from both plaques and tangles; hence the early presence of memory deficits, especially short-term memory deficits.
Some cortical areas remain relatively spared from pathology from plaques and tangles in AD, including sensory cortices (somatosensory, auditory, visual) and motor cortex. See Plate 16.31 Clinical Point.
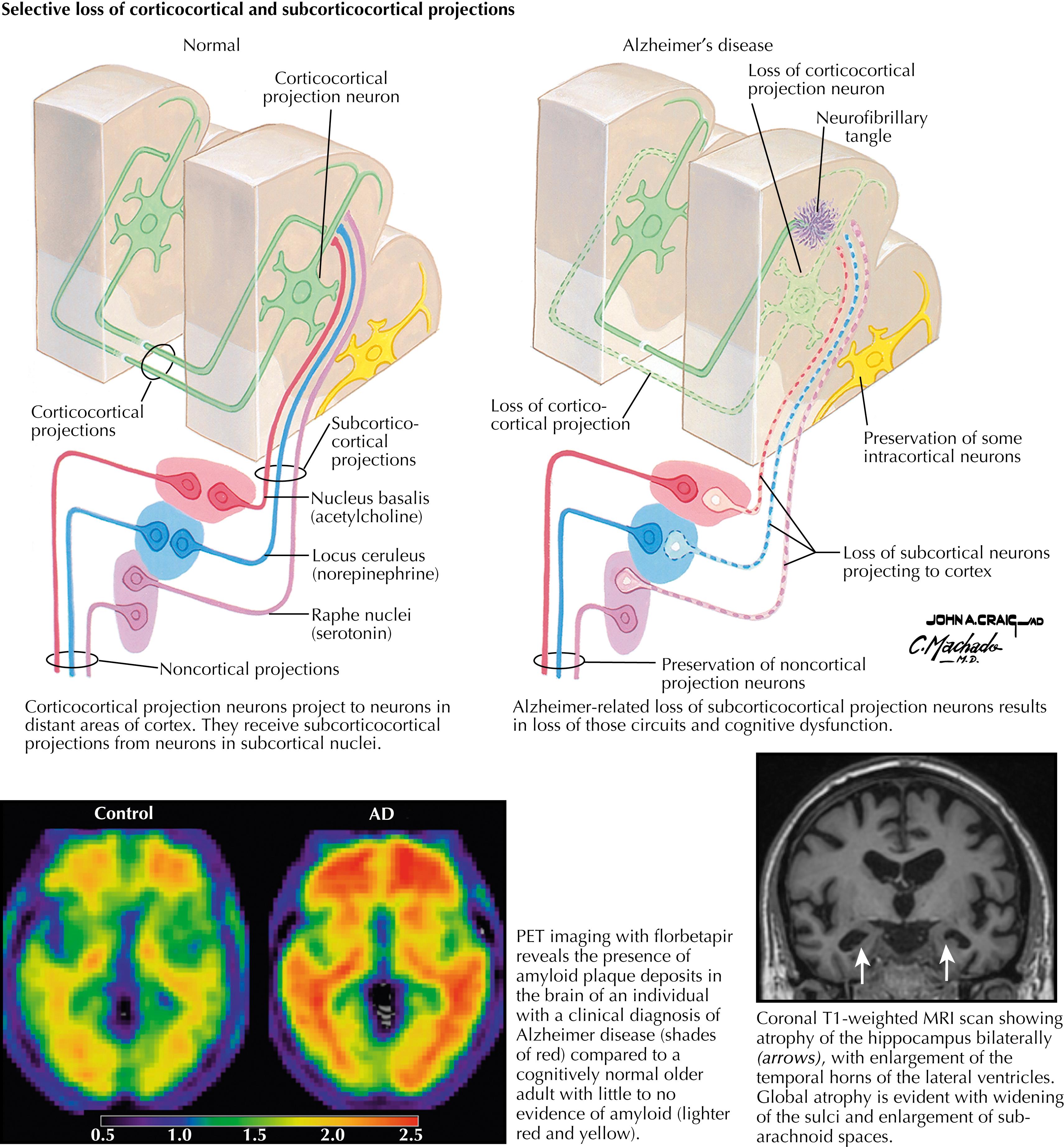
Pathological changes seen in AD include enlarged ventricles and the lateral fissure, with significant cortical atrophy and hippocampal atrophy, loss of cortico-cortical connections, and widened cortical sulci. Cellular pathology includes amyloid-beta deposits, extracellular neuritic plaques, and intracellular neurofibrillary tangles. Also present is a significant subcortical loss of serotonergic (raphe nuclei), noradrenergic (locus coeruleus), and cholinergic (nucleus basalis) nuclei and their projections to the cortex.
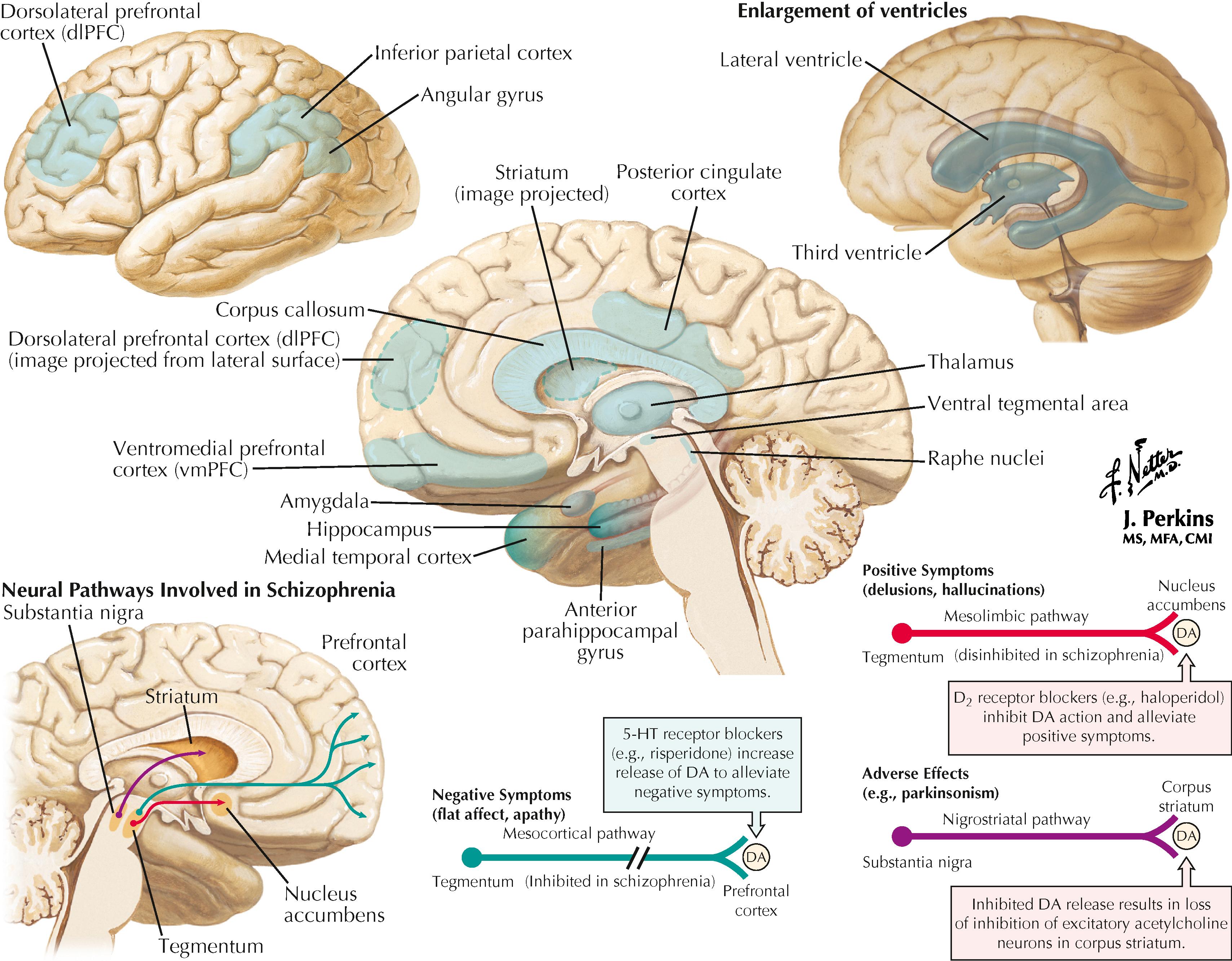
Schizophrenia is a major psychiatric disorder, with a genetic component, characterized by delusions, hallucinations, disorganized speech and thoughts, psychomotor disturbances, and often cognitive impairment. Positive symptoms (delusions and hallucinations) and negative symptoms (catatonic behavior, social withdrawal, blunted affect, alogia, and avolition) are seen. Patients sometimes have difficulty distinguishing fantasy from reality and show reduced insight and awareness of their illness. Cognitive impairment may include deficits in episodic memory, attention, executive functions, and intellectual ability. These many symptoms may be variable in their appearance and severity but usually have a drastic effect on personal relationships and business and professional relationships. Schizophrenia has a lifetime prevalence of approximately 1%, typically appears at 20 to 35 years of age, and is more frequent in men than in women. Approximately 15% of patients with schizophrenia commit suicide.
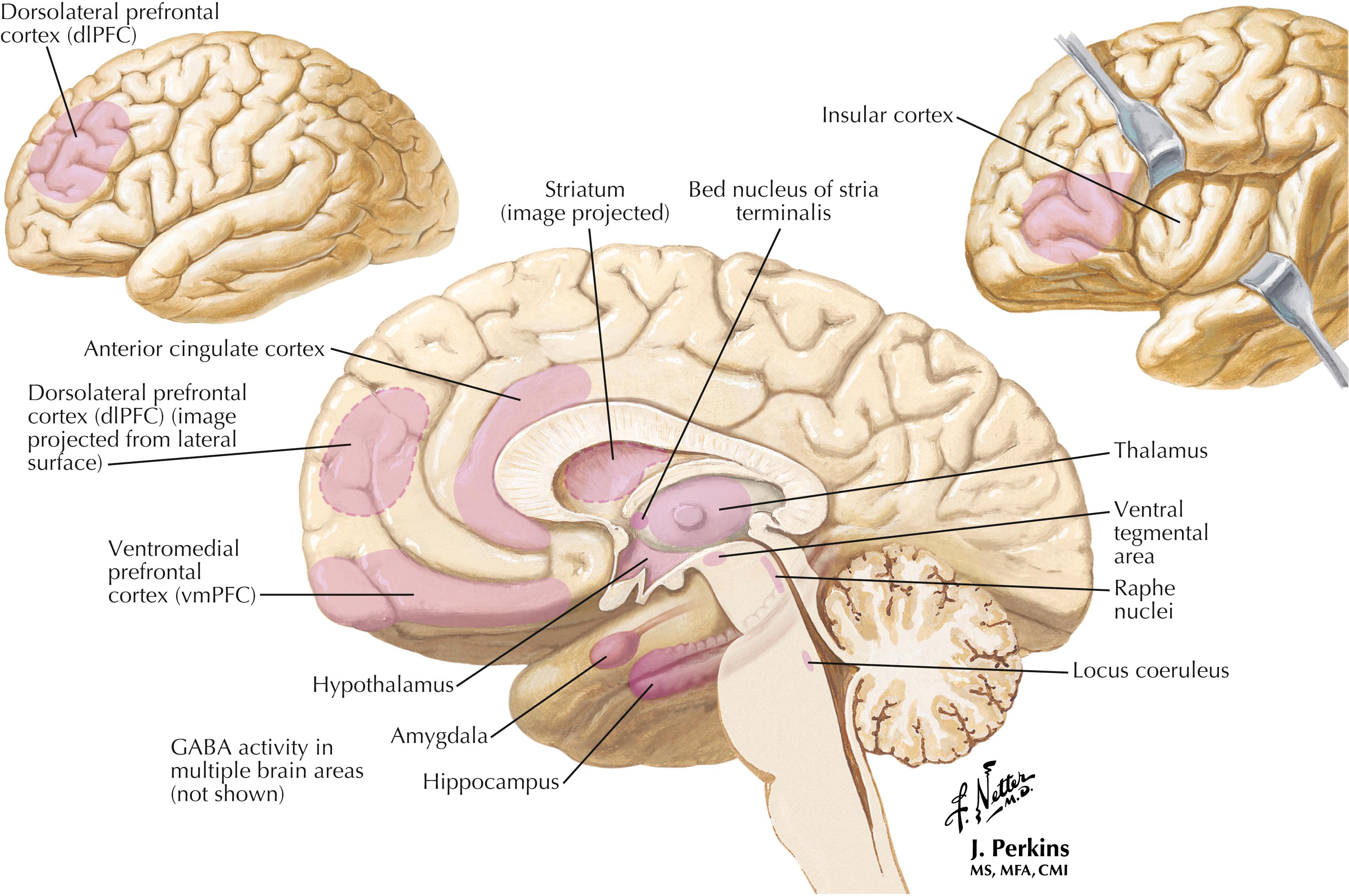
Areas of the brain involved in schizophrenia include:
Prefrontal cortex (both ventromedial prefrontal cortex [vmPFC] and dorsolateral prefrontal cortex [dlPFC]) and its connections with temporal cortex, parietal cortex, and striatum
Medial temporal cortex
Other cortical areas—posterior cingulate cortex, inferior parietal cortex, angular gyrus, anterior parahippocampal gyrus, and cortico-cortical excitatory pathways
Corpus callosum—slower interhemisphere processing
Hippocampus—disorganized pyramidal neurons in CA1, CA2, subiculum, entorhinal cortex
Amygdala—diminished emotionality
Thalamus—especially dorsal and medial dorsal (MD) regions
Striatum—striatal enlargement may result from antipsychotic meds
Enlarged lateral and third ventricles—may be the consequence of neuronal loss
Ventral tegmental area (VTA) and its mesolimbic and mesocortical pathways
Raphe nuclei—dorsal raphe nucleus, central superior nucleus
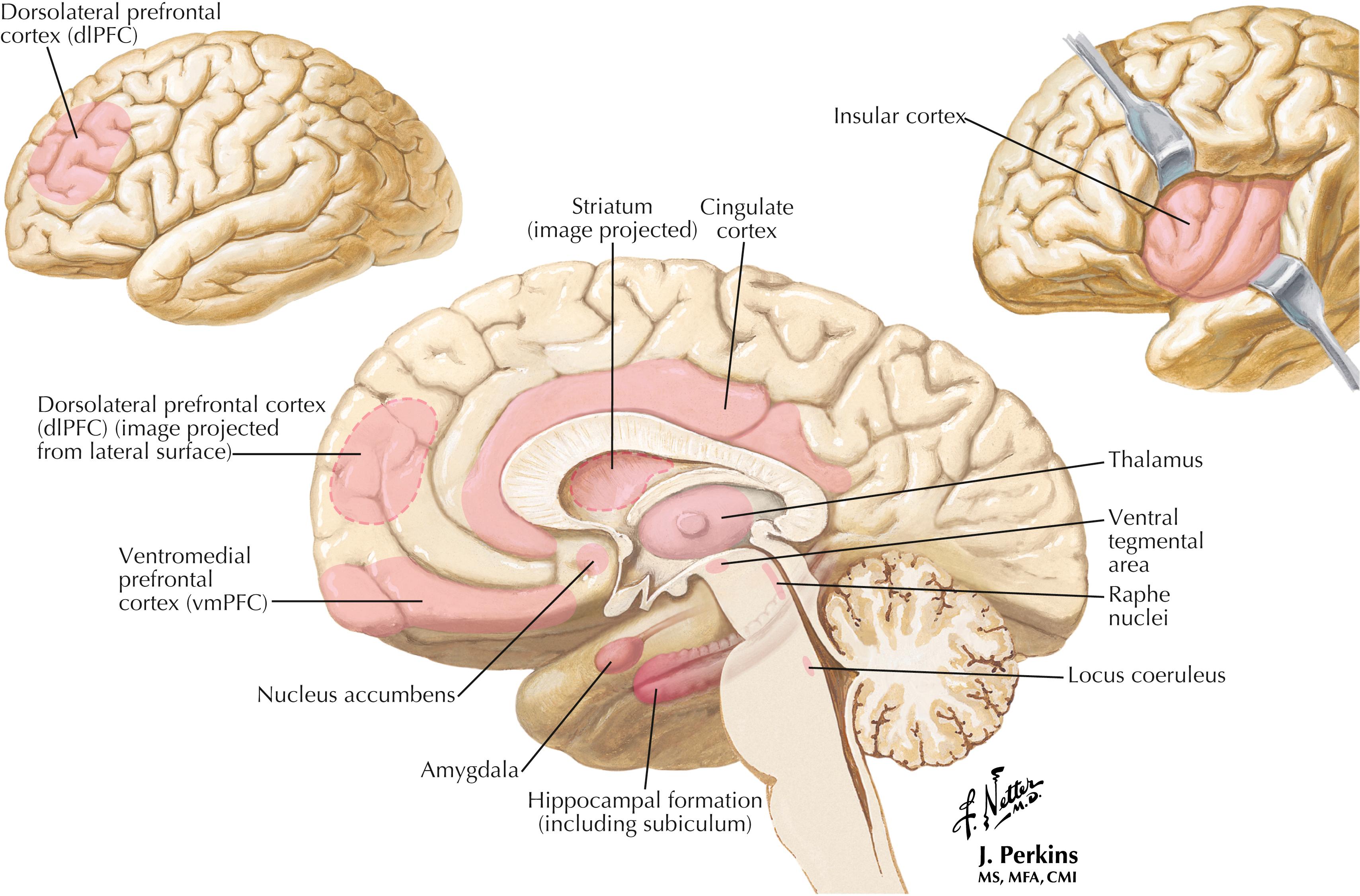
Major depressive disorder (MDD) is a common neuropsychiatric disorder, with onset often in early adulthood, that occurs in approximately 5% of the population. MDD is more prevalent in women and is associated with a genetic component. Many medical conditions may provoke MDD. The clinical onset includes at least 2 weeks with sadness and a loss of pleasure (anhedonia), accompanied by at least five of the following symptoms: (1) diminished concentration, (2) lethargy and fatigue, (3) altered appetite and weight changes, (4) sleep dysfunction, (5) restlessness, (6) feelings of worthlessness or guilt, (7) difficulty making decisions or thinking, and (8) suicidal thoughts or an actual attempt. MDD is a chronic illness with a tendency to recur, sometimes becoming worse at it progresses. A major treatment approach is pharmacologic, such as the use of selective serotonin reuptake inhibitors (SSRIs).
Brain areas involved in MDD include:
Prefrontal cortex—both vmPFC and dlPFC
Insular cortex
Cingulate cortex and its connections regulating autonomic and neuroendocrine systems
Corticolimbic connections
Hippocampal formation, including the subiculum
Amygdala
MD thalamus and its connections to PFC, amygdala, and striatum
Striatum
Nucleus accumbens and its midbrain dopaminergic (DA) mesolimbic connections for reward and motivation
Raphe nuclei—dorsal raphe nucleus and central superior nucleus (serotonergic)
Locus coeruleus and its noradrenergic connections
VTA and its dopaminergic mesolimbic and mesocortical connections
Bipolar disorder often appears as recurrent manic episodes seen before a major depressive disorder. Bipolar I disorder is the occurrence of one or more full-blown manic episodes, accompanied by expansive or irritable mood, grandiosity, racing thoughts, excess energy and a decreased need for sleep, distractibility, poor judgment, and risk-taking. Bipolar II disorder involves prior hypomanic behavior and depressive episodes but no major manic episode. In some situations, both manic/hypomanic and depressive components may occur together.
Areas of the brain involved in bipolar disorder include many of the areas noted above for MDD, including PFC, cingulate cortex, reduced cortical thickness (frontal, temporal, and parietal), hippocampal CA regions, amygdala, and ventral striatum.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here