Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Functional limb salvage mandates a multidisciplinary team approach that comprises vascular surgery, plastic surgery, foot and ankle surgery, infectious disease, general medicine, endocrinologist, rheumatology, physical therapy, pedorthotist, and prosthetist.
A successful functional limb salvage is one that restores function whether it be via soft-tissue reconstruction or minor or major amputation.
Successful healing of a foot and ankle wound is dependent upon accurate determination of wound etiology and biomechanics, establishing a clean wound base and achieving angiosome-based blood supply.
The reconstructive plan must be individually tailored to provide the best biomechanical result given the patient’s age, goals, and functional capacity. This may involve local wound care, skin grafting, local/regional flaps, free tissue transfer, and minor and major amputations.
Postoperative wound care and biomechanical offloading are essential to ensure successful reconstruction and prevent unnecessary complications such as wound breakdown and delayed healing.
Current advances in major amputations have now given us more options as a major amputation may be more functional than a salvaged foot.
The distal lower extremity has unique structural and functional significance, serving as a dynamic platform for posture and ambulation that is subject to repetitive trauma from large stress loads. Considering the complex anatomical variations and functional demands of the foot and ankle, restoration of defects in this region poses a significant reconstructive challenge. Trauma, infection, oncologic resection, autoimmune disease, as well as alterations in blood supply, sensation, and mechanical alignment can compromise skeletal stability and increase the likelihood of soft-tissue breakdown.
The importance of maintaining function to be able to walk and exercise cannot be overstated. Thirty minutes of exercise three times a week can add two life years while five or more times a week can add up to five life years. In diabetics, functionality significantly increases the five-year survival of both minor and major amputees over the national average. This is especially important because 40% of diabetics are obese, and 40% of diabetics spend less than 10 minutes per week exercising.
When salvaging a limb, it is critical to assess the type of function the reconstructed limb can achieve. One has to accurately determine the activities that the patient desires and is physically capable of. This determines which reconstructive options will best meet those goals: limb salvage versus amputation. The function achieved with below-knee amputations (BKA) has improved dramatically with the application of myodesis, vascularized fibular graft, targeted muscle reinnervation (TMR), and the use of ever more sophisticated prostheses. Because of this, pursuit of limb salvage as the primary objective, regardless of functional status, is no longer an acceptable goal.
The surgeon’s goal is to give patients a functional limb that meets their realistic physical goals, whether it be a reconstructed or amputated limb. The younger and/or more athletic the patients, the more they will demand of their reconstructed leg. As such, the reconstructed limb may not be able to meet their desired goal, and the decision to undergo an amputation may be more appropriate. However, the older the patient, the less he/she may demand of the reconstructed leg. As a result, a less-than-perfectly functional leg may be sufficient to carry on acts of daily living and avoids the necessity of relying on a prosthesis.
History has demonstrated that routine evaluation and treatment by a comprehensive multidisciplinary team improves the quality and cost-effectiveness of care and can reduce amputation rates by 36% to 86%. Successful foot/ankle reconstruction and functional limb salvage begins with a multidisciplinary team approach that includes collaboration between a vascular surgeon skilled in endovascular intervention and open vascular bypass, a foot and ankle surgeon competent in biomechanical surgery and internal/external skeletal stabilization techniques, a plastic surgeon familiar with principles of modern wound healing and soft-tissue reconstruction, and an infectious disease physician who specializes in surgical infections. In addition, medicine, endocrinology, nephrology, cardiology, hematology, rheumatology, and dermatology consultations may be indicated to address the patient’s comorbid medical conditions. For the at-risk or biomechanically unstable foot, a podiatrist and pedorthotist specializing in routine foot care and orthotics/shoe wear are critical in preventing ulceration and/or recurrent wound breakdown. In the setting of major amputation, a skilled prosthetist is necessary for the creation of a customized prosthesis capable of optimizing the biomechanical potential of the residual limb.
The reconstructive plan must be individualized to provide the best biomechanical result given the patient’s age, goals, and functional capacity. This may involve local wound care, grafting, local/regional flaps, free tissue transfer, and/or amputation for similar wounds presenting in different hosts. Surgical goals in foot and ankle reconstruction center on the “Three B’s”: (1) blood supply, (2) bioburden, and (3) biomechanics. This is achieved by ensuring adequate local blood flow, aggressive debridement to a clean wound base, and correction of biomechanical and structural abnormalities during surgical reconstruction, which offers the best opportunity for a durable, efficient, and functional foot. With these considerations in mind, most reconstruction can successfully be accomplished utilizing simple techniques (90%), while the rest require complex flap reconstruction (10%).
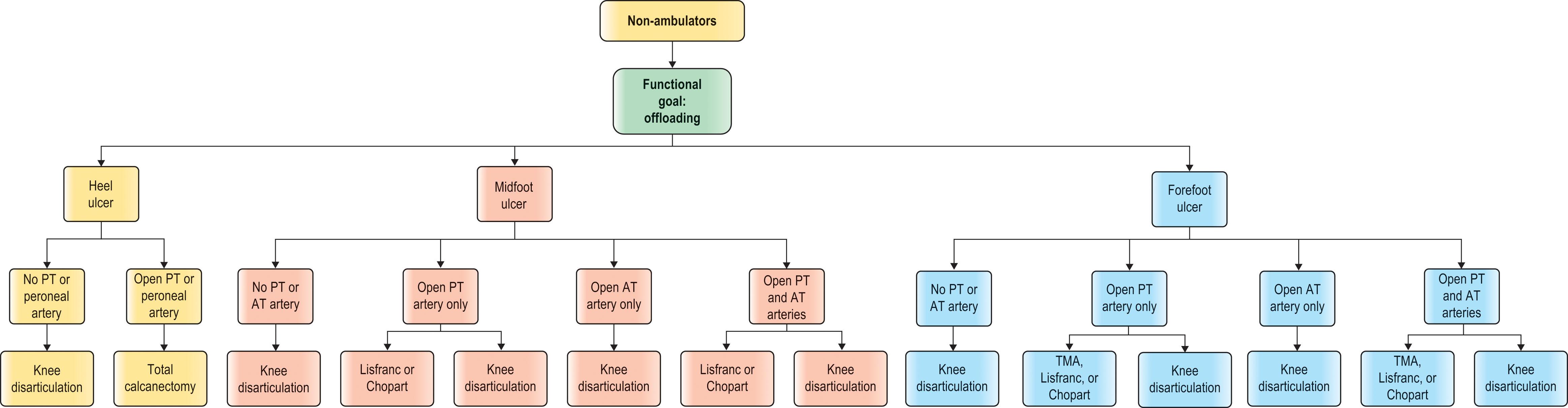
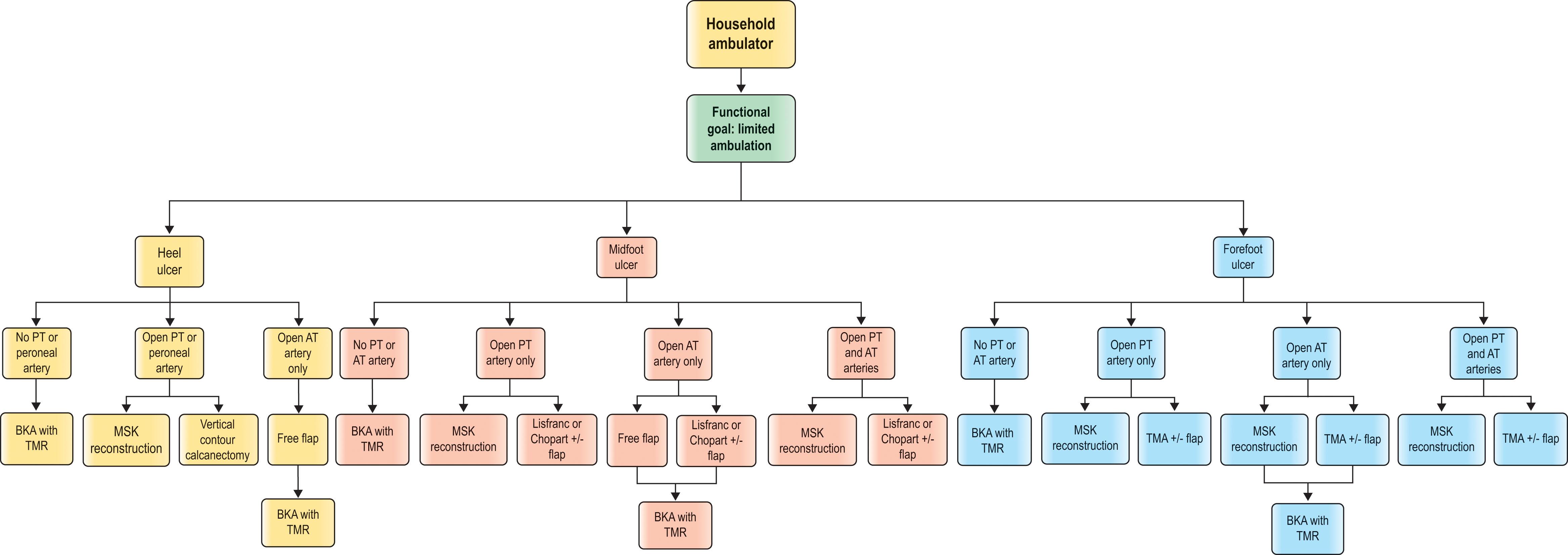
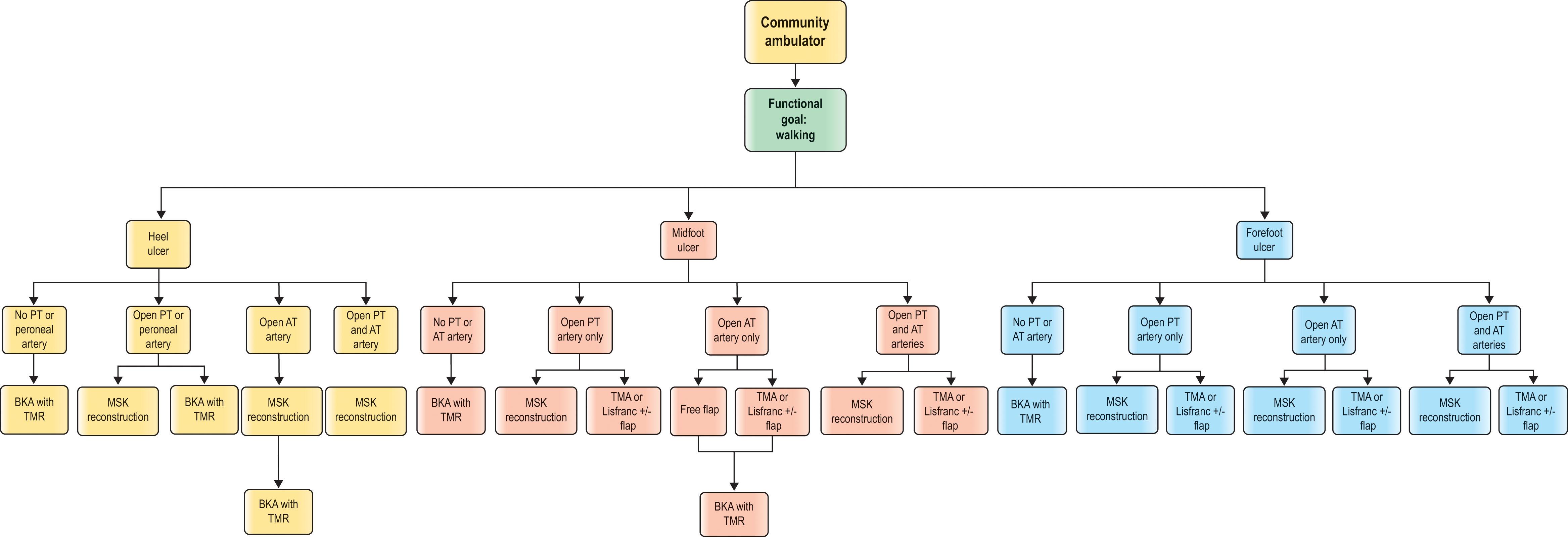
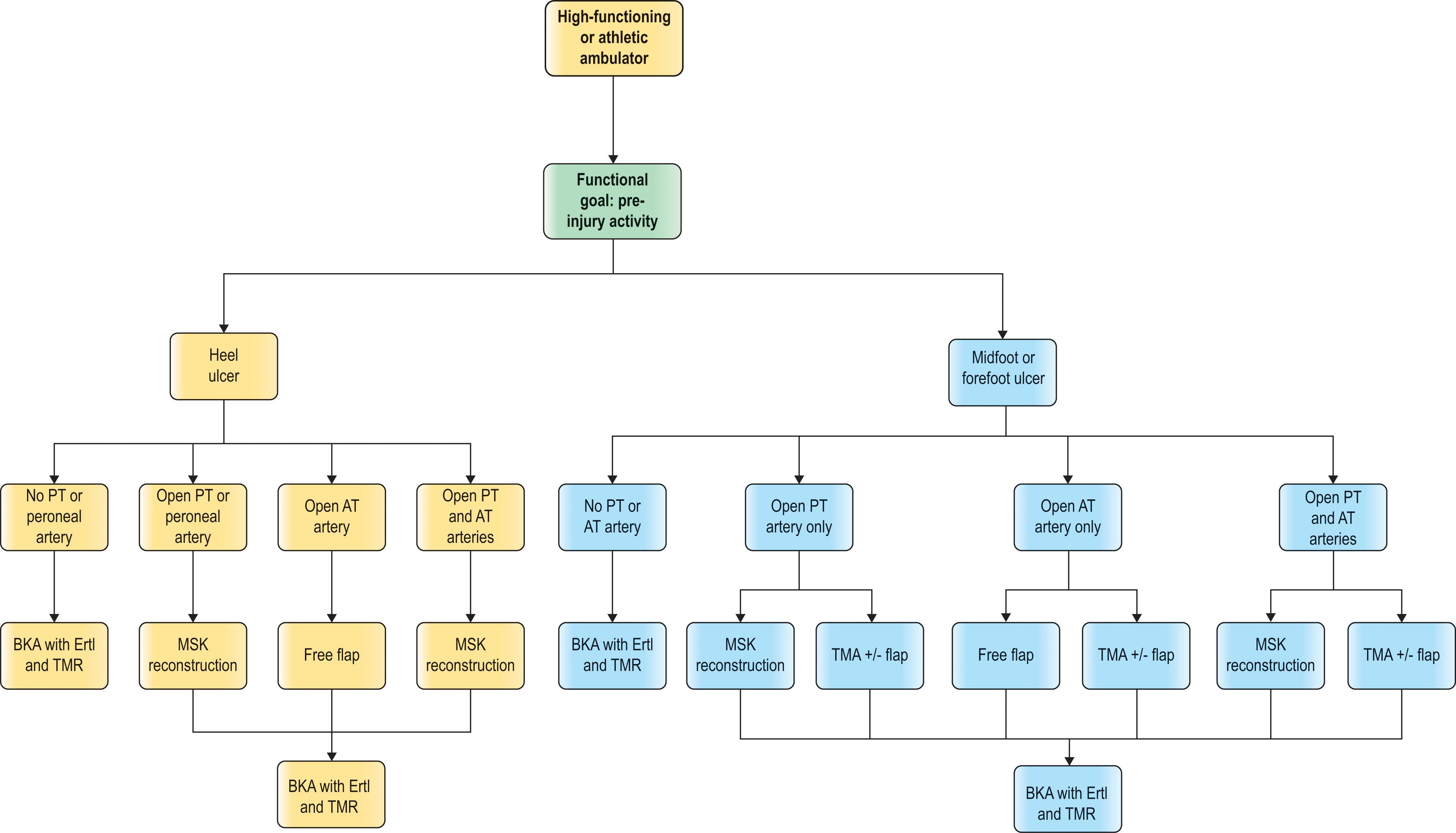
Four surgically based algorithms have been provided, based on function and available blood flow. They presuppose having a multidisciplinary team approach with plastic surgery (microsurgery and peripheral nerve), podiatric and/or orthopedic foot and ankle surgeon(s), and vascular surgery (arterial endovascular and bypass and venous surgery). Function is broken down into four categories: non-ambulator, household ambulator, community ambulator, and high-functioning or athletic ambulator ( Algorithms 8.1–8.4 ). The functional goals for each, respectively, are offloading, limited ambulation, normal ambulation, and pre-injury activity level.
The blood flow is broken down by which arteries are open or closed. An open posterior tibial artery allows for the most varied reconstructive options. All reconstructions include functional corrections (bone and tendon) where necessary to avoid recidivism. The soft-tissue component of the reconstruction includes any combination of skin graft, local flaps, pedicled flaps, or free flaps. These reconstructions are labeled in the algorithm as musculoskeletal (MSK) reconstructions. All foot amputations are done with correction for tendon imbalance. Below-knee amputations are performed with posterior flap, myodesis, and TMR. Ertl is added for the most functional group.
G. Ian Taylor first introduced the concept of “angiosomes” in human anatomy to describe a three-dimensional unit of tissue supplied by a single source artery. This was further developed as it applies to the foot and ankle to define the six specific angiosomes of the foot originating from three primary source arteries. The principal vascular supply to the foot and ankle begins with the popliteal artery and then branches out into three terminal branches: (1) the anterior tibial artery, (2) the posterior tibial artery, and (3) the peroneal artery. These further split up to feed the six angiosomes of the foot ( Fig. 8.1 ).
 Each of the three branches of the posterior tibial artery supply specific parts of the plantar foot: the calcaneal branch supplies the plantar heel, the medial plantar artery supplies the instep, and the lateral plantar artery supplies the rest of the plantar foot. Note that the lateral border of the calcaneal and lateral plantar branches end at the lateral glabrous junction. (B) The dorsalis pedis supplies the dorsal foot. (C) The calcaneal branch of the peroneal artery feeds the lateral heel, and the anterior perforating branch feeds the anterior lateral ankle.")
Above the ankle, the peroneal artery bifurcates into (1) the anterior perforating branch and (2) the calcaneal branch. The anterior perforating branch pierces through the distal anterior intermuscular septum and sends a branch superiorly overlying the intermuscular septum (this encompasses the area from which the lateral supra-malleolar flap can be harvested). The anterior perforating artery then connects directly with the anterior lateral malleolar artery off of the anterior tibial artery and supplies the anterolateral ankle angiosome. At the level of the lateral malleolus, the lateral calcaneal artery emerges laterally between the Achilles tendon and peroneal tendons. It curves with the peroneal tendons 2 cm distal to the lateral malleolus and gives rise to four or five small calcaneal branches. The lateral calcaneal artery terminates at the level of the fifth metatarsal tuberosity, where it connects with the lateral tarsal artery (dorsalis pedis). The lateral calcaneal branch supplies the lateral and plantar heel angiosome.
The posterior tibial artery connects with the peroneal artery via three arterial–arterial connections deep to the distal Achilles tendon. It then splits into three terminal branches: (1) the calcaneal branch, (2) the medial plantar artery, and (3) the lateral plantar artery. The medial calcaneal artery arises inferiorly and arborizes into multiple branches that travel in a coronal direction to supply the medial and plantar heel. Thus, the plantar heel receives dual blood supply from the calcaneal branches of the posterior tibial and peroneal arteries ensuring adequate flow to an area regularly traumatized during ambulation. Development of posterior heel gangrene usually implies severe vascular disease involving both the peroneal and posterior tibial arteries. The posterior tibial artery then enters the calcaneal canal, underneath the flexor retinaculum, and bifurcates into the medial and lateral plantar arteries at the level of the transverse septum between the abductor hallucis longus and flexor digitorum brevis muscles. The medial plantar artery’s angiosome encompasses the instep, while the lateral plantar artery supplies the lateral plantar surface as well as the plantar forefoot.
At the level of the lateral malleolus, the anterior tibial artery gives off (1) the lateral malleolar artery that joins with the anterior perforating branch of the peroneal artery. At the same level, the medial malleolar artery arises and anastomoses with the posteromedial artery of the posterior tibial artery. The anterior tibial artery then emerges under the extensor retinaculum of the ankle to become (2) the dorsalis pedis artery, which supplies the entire dorsum of the foot. The dorsalis pedis artery dives into the proximal first inter-metatarsal space to connect with the lateral plantar artery.
In the absence of vascular anomalies or disease, blood flow to the foot and ankle is redundant with multiple arterial–arterial connections that provide a margin of safety in the setting of distal source vessel occlusion ( Fig. 8.2 ). For example, the anterior perforating branch (peroneal artery) connects with the anterior tibial artery via the lateral malleolar artery at the ankle. At the Lisfranc joint, the dorsalis pedis artery dives into the first interspace to connect directly with the lateral plantar artery (posterior tibial artery). This vascular arch is critical in determining the direction of flow within the anterior and posterior tibial arteries, which can be antegrade, retrograde, or both. Furthermore, the plantar and dorsal metatarsal arteries are linked to one another at the Lisfranc joint by proximal perforators and at the web space by distal perforators. The posterior tibial and peroneal arteries connect via one to three arterial–arterial connections crossing deep to the distal Achilles tendon. Because of these arterial–arterial connections, the obstruction of the antegrade flow in a proximal artery can be restored distally via one of the above arterial–arterial connections ( Fig. 8.3 ).
 The important arterial–arterial connection between the dorsalis pedis and lateral plantar artery via a patent arch between the first and second proximal metatarsal. In the specimen, the bones have been removed. (B) The arterial–arterial connection between the anterior perforating branch of the peroneal with the anterior tibial artery via the lateral malleolar artery. (C) The arterial–arterial connection between the posterior tibial and peroneal arteries at the level of the ankle.")
 The angiogram picture of the three important arterial–arterial connections. (B) The peroneal artery can restore blood flow to both an occluded anterior tibial artery and a severely diseased posterior tibial artery via the arterial–arterial connections.")
Evaluation of blood flow is critical to optimize the success of any planned treatment or procedure. Using a Doppler ultrasound probe and selective occlusion, it is possible to determine the patency of these interconnections, the direction of blood flow, and selection of incision placement. An appropriate incision along the boundary of two adjoining angiosomes ensures optimal blood flow from either side, thereby facilitating safe exposure of underlying skeletal structures as well as the design of vascularly reliable flaps. Among patients with infrapopliteal disease, angiosome-directed revascularization has manifested higher rates of healing (91% vs. 38%) and fewer amputations (9.1% vs. 38.1%) than indirect revascularization. Similar findings have also been confirmed for infrapopliteal lesions treated with endovascular techniques. This detailed knowledge of vascular anatomy further aids the surgeon in determining the likelihood of limb salvage for a given wound and existing blood supply. When salvage is not possible, early recognition and effective design of amputations minimizes the risk of distal tissue necrosis and spares the patient needless, costly, and potentially dangerous procedures that have little chance of success.
Effective management of foot and ankle wounds is predicated upon an accurate determination of wound etiology, previously administered therapies, host comorbidities, and baseline biomechanics. The origin and age of the wound should be determined. Traumatic wounds should be defined in terms of acute versus chronic; high versus low impact; and mechanism of injury (i.e., biomechanical, thermal, caustic, radiation-induced, etc.). The patient’s tetanus immunization status should be obtained and updated as indicated. In chronic wounds, the age of the wound is important as long-standing wounds have the potential for malignant transformation (i.e., Marjolin’s ulcer). Previous topical therapies must be elucidated to determine if caustic agents (i.e., hydrogen peroxide, 10% iodine, Dakin’s solution, etc.) may have contributed to wound chronicity.
A careful medical history should be obtained to identify disease states that negatively affect wound healing (i.e., diabetes mellitus, peripheral vascular disease, autoimmune conditions, immunocompromised state, hematologic disorders, malnutrition, and so on). The presence of rheumatologic autoimmune conditions such as rheumatoid arthritis, pyoderma gangrenosum, systemic lupus erythematosus, and scleroderma are frequently associated with inflammatory wounds that initially necessitate medical rather than surgical management. Optimizing coagulopathies (i.e., factor V Leiden, protein C/S deficiency, anti-thrombin III deficiency, anomalous factor II, etc.) in patients with vasculitic wounds is critical for progression of normal wound healing. A complete list of medications and drug allergies should be obtained, as medications used in the treatment of autoimmune disease (i.e., steroids and/or chemotherapy) frequently impair healing. Nutritional status must also be optimized to promote healing (albumin > 3.5 g/dL and/or total lymphocyte count >1500). Once the infection has been treated, blood glucose levels should be kept below 200 mg/dL to minimize postoperative complications. Smoking significantly decreases local cutaneous blood flow and should be documented and addressed with each patient. Given the complexity of various disease processes, multiple specialties are often called upon to assist in optimizing the patient’s medical condition in order to improve the chances of successful wound healing.
Assessment of the patient’s current and anticipated level of activity is important to determine if the leg should be salvaged and to what extent it should be reconstructed. If a soft-tissue, tendon, and skeletal reconstruction can achieve the desired function and the patient’s health can tolerate the reconstruction, that should be the option chosen. However, for the younger and/or active patient, an inadequate functional limb for the desired physical activity may be counterproductive, and the patient may do better with a below-knee amputation (myodesis, TMR, and Ertl). For the less active patient who only desires to be able to perform the daily acts of living, a less than fully functional limb may be enough. For the latter patients, salvage may only need to be functional enough for limited ambulation with a walker or transfer. For non-ambulators, if the limb is non-functional, strong consideration should be given to performing a knee disarticulation or above-knee amputation (AKA) to cure the problem and minimize the risk of recurrent breakdown and/or development of a life-threatening infection.
The complete physical exam starts with a careful three-dimensional wound measurement (length, width, and depth), as well as evaluation of involved tissue types (i.e., epidermis, dermis, subcutaneous tissue, fascia, muscle, tendon, joint capsule, and/or bone). A metallic probe can be used to assess underlying skeletal involvement. Direct palpation of bone at the base of the wound is highly sensitive (87%) and specific (91%) for the presence of osteomyelitis. Diabetic ulcers with an area greater than 2 cm 2 have a 90% chance of harboring osteomyelitis, regardless of findings on the probe-to-bone test. The level of tissue necrosis and potential avenues for the spread of infection (i.e., flexor and/or extensor tendon surfaces) must be determined. The presence and extent of cellulitis must be noted and differentiated from dependent rubor by direct leg elevation above the level of the heart. If cellulitis is present, the erythema will not resolve with elevation, and its borders should be delineated with a marker, dated, and timed accordingly. This permits the clinician to accurately monitor the progress of infection and/or response to initial treatment and antibiotics.
The vascular status of the foot must be accurately evaluated. The presence of palpable pulses (i.e., dorsalis pedis and/or posterior tibial artery) signals that blood flow is likely adequate to promote healing. If pulses are not palpable, however, the Doppler signal over the posterior tibial artery, dorsalis pedis artery, and anterior perforating branch of the peroneal artery should each be assessed. Doppler ultrasound allows the surgeon to evaluate both the quality and direction of flow through major and minor arteries in the foot to assess the perfusion of the wound’s angiosome and to assess possible flap harvest ( Fig. 8.4 ). In the setting of atherosclerosis, the normal triphasic waveform may deteriorate distally to a biphasic or monophasic or aphasic waveform. Triphasic flow along the artery being evaluated indicates normal blood flow. If there are any questions, these patients should be referred to vascular lab for noninvasive studies to confirm triphasic flow. Patients with monophasic or biphasic flow and a non-healing wound or in preparation for a free flap should undergo an angiogram. There is no need to lose time obtaining noninvasive testing. We have found this to be a very effective and accurate way of determining blood flow. An angiogram can be done with 6 to 8 cc of dye, which poses minimal risk to the kidneys.
 An ulcer over the distal anterior tibial artery angiosome that is not healing despite a palpable posterior tibial pulse. (B) Angiogram shows that both the anterior tibial artery and the peroneal artery are occluded.")
Diabetics often have non-compressible arterial walls secondary to mural calcification, which may lead to falsely elevated, and thus unreliable, ABI values. If the palpation or Doppler examination of the proximal and distal pulses suggest ischemia, arterial imaging should be obtained to evaluate whether a vascular inflow (absent or weak femoral pulse) and/or outflow (absent or weak distal pulse) intervention is required. CT angiogram is more useful for proximal disease, while arteriogram is more valuable for distal disease. Discussing the angiogram with the respective vascular interventionist is critical to convey exactly what type of blood flow is needed for the reconstructive surgery to be successful. With advances in endovascular techniques, revascularization with dilatation, recanalization, and atherectomy of stenosed/obstructed arteries can be performed in patients who would otherwise be poor candidates for open vascular bypass.
As part of our algorithm for planned microvascular reconstructions, we obtain a diagnostic angiogram for all patients. Duplex Doppler exam can also be helpful, especially when monitoring an angioplastied vessel. In situations where intervention is deemed necessary, targeted percutaneous transluminal angioplasty (PTA), with or without stent placement, is employed in the same setting to restore both direct and peripheral inflow. Stenting of infrapopliteal vessels has a poor patency history and should be avoided. Angioplasties tend to have a shorter half-life (30% occlusion rate at 3 months). Bypass surgery is always an excellent option with high 5-year patency rates (>60%). The optimal flow to the downstream foot (as measured by TcO2) with bypass surgery occurs at 5 to 8 days post bypass versus as long as 30 days post angioplasty. Whenever a patient who has had an angioplasty presents with a healed wound or skin graft breakdown, the first thought should be that the angioplastied vessel is occluded.
The role of angiogram, angioplasty, and/or bypass in microsurgery is further discussed in Chapter 9.3 .
Sensibility is evaluated with a 5.07 Semmes–Weinstein filament that represents 10 g of pressure. If the patient cannot feel the filament, protective sensation is absent, and the risk of breakdown and/or ulceration is significantly increased. Motor function is assessed by looking at the resting position of the foot and by testing the strength and active range of motion of the ankle, foot, and toes.
For a thorough discussion, see the sections regarding biomechanics and skeletal stability of the diabetic foot in Chapter 9.1, Chapter 9.2 .
Crush injuries or ischemic insults to the foot can elevate pressures within myofascial compartments; and, like that in the leg, compartment syndrome in the foot must be evaluated and treated if necessary. The signs and symptoms of compartment syndrome of the foot are similar to those elsewhere in the body (i.e., 6 P’s: pain, paresthesia, pallor, paralysis, pulselessness, poikilothermia). Pain out of proportion to the clinical examination is often the first symptom. Weakness of the toe flexors/extensors and pain with passive dorsiflexion of the toes represent important physical signs. Pallor, paresthesia, a palpably tense compartment, and absent digital pulses on Doppler assessment eventually occur. When measuring pedal compartment pressures, it may be difficult to determine the compartment in which the pressure is being recorded. Therefore, compartment pressure recordings should be obtained by a physician who understands the compartmental anatomy of the foot.
If clinical indications are present, a four-compartment release should be performed. The medial approach to the foot, as advocated by Henry, allows decompression of all four compartments through a single incision. Mubarak and Hargens advocate two longitudinal incisions on the dorsum of the foot through which the interosseous compartments may be decompressed (analogous to that in the hand). Whitesides anecdotally described compartment syndrome of the foot, secondary to burns and direct trauma, and recommended decompression using the medial approach of Henry.
For adequate compartment decompression, an incision is made along the medial glabrous junction of the foot, beginning at the first metatarsal head and extending to the heel. The skin and fascia are divided and the incision is carried down to release the abductor hallucis muscle and its tendon, thus decompressing the medial compartment. Retraction of the abductor hallucis towards the plantar surface exposes the medial intermuscular septum, which is divided to release the central compartment. The lateral compartment is released utilizing a linear incision along the lateral glabrous junction that extends from the fifth metatarsal head to the calcaneus. Through this incision, the fascia enveloping the lateral compartment is released. Decompression of the interosseous compartment is best achieved through two linear, dorsal incisions overlying the second and fourth metatarsals. The fascia overlying the four interosseous spaces is then opened.
Wound infection is characterized by the presence of replicating microorganisms within a wound, resulting in a subsequent host response such as erythema, warmth, swelling, pain, malodor, and purulent drainage. If not recognized and treated early, the infection will spread systemically leading to fever, leukocytosis, and possibly sepsis. The line between colonization and infection may be minute, so prompt identification is critical to healing wounds and minimizing complications. For most microorganisms, a bacterial count (bioburden) of 10 5 bacteria per gram of tissue or greater has been defined as the quantitative threshold for wound infection and inhibition of the wound healing process.
When managing infected foot wounds, it is important to determine the source and extent of infection. At the first evaluation, the erythematous border surrounding the wound should be delineated, timed, and dated for serial comparison. The original mark is used as a reference point for determining the effectiveness of antibiotics and/or prior debridement. Radiographic evaluation of the affected area will help identify skeletal involvement as well as the presence of soft-tissue gas. If gas is visualized radiographically within the tissue planes beyond the immediate location of an open ulcer, gas gangrene is most likely present and the wound becomes a surgical emergency. Gas is usually a byproduct of anaerobic bacteria (i.e., Clostridium perfringens ); it tends to be foul smelling and travels along the fascial planes. A CT scan can be very helpful in identifying the extent of gas and possible proximal infection. Compartment pressures in the affected area should be assessed, as high pressures in the diabetic foot with gas gangrene are frequently missed secondary to neuropathy.
If the wound is acutely infected with purulent drainage, malodor, and/or proximally ascending erythema, immediate and aggressive debridement is indicated to prevent sepsis, possible limb loss, or death. The involved compartments of the extremity should be released if there is any suspicion of elevated compartment pressures. Wounds with foul-smelling odors should be debrided aggressively enough to get rid of all malodor. Persistent malodor signals the need for further debridement and excision of any remaining necrotic or infected tissue. It is important to remember that the presence of gas gangrene should not be an indication for drainage amputation. Aggressive serial debridement to normal tissue colors (red, yellow, and white) is critical, and may leave enough healthy tissue for possible reconstruction using spare parts surgery ( Fig. 8.5 ). A second look within 24 hours is always recommended. Adjunctive hyperbaric oxygen therapy may help in controlling the anaerobic infection but is unnecessary if the initial debridement was adequate.
 Patient presented with a rapidly expanding necrotizing fasciitis from an incision in the forefoot. The patient was taken to the operating room immediately, and all of the necrotic tissue was excised. Despite very aggressive debridement, the first and 5th toes were spared (C) . The patient underwent serial debridements until the tissue was culture negative. (D) A transmetatarsal amputation was performed using the soft tissue of spared hallux and 5th toe and Achilles tendon lengthening. (E,F) The patient’s limb was salvaged at a very functional long transmetatarsal amputation level.")
Aerobic and anaerobic cultures of the wound should be obtained during each debridement by taking samples deep to the surface of infected tissue and purulence. Superficial swabs and tissue cultures are of limited use, as they usually reflect surface flora rather than the underlying bacteria that are responsible for infection. Broad-spectrum antibiotics should be started after deep tissue cultures are obtained and subsequently narrowed based upon culture results and sensitivities. It is important to be aware that deep cultures may miss up to two-thirds of the bacteria species present within a wound. Therefore, persisting signs of infection after 24 to 48 hours of antibiotic therapy signal a need to reconsider the choice of antibiotics and the possibility of further debridement.
For suspected osteomyelitis, cultures of both debrided bone and normal proximal bone should be obtained. It may be helpful to label the osteomyelitic bone culture as “pre-debridement” and the normal proximal bone culture as “ post-debridement” so that the quality of debridement can be assessed, and the length of antibiotic treatment determined. If a wound is closed and the “post-debridement” culture is showing no growth (i.e., only healthy bone remains at the base of the wound), then a one-week course of appropriate antibiotic therapy is often sufficient. In contrast, if the “clean” culture is positive for bacterial growth, then re-resection of bone or a six-week course of antibiotics may be necessary. If the surgeon suspects that the bone left behind still harbors osteomyelitis despite negative cultures (i.e., calcaneus or tibia), then a six-week course of antibiotic therapy may be needed for eradication of infection. The appropriate antibiotic choice and duration is best determined and monitored by an infectious disease specialist, who is also familiar with managing the untoward side effects of prolonged antibiotic therapy. A recent randomized study on antibiotic treatment of osteomyelitis showed equal efficacy between oral and intravenous antibiotics.
By definition, open wounds are contaminated, meaning that the bed contains planktonic bacteria and biofilm. Acute wounds have only 6% biofilm present, whereas up to 90% of chronic wounds may have biofilm present. Biofilm is characterized as a microbial community embedded within an extracellular polymeric matrix that is irreversibly adherent to both living and non-living surfaces. This structurally heterogeneous matrix promotes enhanced cell-to-cell signaling between bacteria (i.e., quorum sensing), allowing biofilms to grow and act as independent organisms. Biofilms require highly specific growth media that are not commonly found in the hospital setting; and, as a result, typical specimen cultures are often inadequate for the positive characterization of bacteria. Polymerase chain reaction (PCR) technology, however, permits rapid identification of causative organisms within a matter of hours. PCR studies of biofilm have identified over 60 different bacterial species, more than 60% of which are anaerobes.
These multi-species colonies coexist at a far lower energy state and serve as a medium for extrachromosomal DNA plasmids that confer antibiotic resistance up to 1000 times greater than that of planktonic bacteria alone. Within 24 to 48 hours, the biofilm matures and becomes resistant to both topical and systemic antibiotic penetration as well as phagocytosis by the host immune response. The colony then spreads passively through fragmentation (70%) or by active individual seeding of undifferentiated planktonic cells (30%). Biofilm can be as deep as 4 mm below the wound surface. Biofilm causes inflammation of the surrounding tissue. While the classic signs of infection may not predominate, increased pain/tenderness, exudate, abnormal odor, and/or friable granulation tissue often signal its presence. This usually requires aggressive mechanical debridement to stimulate healing of healthy underlying tissue.
The goal of treating any wound is to promote healing in a timely fashion. The first step toward realizing this objective is to establish a clean and healthy wound base. An acute wound is defined as a recent wound that has yet to progress through the sequential stages of wound healing. In the setting of adequate blood flow, a clean base can be established with simple debridement techniques and the wound closed either immediately or following application of a local dressing to facilitate healing by secondary intention or closure at a later date. In contrast, a chronic wound is one that is arrested at some stage of healing (usually the inflammatory stage) and cannot progress further.
Converting a chronic wound to an acute wound mandates the correction of underlying medical comorbidities (i.e., hyperglycemia, coagulopathies, changing or modifying drug therapy, etc.), restoration of adequate blood flow, administration of appropriate antibiotics when indicated, and aggressive wound debridement. If the wound has responded appropriately, healthy granulation will appear, edema will decrease, and neo-epithelialization of the wound edges will occur. Measuring the wound area weekly is a useful means to monitor progress, as the normal rate of healing equates to a 10%–15% decrease in wound surface area per week. Assuming any underlying abnormalities have been corrected (i.e., infection, ischemia, coagulopathy), a healing rate below that expected may be helped by using adjuncts such as negative pressure wound therapy (NWPT), topical growth factors, cultured skin/dermal substitutes, hyperbaric oxygen, soft-tissue reconstruction, etc. Using an aggressive surgical algorithm in large wounds (49 cm 2 with 89% to bone or muscle) yielded healing rates at one year of 75%.
Necrotic tissue, foreign material, and bacterial burden impede the body’s attempt to heal through the production of proteases, collagenases, and elastases that overwhelm the local healing process. Aggressive mechanical debridement, therefore, is essential to overcome these barriers and stimulate normal healing. However, surgical debridement is the single most underperformed procedure in treating foot and ankle wounds because of wound closure over the resultant tissue defect. Tissue with clotted veins or arteries in the dermis or subcutaneous tissue, liquefied fascia or tendon, and nonviable bone should all be debrided. Indurated tissue along the wound edge should be serially deli-sliced until a soft-tissue edge is achieved. Debridement should be considered complete only when soft normal-colored tissue (red, yellow, white) remains. By the same token, any viable tissue should be preserved as it may prove useful at the time of definitive reconstruction. Spare parts surgery is very useful in preserving length in foot amputations (see Fig. 8.5 ).
The most effective debridement technique consists of tangential excision of all grossly contaminated and devitalized tissue, until only normal soft tissue is present. Gentle tissue handling, sharp dissection, skin hook retraction, and pinpoint cauterization of bleeding vessels serve to minimize trauma to the tissue and promote tissue viability. One should avoid harmful maneuvers such as crushing skin edges with forceps or clamps, burning tissues with electrocautery, and/or suture-ligating healthy perivascular tissues. Useful surgical tools include a scalpel blade, Mayo scissors, curettes, rongeurs, sagittal saw, power burr, and hydro-surgical debrider (Versajet, Smith & Nephew, Hull, UK). Serial debridement is performed regularly, and as often as necessary, until the wound is deemed clean and ready for closure.
Three technical adjuncts can be used in combination to ensure adequate debridement of the entire wound: (1) topical staining of the wound with methylene blue ( Figs. 8.6), (2 ) utilizing color to guide debridement, and (3) debridement via tangential excision of all indurated tissue to normal soft tissue. Prior to debridement, methylene blue is liberally applied to the wound base using a cotton tip applicator. This helps the surgeon adequately address all portions of the exposed wound base by ensuring complete removal of all visibly stained tissue from the wound base. As a further color guideline, the surgeon must get the wound base to normal tissue colors (i.e., red, white, and yellow). Using these colors as a guide provides an endpoint to debridement and helps prevent removal of healthy tissue ( Fig. 8.7 ). Finally, the surrounding indurated tissue is tangentially excised until tissue of normal texture is reached allowing healthy underlying cells to progress through the stages of normal wound healing.
 to paint the entire surface of the wound so that no area is missed during debridement is critical for removal of all surface biofilm. A Q-tip soaked in blue dye applies blue dye to the wound (A) until the entire surface is painted (B) . The wound is excisionally debrided until there is no residual dye post debridement (C) .")
 Serial excision of a chronic and/or infected wound with a scalpel, rongeur, and saw to normal-color tissue (red, yellow, white) is critical to establishing a clean base. (B) The bone still needs to be resected, but the rest of the tissue has the desired color and texture. This is the technique to successfully convert a chronic wound into an acute wound.")
After initial debridement to clean, healthy tissue, it is important to prevent subsequent buildup of metalloproteases that destroy naturally produced growth factors. Bacterial biofilm and proteinaceous debris that form on the wound surface must be removed at regular intervals. This can be done by scrubbing the wound daily with soap and water or using wet-to-dry dressings. In between debridements, topical antibiotics can help reduce the bacterial load. Bacitracin is most useful for minimally infected wounds, mupirocin for methicillin-resistant Staphylococcus aureus (MRSA) contamination, and silver sulfadiazine or gentamicin ointment for Pseudomonas infections. For most contaminated wounds, antibiotic beads, 1% acetic acid, 0.5% Dakin’s solution, Sulfamylon or Iodosorb work well. Short-term use of quarter- or half-strength Dakin’s solution may be appropriate for temporizing heavily contaminated and/or necrotic wounds in patients who require medical optimization prior to operative debridement. An absorbent dressing (i.e., alginate, Drawtex [Beier Drawtex Healthcare, Pinetown, South Africa]), hydrofiber, foam, hydrocolloid, etc.) with bactericidal ingredients (iodine) is effective for heavily exudative wounds.
For patients who are poor operative candidates, maggot debridement therapy (MDT), using larvae of the blowfly Phaenicia sericata , is a proven, cost-effective alternative for treating drug-resistant, chronically infected wounds. MDT serves to enhance healing through selective debridement of necrotic tissues and reduction of bacterial burden. A recent meta-analysis evaluating the safety and effectiveness of MDT revealed significant improvements in both the rate and efficiency of chronic wound healing, longer antibiotic-free intervals, and a lower amputation risk among patients with diabetic foot ulcers. Nevertheless, the prospect of maggot escape, failure to control secretions, and use of tenuous/labor-intensive dressings often precludes the use of maggots in geometrically complex locations.
Once the wound is clean and adequately vascularized, negative pressure wound therapy (NPWT) using a vacuum-assisted closure (VAC) device can help expedite formation of granulation tissue. NPWT increases local blood flow, reduces tissue edema, controls bacterial proliferation, and catalyzes the formation of granulation tissue. Level-one data demonstrate the ability of NPWT as a postoperative dressing before closure to hasten healing and reduce amputation rates in the setting of diabetic foot wounds. Furthermore, because the VAC is changed every 48 to 72 hours in the operating room, the wound is less susceptible to cross-contamination compared to when the dressing is changed two or three times each day on the hospital floor.
NPWT with instillation (NPWTi) represents an important evolution in management of complex acute/chronically infected wounds, those with underlying osteomyelitis, and wounds with exposed orthopedic hardware and/or joint implants, among others. NPWTi combines negative pressure (−125 mmHg) with automated, intermittent instillation of a topical wound solution (antimicrobial vs. saline) of set volume (until sponge is visibly saturated), dwell time (10 to 20 mins), frequency (every 1.5 to 2 hours), and duration (2 to 10 days). In a retrospective, historical, cohort-controlled trial examining the impact of negative pressure with (n = 68) and without (n = 74) instillation, NPWTi was shown to reduce the total number of operative procedures, expedite the time to wound closure, and shorten the length of hospital stay when compared with NPWT alone. A subsequent study comparing NPWTI to traditional care shows (1) shorter time to wound closure, (2) reducing bacterial count 4.4 times more effectively, (3) significantly lower length of therapy, (4) more than twice as likely to have wound closed. Similar results occurred in infected wounds when comparing NPWT to NPWTi.
While studies support the use of 0.1% polyhexanide-betaine as an irrigation solution in NPWTi in contaminated artificial joints, the use of saline has been shown to be at least equally effective in postoperative care. Future questions that remain to be answered pertain to the optimal volume and solution for instillation, dwell time, and duration of therapy, which should be assessed through appropriately conducted, high-powered, randomized controlled trials.
If the wound fails to show signs of healing despite being clean and having adequate blood flow, providing biologically active coverage, such as platelet-derived growth factor (Regranex, Ortho-McNeil Pharmaceutical, Raritan, NJ), cultured skin substitutes (e.g., Apligraf, Organogenesis, Canton, MA; Grafix, Smith and Nephew, Andover, MA), etc., may facilitate more rapid healing. The formation of new tissue over debrided wounds and/or partially exposed healthy bone or tendon can also be stimulated through the application of a dermal regenerative template (e.g., Integra or Primatix, Integra LifeSciences, Plainsboro, NJ), with or without VAC support, and allowing it to revascularize over the course of 2 to 3 weeks. The newly incorporated dermis can then be skin grafted with a thin autograft to provide coverage. Finally, level-one evidence has demonstrated the ability of systemic hyperbaric oxygen therapy (HBOT) to reduce amputation rates and promote granulation of certain complicated, non-healing wounds. It is particularly useful in radiation-induced wounds, frostbite, revascularized gangrenous feet, and failing flaps. HBOT stimulates local angiogenesis in the wound bed, promotes collagen cross-linking and extrusion from cells, and potentiates the ability of macrophages/granulocytes to kill bacteria. Any or all of these modalities may prove valuable when used in concert with more traditional reconstructive strategies.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here