Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

 Access video content for this chapter online at Elsevier eBooks+
Access video content for this chapter online at Elsevier eBooks+
Contemporary understanding and management of lower extremity wounds has experienced a renaissance in the last several years with a combination of advances in technology and an evolution of evidence-based knowledge leading to significant progressions in the assessment, treatment, and suppression of chronic non-healing lower extremity wounds. The application of these practices has precipitated better utilization of treatments, reduction in recidivism, and a greater appreciation of the non-healing foot and ankle wound environment.
There are numerous factors which may contribute to an acute wound’s degeneration into a chronic state. Some of the most common causes in the lower extremity include ischemia, infection, neuropathy, deformity, or any combination thereof. Diabetes mellitus, for example, bears an assortment of complications that affect a myriad of tissue types, all of which may blunt wound healing. In this way, patients with diabetes truly represent the personification of complex and non-healing wounds. It is important, however, to consider that although a great number of complicated and non-healing wounds emanate from the diabetic population, diabetes as a pathology in and of itself is an insufficient scapegoat for classifying the etiology of a lower extremity wound. Further investigation must be sought to define the causal relationship for wound formation and its chronicity. The terms “diabetic wound”, “diabetic ulceration”, or “diabetic foot” are classic misnomers that lead one to assume the etiology for a wound is the disease of diabetes or its complications. While complications associated with diabetes may in fact be the reason(s) for a wound’s chronicity and non-healing, it should not be assumed without a proper assessment, and these fairly antiquated “diabetic” terms should only be used as grossly generalized descriptors. Rather, non-leading terms should be used and descriptors like “complex wound”, “complicated wound”, “chronic wound”, or “non-healing wound” are preferable. In patients without diabetes, for instance, the burden of etiological proof placed upon the physician and team is just the same as it is for a patient with diabetes.
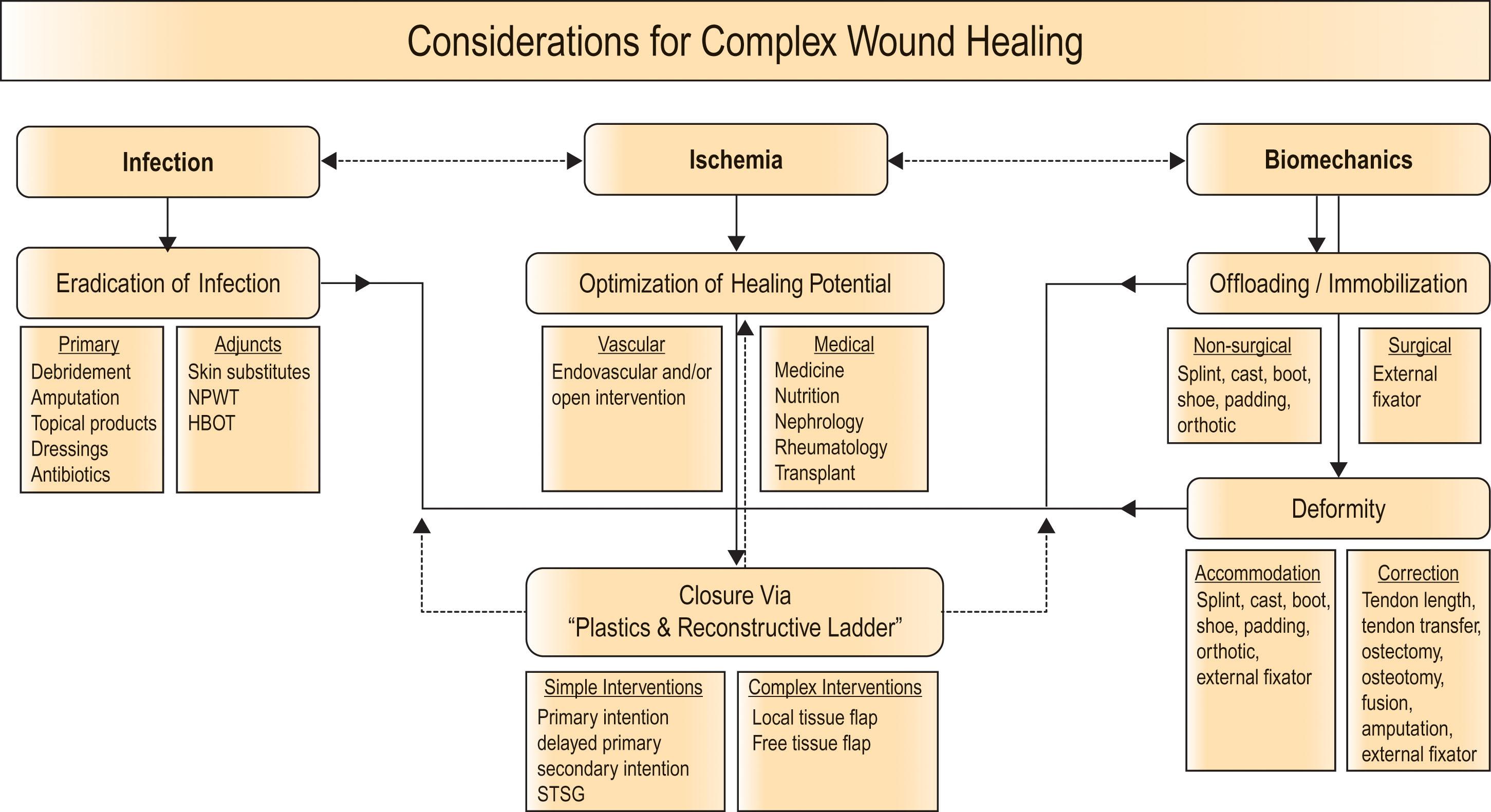
Certainly, the non-healing lower extremity wound is a complex structure and environment that is undeniably disadvantaged due to an assortment of potential local and systemic complications that may hinder wound healing. With this in mind, it is imperative that clinicians be vigilant and attentive to this dynamic patient population, modify wound healing strategies appropriately, and engage in aggressive and even varied treatment practices when warranted. In this chapter we review the principles in the management of non-healing wounds and amputations of the foot and ankle and offer an assortment of considerations and strategies aimed at their treatment and suppression with special attention to the biomechanical implications, considerations, and available treatments strategies ( Algorithm 9.2.1 ).
Infection is an obvious impediment to wound healing and as such must be addressed early and aggressively. As all open wounds will assuredly be colonized with microorganisms, we delineate infection by the presence of the classic signs of inflammation, including rubor (redness), tumor (swelling), dolor (pain), calor (heat), and function laesa (loss of function). The observation of superficial infection or cellulitis should include assessment for responses to elevation and dependency and monitoring by drawing a line of demarcation as a reference to advancing or receding infection. Wound depth should be probed utilizing a sterile instrument as this will enable the clinician to fully examine the extent of the wound and may aid in the diagnosis of bone infection.
Subjective questioning for constitutional symptoms associated with infection include inquiries of nausea, fever, diarrhea, constipation, cough, chills, cramps, and malaise. However, in many immunocompromised patients, these systemic factors present with a lesser frequency and severity as the patient may be unable to mount a sufficient immune response to infection. Patients should also be questioned about recent illness, hospitalization, or visit to the emergency room or urgent care, as these types of information can go undetected if not pursued. Baseline vital signs should always be evaluated.
Following the removal of all infected and nonviable soft tissue and bone, the appropriate and judicious use of antibiotics specifically targeting the offending organism(s) is necessary to slow the growing concerns of bacterial resistance. Appropriate consultation with an infectious disease will help ensure the best possible practices are implemented and at the same time will help to ensure antibiotic efficacy into the future.
The word debridement derives from the French débridement , which translates as “to remove a constraint”. This term was first used by Henri LeDran (1685–1770) in the context of an incision of skin and fascia to release swelling associated with injury. However, during the eighteenth and nineteenth century wartime this definition was refined to include removal of all materials incompatible with healing in order to prevent gangrene, and it is this definition that still guides practitioners today. Presently, debridement is the excision of dead, damaged, or infected tissues in order to optimize healing potential of the remaining presumably healthy and viable tissues. This is performed in an assortment of individual or combined methods and settings in preparation of a wound bed for closure. However, it is important to remember that debridement is merely one, albeit vital, factor in modern wound bed preparation.
Methods of debridement can be categorized as mechanical, enzymatic, autolytic, biological, and surgical. Surgical debridement is arguably the most common and varied type of debridement. A myriad of instrumentation and adjuncts are utilized to physically excise nonviable tissue from the wound bed, either at bedside, in clinic, or in an operating room. The surgeon will debride tissue to viability, as determined by tissue character and the presence of vascularity in healthy tissues, using any combination of instruments including rongeur, curette, blade, scissors, forceps, and the like. Overall, surgical debridement affords superior control over what and how much tissue is removed, is the most efficient means to achieve a clean wound bed, and can speed the healing process in nearly every patient.
A plethora of topical products exist and may be utilized in conjunction with debridement in the management of wounds in the form of pastes, ointments, gels, and solutions. These include debriding agents, antibiotics and antimicrobial formulations, as well as progranulation products. The ease of application and noninvasive nature make them a simple but effective adjunct to wound care. Commonly utilized topical antibiotics include triple antibiotic, mupirocin, gentamicin, silver sulfadiazine, and cadexomer iodine. A multitude of topical agents exist with varying indications and efficacies, however a detailed discussion of each agent is beyond the depth of this discussion.
Dressing materials represent a great diversity of function in the approach to wound healing and promote formation of granulation tissue through infection prevention, exudate control, void filling, and prevention from pressure and shear forces. An understanding of the different dressing categories and uses allows for a better patient-specific dressing selection. Use of diluted acetic acid (vinegar) solution has been shown to be effective in the treatment of multi-bacterial infected wounds including Pseudomonas infections. Additionally, use of diluted sodium hypochlorite (bleach) solution should be used for no more than three to four days consecutively due to the potential caustic effects on healthy surrounding tissues and cells involved in wound healing (i.e., fibroblasts, keratinocytes, neutrophils, endothelial cells). Absorptive wound filler dressing materials are used in exudative wounds and function by drawing fluid away from the wound surface. Topical collagens are typically combined with other materials including alginates or hydrogels and have the ability to absorb significant volumes of exudate and dissolve at the wound site.
Bioengineered skin substitute grafts play an important role in accelerating the healing of chronic or non-healing wounds, however, due to their heightened cost they require judicious utilization. It is important to note the use of bioengineered tissue substitutes alone does not replace the fundamental basics of wound management as mentioned above and should be seen only as an adjuvant to concurrent good practice therapies. Prior to application, and regardless of the specific biologic used, the wound should be free of infection and adequate tissue vascularity should be established. Living cell-based biologic skin substitute grafts deliver growth factors to wound beds and can promote the conversion of a stagnant wound to an acute wound to incite healing. Each product has been specifically designed to interact with the wound environment in a unique manner. As such, not all products are the same in terms of structure and function. Therefore, each product will have its own specifics for application, and a general protocol should be adhered to. Application should begin with thorough wound debridement to a bleeding base.
Negative pressure wound therapy (NPWT) has become ubiquitous in the treatment of both acute and chronic wounds of varying size and depth. Whether used as a supplement to primary wound closure, as a precursor to delayed closure, or for preparation of the wound bed for additional therapies, NPWT now plays an important role in all processes of wound closure. Since its inception, NPWT has been reported with successful outcomes in the medical and surgical literature and promotes granulation by decreasing bacterial bioburden and increasing capillary budding at the wound base in an assortment of wound types. Additionally, its superiority over more “standard” wound care modalities has been well established, and its variability of use via adjustable settings and formations makes it an excellent adjunct to wound treatment.
Hyperbaric oxygen therapy (HBO) has been demonstrated to be effective as an adjunctive therapy in some chronic wound management. This wound care modality should be used as a supplement in conjunction with other wound care modalities and specifically may be beneficial in patients with microvascular disease causing local wound ischemia. Regardless of the physiology of HBO, oxygenation will not reach the wound tissues if peripheral vascular occlusion exists. A careful assessment of the cost–benefit ratio should be conducted prior to use and only ever in a state-sanctioned HBO facility with properly licensed HBO specialists.
The ability to optimize the healing potential of the comorbid patient is of great importance. Numerous scenarios exist wherein the physiologic ability to heal in the lower extremity is blunted from either local or systemic factors or some combination thereof. This topic deserves a devoted discussion into the extensive causes of blunted healing potential; however, the most common etiology for retarded healing includes adverse arterial perfusion, poor glucose management, biomechanical fault, poor nutrition, underlying rheumatologic pathology, history of organ transplantation on immunosuppression, or history of cancer treatment with radiation or chemotherapy. Anecdotally, the diabetic patient population most often ascribes to underlying pathology related to peripheral arterial pathology and/or chronically poor blood glucose levels, most often with an associated biomechanical fault. It is important to recognize that these factors and many more may have a significantly adverse effect on a tissue’s ability to heal to fruition and to stay healed in the long term.
All too often a patient’s wound healing either stagnates or digresses until the insufficiency in healing potential is corrected and the physiologic healing potential is optimized. Where available, inquiry into the macro- and microvascular arterial perfusion of the angiosome to the surgical or wound site should be assessed and treated with a lower extremity arteriogram or with an open bypass where applicable. Additionally, acute and chronic blood glucose should be strictly managed to afford appropriate healing potential. When any physical findings and personal or familial history indicate the possible presence of an underlying rheumatologic pathology, a rheumatology consultation should be placed in order to ensure no underlying pathology is contributing to non- or delayed healing. Patients with any history of organ transplantation or cancer should be screened for remote or continued use of immunosuppressive agents or treatments. Finally, an assessment for associated biomechanical fault with formulation for its management can be an integral aspect of wound healing and may ultimately prevent the reformation of such pathologies.
The biomechanics of the lower extremities is an immense but integral topic of consideration, especially with respect to its implications in the complex wound and comorbid populations. Although the full extent of lower extremity biomechanics lies well outside the scope of this discussion, it does warrant special consideration and discussion. Ultimately, gait biomechanics in the complex wound patient are especially important due to the lower extremity’s relationship with the weight-bearing surface, its interaction with ground reaction forces, and perhaps most importantly in a patient’s ambulatory efforts and demands. Inherently, the foot’s contact with the ground in a static and especially in a dynamic and ambulatory manner will undergo extreme multiplanar forces that may precipitate excessive force distribution resulting in the formation of an assortment of pathologies, which may also blunt the remaining tissue’s ability to heal or cause the formation of new areas of excessive force. This is nowhere more apparent than in the plantar aspect of the foot; however, anatomic areas surrounding joints with significant excursion like the ankle, midtarsal, metatarsophalangeal and interphalangeal joints and the medial and lateral aspects of the foot are especially susceptible to these stresses as well. This process is magnified in those patients where underlying deformity exists as well as in those with peripheral neuropathy, where protective and corrective responses to ground reactive forces are blunted or grossly absent. Simplistically, biomechanical considerations of the complex wound patient population should be made in two general categories: considerations for offloading and/or immobilization and considerations for deformity correction and/or accommodation.
A basic understanding and working knowledge of normal human gait mechanics is essential in the assessment and treatment of the pathologic gait pattern and thus its impact on the healing and longevity of the wound patient. Bipedalism, that is, habitual two-legged locomotion, is truly a uniquely human ability. Anthropologic debate exists regarding the precise manner of evolution of our upright bipedal gait; however, consensus remains that this specific and persistent form of ambulation is unique to human beings but as such is fraught with the potential for pathologic disturbance. Normal human bipedal gait has been crudely, though not incorrectly, likened to a series of controlled forward falls. Our refined modern understanding of the human gait cycle is that of a reciprocating sequence of lower extremity motions which moves the body forward while simultaneously maintaining stability and conserving energy. Identification of the numerous events that occur during gait necessitates viewing from several vantage points, both literally and figuratively. As the body moves forward, one limb serves as a mobile source of support while the other limb advances itself to a new support location. Then the limbs reverse their roles. A single sequence of these actions by one limb is termed a gait cycle or stride ( Fig. 9.2.1 ). Each gait cycle is divided into two phases, stance and swing. During stance phase the foot is in contact with the ground, which accounts for approximately 60% of a limb’s gait cycle. During swing phase the foot is advancing forward in the air, not contacting the ground, and accounts for approximately 40% of a limb’s gait cycle. For the transfer of body weight from one limb to another, both feet are in contact with the ground simultaneously in opposite ends of the stance phase for a brief period termed dual limb support . The duration of these actions of gait varies indirectly with the ambulatory velocity, where as one’s gait velocity increases, the total time spent in both stance and swing phase are shortened. In order for an entire limb to afford a normal gait pattern, it must meet five prerequisites: stability during stance phase, clearance during swing phase, adequate step length, prepositioning during swing phase , and energy conservation throughout the cycle . Failure to provide at least these prerequisites will ensure a pathologic gait pattern in some variety.

Stability during the stance phase may be further defined by three distinct functional actions of the foot and ankle complex, which provide for weight acceptance, forward progression of the body, and ultimately forward propulsion or push-off. Perry defined these actions as the rockers of the stance phase of a gait cycle ( Fig. 9.2.2 ). First rocker (heel rocker) is seen immediately following initial contact of the heel as eccentric plantarflexion motion of the ankle during loading response, which accounts for significant force absorption or weight acceptance as well as for inducing forefoot contact with the ground. Second rocker (ankle rocker) is the forward progression of the leg atop of a plantigrade foot seen as ankle dorsiflexion which precipitates forward progression of the body atop the stance phase foot. Finally, third rocker (toe rocker) is observed as dorsiflexion at the level of the metatarsophalangeal joints and includes active stability of the plantarflexory force for terminal stance phase push-off of the extremity away from the ground. Deviation from these functional elements may subtly or significantly alter gait mechanics, leading to the formation of a pathologic gait pattern.
 is eccentric plantarflexion motion of the ankle during loading response. Second rocker (ankle rocker) is ankle dorsiflexion which precipitates forward progression of the body atop the stance phase foot. Third rocker (toe rocker) is dorsiflexion at the level of the metatarsophalangeal joints for terminal stance phase push-off.")
Pathologic human gait is seen under a wide array of scenarios and may range from minor or seemingly insignificant to severely incapacitating. While the list of disease states that can impair a patient’s ability to ambulate may differ markedly in their primary cause, the abnormalities they impose on the biomechanics of gait fall into four primary functional categories: deformity, weakness, control , and pain . Each of these categories has typical modes of impairment and/or compensation, and recognition of these characteristics will help to differentiate primary pathology from those that are non-contributory. Pathologic gait secondary to deformity is by-and-large the primary etiology of biomechanical fault in the complex wound population.
However, it is important to recognize that peripheral neuropathy and its associated proprioceptive impairments and relative weakness may also contribute to the formation of deformity-induced pathologic gait and its sequelae. Peripheral neuropathy will obstruct and alter ambulation as it impairs proprioceptive and nociceptive sensations of the lower extremities and alters the perceived quality of contact with the floor. As such, there is a lack of guarded weight acceptance and transfer of body momentum onto and through the stance phase limb. Peripheral neuropathy will prevent otherwise rapid autonomic stability, and this may exaggerate the already large and multiplanar forces born by the foot and ankle complex, which may be even more amplified by associated foot and ankle deformity.
Finally, but importantly, it is imperative to understand that deformity and/or weakness of the foot and ankle may not immediately or outwardly be projected as frankly pathologic gait patterns but rather, may very well manifest solely in the form of quite subtle aberrant force distributions evidenced only under careful physical examination and/or radiographically. Even still, identification of pathology including deformities of alignment and/or stability in the foot and ankle remain elusive. The human body has an amazing ability to compensate for difficulties in gait mechanics where many deformities and/or weaknesses are quite efficiently amended for during the gait cycle while at the same time preserving a relatively forward pattern of ambulation. Where one anatomic area lacks sufficient stability or alignment, another level may reactively alter its position to help compensatorily realign for continued forward body progression. A common example is seen where any functional lengthening of a single limb, as in drop foot pathology, results in a deviation of the opposite limb or the trunk in order to provide for sufficient swing phase clearance of the ground. In this way, deformity of the foot and ankle is hidden from view and may only be detected with identification of compensation and careful physical examination. Additionally, our ubiquitous use of shoe gear and clothing can easily mask the appropriate visualization of our anatomy, and these may themselves provide compensation for, or even precipitate, the formation of deformity. These innate abilities for biomechanical compensation and masking of deformity accounts for a seemingly large proportion of patients who suffer mechanically induced pathology without early recognition and thus delayed intervention and the precipitation of further disease processes.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here