Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Advances in microsurgery have broadened the scope of reconstructive solutions available for the closure of chronic lower extremity wounds. Pedicled muscle flaps and free tissue transfer offer high rates of limb salvage for patients who might otherwise be subject to minor or major limb amputation. Diabetes is not an absolute contraindication for skin grafting, local muscle flaps, or free flap reconstruction, but patients with diabetes often require longer healing times.
The decision to pursue soft-tissue reconstruction over amputation requires careful consideration of a number of patient- and wound-specific factors including but not limited to wound size and location, exposure of underlying bony, ligamentous, or tendinous structures, and vascular supply. The multifaceted nature of surgical planning for the highly comorbid chronic wound population, including patients with diabetic foot wounds, requires a multidisciplinary team of specialists including reconstructive, vascular, orthopedic, and podiatric surgeons in addition to infectious disease, endocrinology, and hematology physicians.
The purpose of this chapter is to discuss available soft-tissue reconstructive modalities, factors that should be considered when choosing an optimal reconstructive strategy, and preoperative evaluation to maximize success in free tissue transfer reconstruction.
The reconstructive ladder , which was first described by Mathes and Nahai in 1982, has traditionally provided a framework for the stepwise progression through management options for complex wounds. The ladder begins with healing by secondary intention and progresses through local wound care and skin grafts before more complex solutions such as local and free flaps. Subsequent iterations of the ladder incorporated negative pressure wound therapy and dermal matrices as reconstructive options in the middle rungs of the ladder.
Others opt for a more flexible framework, such as the reconstructive elevator , which allows a surgeon to rise directly to the most effective reconstructive modality without first going through earlier steps in the ladder. This approach is especially useful in cases where lower rungs of the ladder are not likely to be successful. This is particularly relevant in patients with diabetes who develop chronic wounds on areas of the lower extremity with thin soft-tissue cover, namely the medial surface of the tibia and/or the lower third of the lateral surface of the fibula. Loss of overlying skin in these areas results in exposed bone. Inadequate soft-tissue domain and exposed bony and/or tendinous structures preclude the use of primary closure and skin grafting, respectively. Furthermore, chronic wounds on weight-bearing surfaces are subject to biomechanical stress and should therefore not be treated with primary closure or skin grafting. Even more complex options towards the top of the ladder may be insufficient for some wounds: local flaps have limited reach and may not always offer a reliable reconstructive option, especially in distal third defects that have been subject to repetitive trauma.
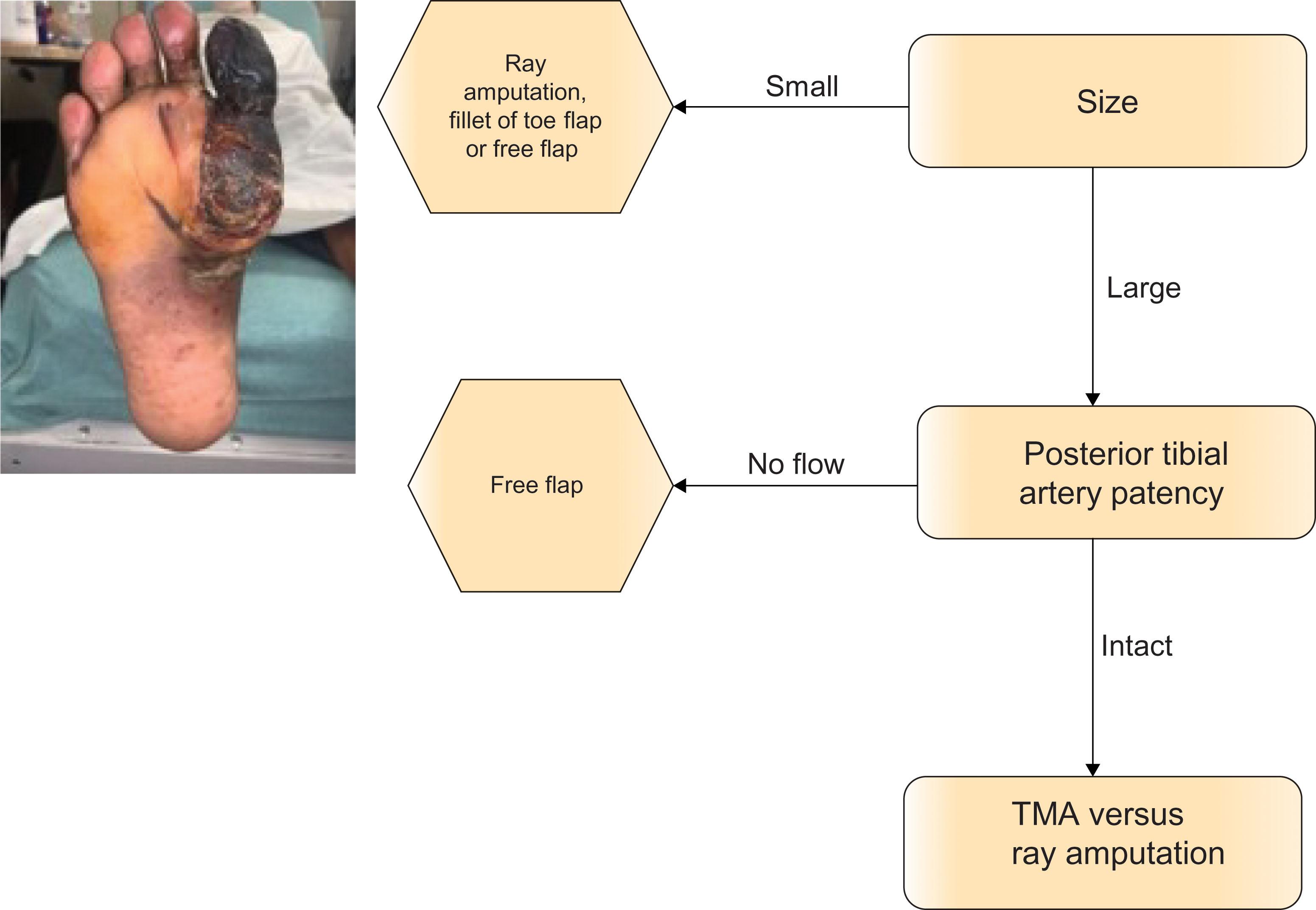
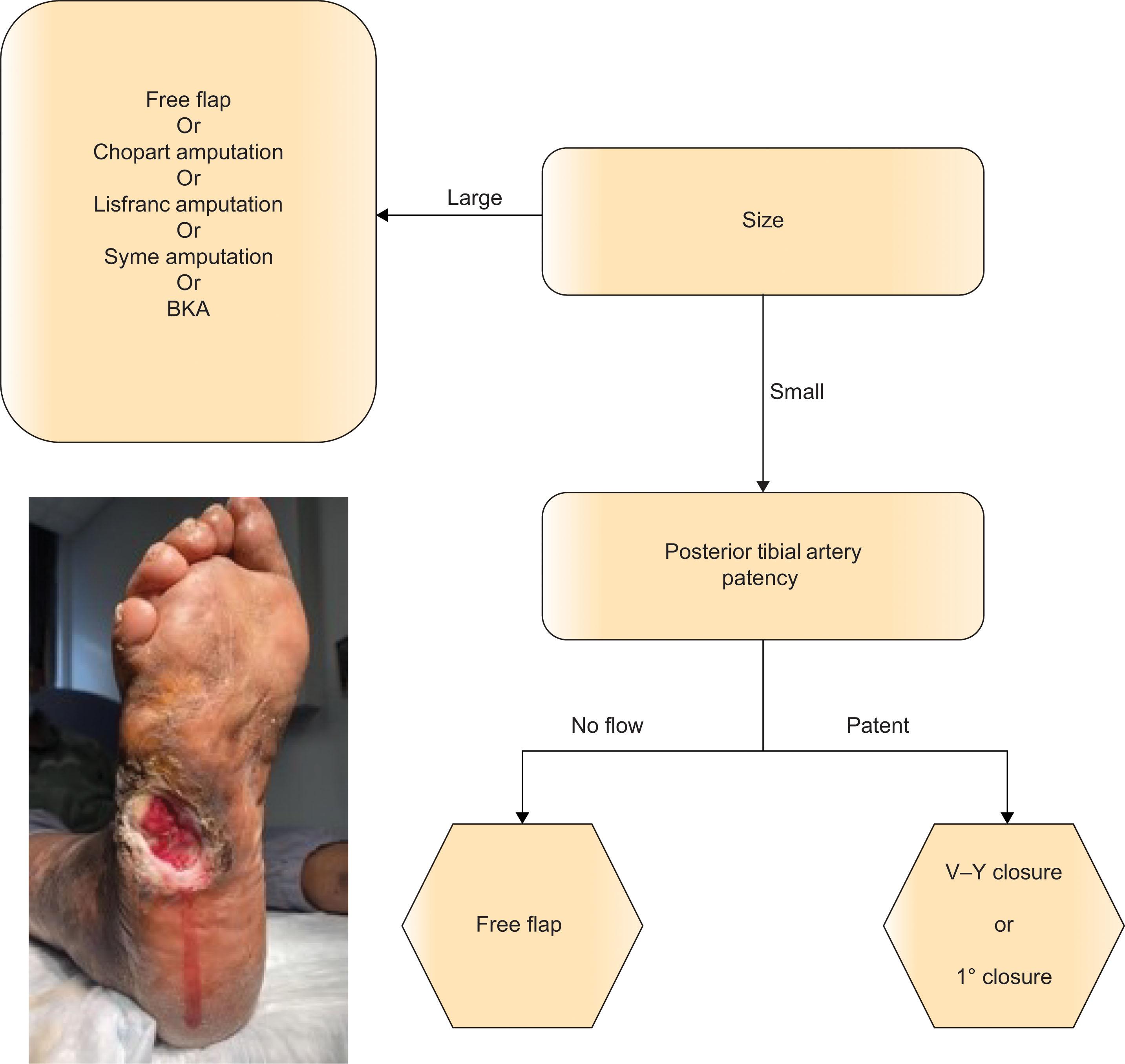
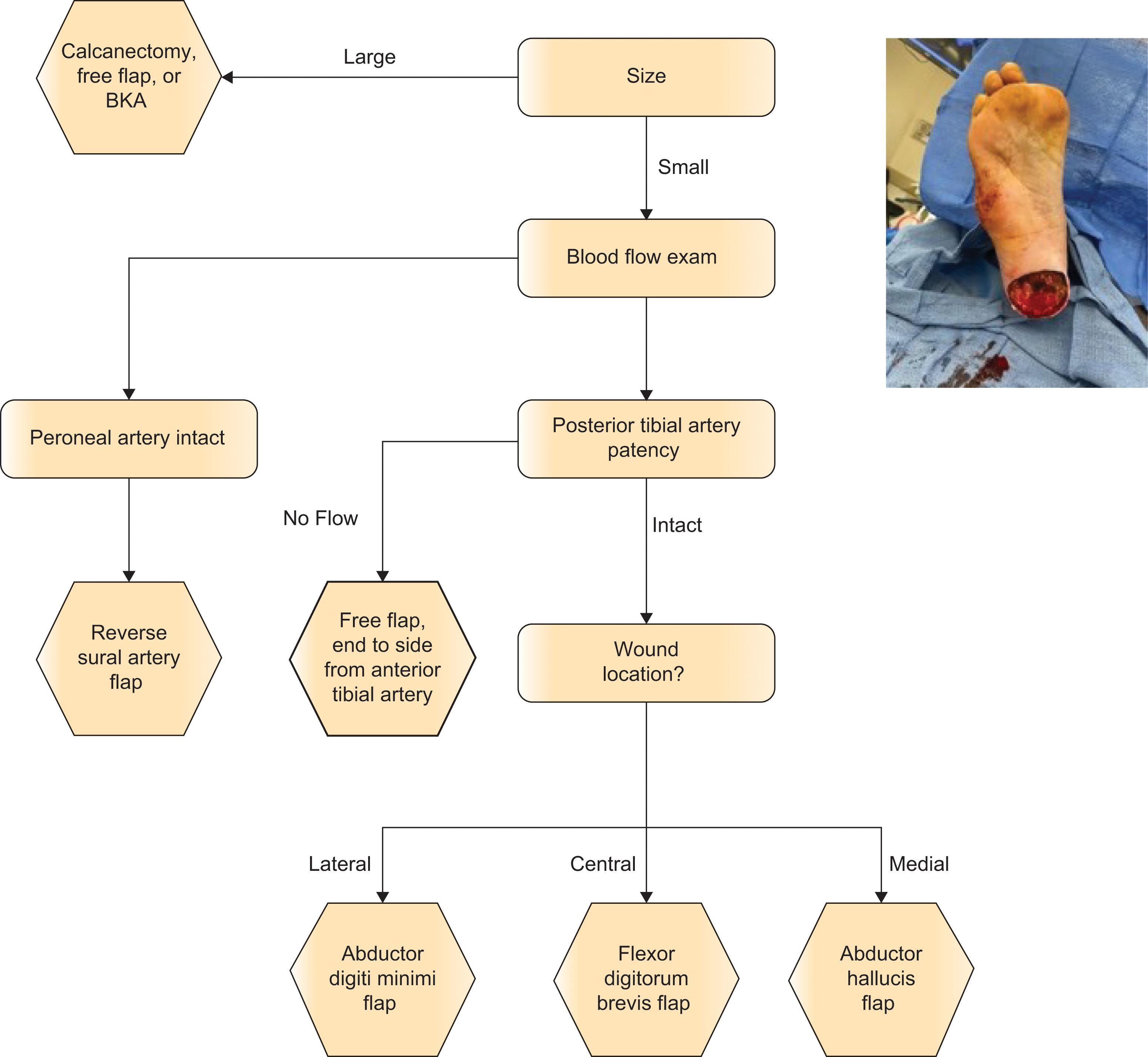
Reconstructive planning for a diabetic foot wound requires consideration of a multitude of patient- and wound-specific factors, including (1) size of wound, (2) location of wound, (3) exposed underlying structures, and in the case of possible free flap, (4) patency of possible donor and recipient vessels. Algorithms 9.3.1–9.3.3 provide a detailed framework for reconstructive modalities, organized by wound location (forefoot, midfoot, and hindfoot, respectively). In the following sections, we highlight several considerations for three reconstructive modalities: skin grafting, local muscle flaps, and free tissue transfer.
Skin grafting is a reliable coverage option for superficial wounds on the foot and ankle. Alternative reconstructive methods such as local or free flaps should be pursued for wounds with exposed bone or tendon. Skin grafts are often avoided on weight-bearing surfaces due to concerns regarding graft healing and durability. Indeed, wounds on the plantar surface of the foot pose unique challenges to healing including but not limited to factors of blood flow and offloading. Findings of several studies have demonstrated lower healing rates for plantar wounds versus non-plantar wounds treated with split-thickness skin graft (STSG). Despite this, we have found low and comparable wound recurrence rates for STSG applied to plantar versus non-plantar foot wounds (17% versus 10%, p = 0.17) at our institution. Another study investigating STSG application for coverage of 20 plantar surface burn wounds found that only one patient required resurfacing, and all patients eventually returned to ambulation over the course of a 2–8 year follow-up. These findings suggest that STSG may provide a durable, cost-effective coverage option for patients who are able to heal.
While tight glycemic control in the perioperative period can reduce the risk of wound dehiscence and/or reoperation, poorly controlled diabetes is not an absolute contraindication to skin grafting. A retrospective review of patients with diabetes who underwent STSG application to the lower extremity found that there was no significant difference in hemoglobin A1c between patients who had >90% graft take versus those whose skin graft failed (healed 8.7% ± 2.8% versus failed 8.4% ± 3.1%, p = 0.72). While successful wound coverage in the diabetic population can be achieved with STSG, it should be noted that patients with diabetes typically take longer to heal after STSG when compared to patients without diabetes. The literature cites average healing times ranging from 5 to 17 weeks for patients with diabetes who undergo STSG. In contrast, research on STSG in patients without diabetes demonstrates healing times of 2 to 4 weeks.
Prior to coverage with a skin graft, the recipient wound bed should undergo serial debridements in order to eradicate infected or necrotic tissue as well as biofilm. Pre- and post-debridement cultures should be taken in order to guide tailored antibiotic therapy for each patient. Scant or negative growth should be confirmed on cultures before proceeding with skin grafting. Harvesting of the skin graft begins by injecting the donor site with a tumescent solution to achieve adequate pain control, hemostasis, and a firm surface for graft harvest. At our institution, we use a tumescent solution comprising one liter of lactated Ringer’s, one ampule of epinephrine, and 30 cc of 1% lidocaine plain. We use a large spinal needle to inject the solution into the subcutaneous tissue. The donor site should then be wiped clean of any skin preparation solution and generously lathered with a lubricant such as mineral oil to facilitate smooth gliding of the dermatome across the skin surface. For coverage of wounds on the lower third of the leg, we typically harvest skin grafts using a power dermatome on the anterolateral thigh of the ipsi- or contralateral leg. Intermediate-thickness grafts ranging from 0.012 to 0.018 inches are suitable for coverage of diabetic foot wounds. Grafts are then meshed in a 1.5:1 or 3:1 ratio using a hand-powered meshing device and attached to the wound surface.
Local muscle flaps were pioneered by Ger in the late 1960s and were used to reconstruct defects of the foot and ankle until the late 1970s, when advances in microsurgery brought free flap reconstruction to the forefront as a preferred reconstructive modality in many cases. In general, flap coverage (either free or local) is the reconstructive modality of choice in defects with exposed tendon, joints, or bone. Local muscle flaps should be used for coverage of small defects (3 × 6 cm or less) that are within reach of a local flap and have exposed bone, joint, or tendon. Local flaps comprising well-vascularized muscle can improve blood flow in the vicinity of the defect and can also provide a hospitable surface for subsequent skin grafting. Dissection of intrinsic muscle flaps is relatively fast and easy and results in minimal functional and aesthetic donor site morbidity. Disadvantages of local muscle flaps include limited bulk and reach; therefore, preoperative planning should ensure that the rotated muscle will have sufficient reach to adequately cover the defect. The bulk offered by a muscle flap is most accurately assessed visually and is therefore difficult to predict preoperatively. A muscle flap must cover any exposed joint, tendon, or bone, but need not fill the entire defect. Skin grafts or biologic wound matrices can be used to cover any unfilled granulating tissue as well as the muscle graft.
Importantly, diabetes is not a contraindication to local tissue transfer. At our institution, limb salvage and healing rates after local tissue transfer were comparable between patients with diabetes and trauma patients. It is of note, however, that these same studies showed that patients with diabetes undergoing local pedicled flaps had longer healing times, hospital length of stays, and lower long-term survival when compared to trauma patients.
At our institution, we primarily rely on three intrinsic muscles of the foot for coverage of diabetic foot wounds: (1) abductor hallucis (AH), (2) abductor digit minimi (ADM), and (3) flexor digitorum brevis (FDB). The incisions required to harvest each of these flaps runs along the border of neighboring angiosomes. Because of this, the soft tissue on either side of the donor site incision should be well-vascularized, allowing the wound edges at the donor site to heal well. The AH, ADM, and FDB flaps are all classified as Mathes and Nahai type II flaps as they each contain one dominant pedicle and one or more distant minor pedicles.
The abductor hallucis (AH) can be used for coverage of wounds on the medial midfoot, ankle, and heel. Coverage of large midfoot and plantar heel wounds can be achieved by combining the AH flap with an ADH flap. The abductor digiti minimi (ADM) can be used for coverage of lateral ankle and calcaneal wounds. The flexor digitorum brevis (FDB) can be used for coverage of wounds on the plantar heel.
Because of the aforementioned limitations of traditionally “simple” reconstructive modalities (i.e., primary closure, skin grafting, etc.) and continued advances in microsurgery, free tissue transfer is no longer viewed as a last resort but rather as a highly reliable reconstructive solution. Free flap reconstruction has been shown to have high rates of reconstructive success and postoperative ambulation and is also associated with improved morbidity and mortality relative to amputation.
Specific indications for free tissue transfer reconstruction include wounds that: (1) are large (>2–3 cm), (2) involve both bone and muscle loss, (3) have exposed joint or neurovascular structures and/or (4) are located in ischemic angiosomes. It may seem contradictory that free tissue transfer should be considered for defects on areas of the leg or foot that are in ischemic angiosomes; however, without in-line blood flow to the wounded area, local options are likely to be unsuccessful. In these settings, FTT acts as a vascular bypass and can add vascularized tissue to otherwise ischemic territories.
Importantly, diabetes, peripheral vascular disease, and elderly age are not absolute contraindications for free tissue transfer; however, patients with these comorbidities do require unique preoperative considerations (see section entitled “Preoperative evaluation and optimization for free flap reconstruction”). Furthermore, patients with diabetes who undergo free tissue transfer reconstruction have been shown to require more debridements, longer healing times, and decreased long-term survival relative to patients without diabetes who undergo free tissue transfer.
There are, however, several contraindications to free tissue transfer which must be given careful consideration in patients with diabetes. First, free tissue transfer is contraindicated in patients without a suitable recipient vessel. This is a particularly important consideration in the diabetic population as peripheral vascular disease is commonly encountered in these patients. Second, caution should be taken in patients with end-stage renal disease and/or patients on dialysis. Patients with end-stage renal disease often have compromised wound healing and diffuse vessel calcifications, the latter of which can complicate micro-anastomosis. Patients on dialysis are at increased risk of hematoma formation as well as thromboembolic complications.
Once a patient is deemed suitable for reconstruction with free tissue transfer, three main considerations should serve as a guide for choosing the optimal free flap for a given lower extremity defect: (1) flap composition, (2) functional and aesthetic needs, and (3) donor site morbidity.
One of four flap compositions can be utilized for most reconstructions of the lower extremity: fasciocutaneous, muscle only, musculocutaneous, or chimeric.
Fasciocutaneous flaps are harvested by elevating the skin along with its underlying deep fascia. Fasciocutaneous flaps are thin, pliable, and amenable to tissue expansion. While preservation of the underlying muscle reduces the donor site morbidity of this flap type, large (>8 cm) fasciocutaneous flaps may require skin grafts at the donor site.
In cases where subcutaneous tissue is too thick, we typically rely instead on a flap comprising only muscle followed by overlying skin grafts. It is of note that any flap requiring an overlying skin graft may require debridement and subsequent repeat skin grafts in the setting of partial skin graft loss. This is a particularly important consideration in the vasculopathic population as these patients often have compromised blood supply to the overlying graft.
Musculocutaneous flaps are harvested by elevating the skin and underlying muscle. The muscle component of these flaps makes them well-vascularized and bulkier than fasciocutaneous flaps. As a result, musculocutaneous flaps are more resistant to infection and are particularly useful for coverage of defects that require obliteration of dead space.
As their name implies, chimeric flaps comprise several different tissue types and can be particularly useful for reconstruction of defects with tendinous or bony components. Chimeric flaps can include vascularized bone, for example, which can be helpful for reconstruction of defects with bony involvement. Chimeric flaps can also be used for cases requiring tendinous reconstruction: in our institution we often use chimeric anterolateral thigh (ALT) with rolled fascia lata free flaps in these instances.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here