Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

A two-position circumferential approach for body contouring of the lower trunk is presented as an alternative technique to the belt lipectomy described by Aly.
Mostly indicated in patients after massive weight loss, this procedure arose from the original lower bodylift from Ted Lockwood.
It allows the simultaneous skin resection and reshaping in the abdominal, flank, lateral thigh, back, and gluteal regions in the same operation with only two position changes.
Besides the reconstruction of the abdominal wall, the gluteal restoration presents a major aspect of this procedure, allowing a volume and shape enhancement with autologous tissue transpositioning.
This technique requires precise patient selection, discussion of the desired result with the patient and clarification of realistic expectations.
The lipo-bodylift is the ideal procedure for skin laxity around the trunk after weight loss, aging, or liposuction-induced deformities.
Focus more on the gluteal area and add gluteal reconstruction to the technique.
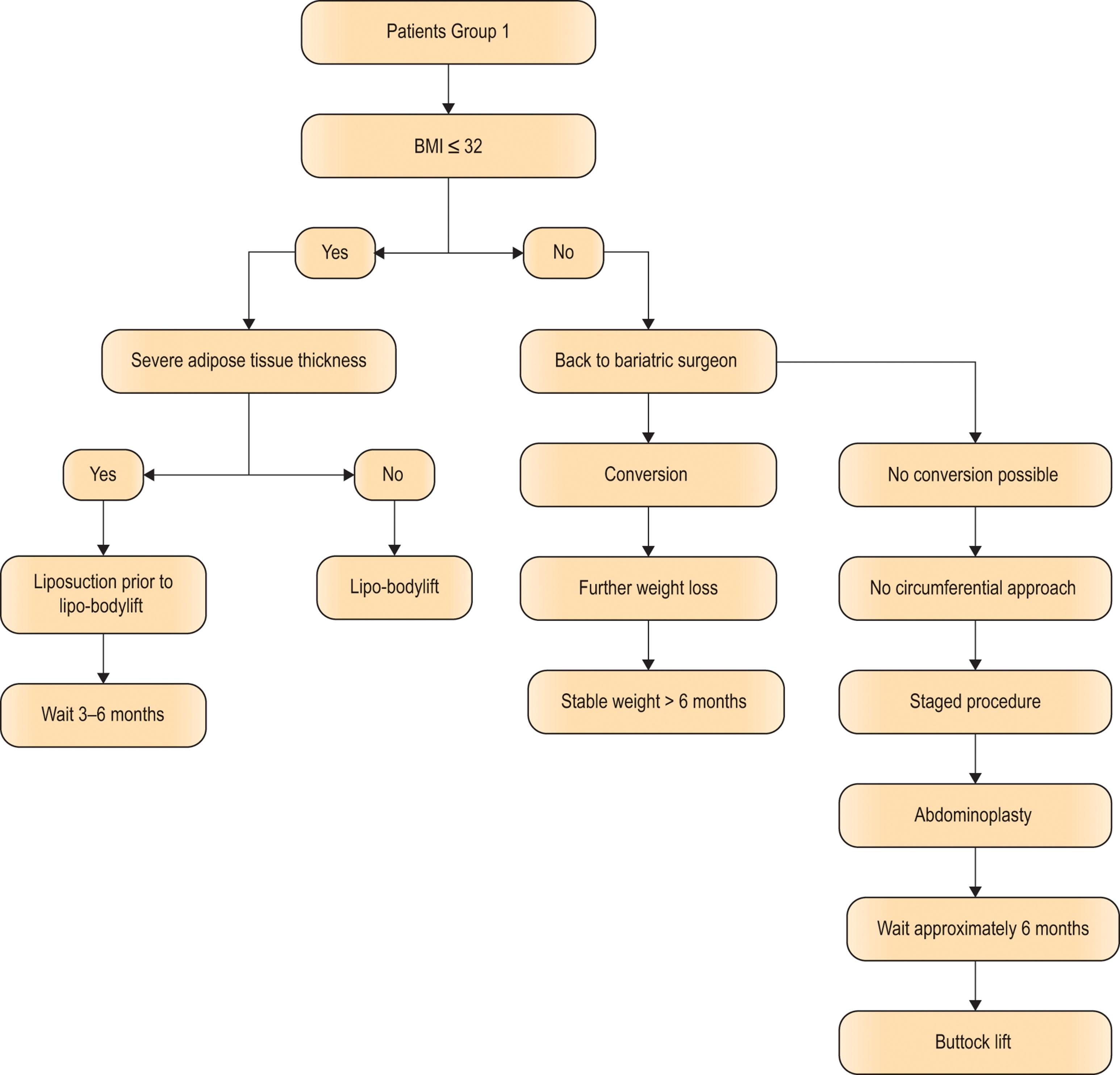
Do NOT perform a bodylift procedure on patients with body mass index >32.
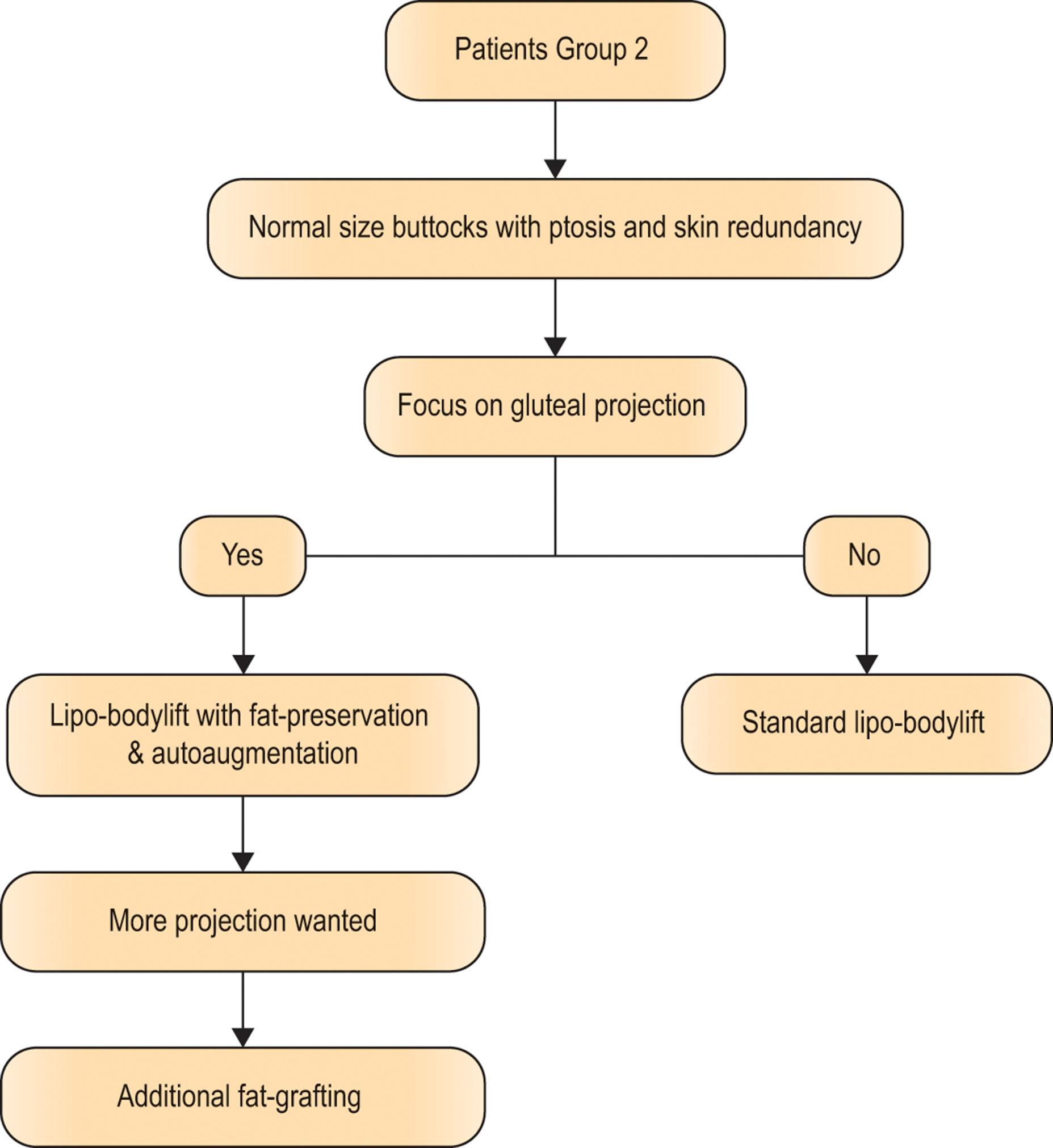
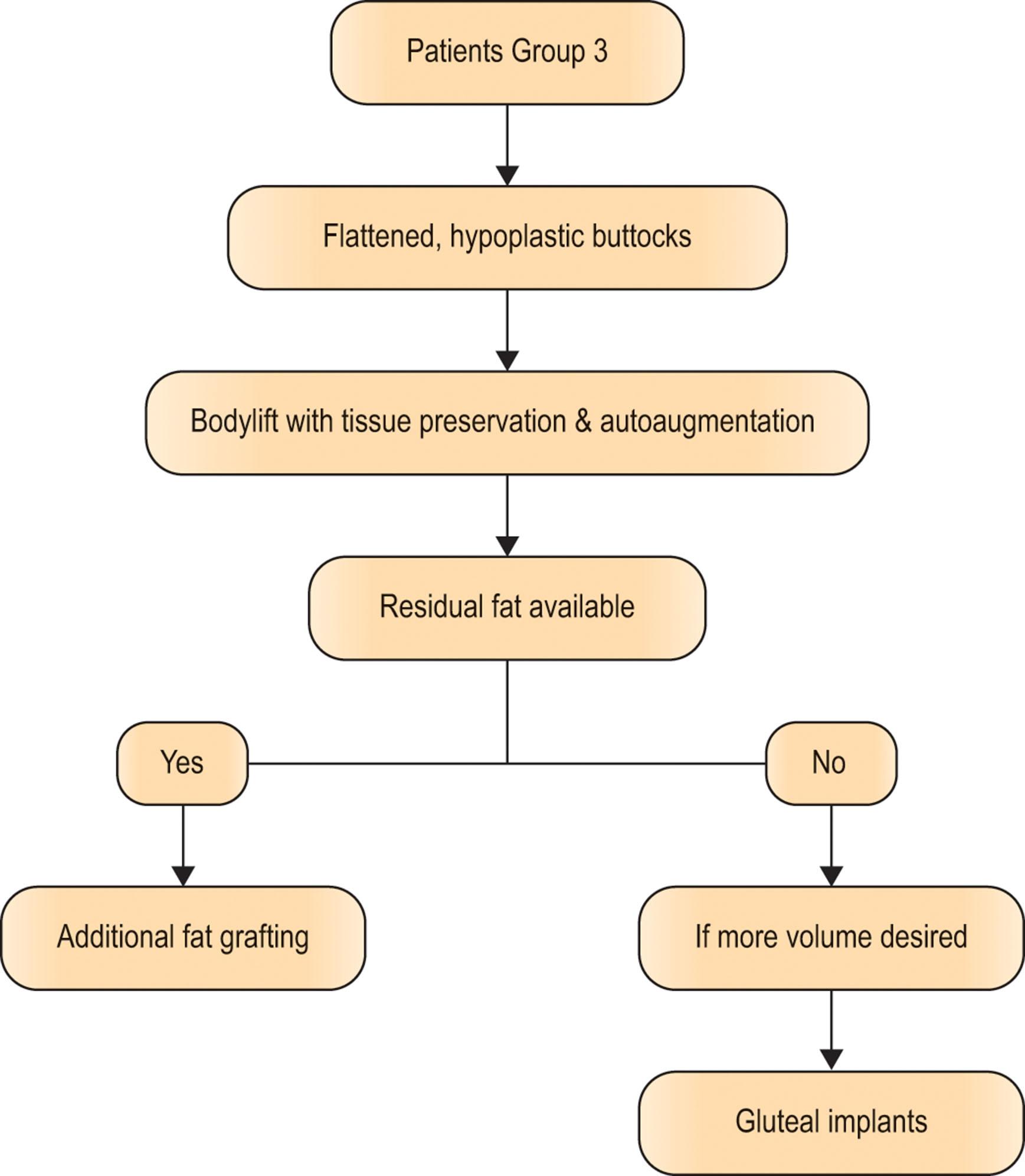
Divide weight loss patients into three groups: large buttocks with excess adipose tissue; normal-sized buttocks with ptosis and skin redundancy; flattened, hypoplastic buttocks with ptosis and skin redundancy.
Access video lecture content for this chapter online at Elsevier eBooks+ 
With the success and increasing number of bariatric procedures, the authors have registered a yearly increase of body contouring procedures. Additionally, due to increasing experience in this field of plastic surgery, these procedures have a wider range of indications, including patients after massive weight loss, patients with primarily cosmetic indications (aging process), and patients who seek for correction of contour deformities after previous liposuction. Coincidently, the requirements and demands for such operations are continually increasing. In addition to the typical problem areas such as the abdomen, the mons pubis, and hip regions, patients frequently present with a growing attention to the aesthetic restoration of the gluteal area.
The variety of gluteal deformities after weight loss result in a range of patient complaints and discomfort. Some patients complain of an enlarged buttock, some of deficient gluteal volume with gluteal flattening (platypygia), and yet others suffer from cellulite or a lengthening of the infragluteal fold. However, patients primarily seek for an enhancement of the gluteal shape and projection. According to the statistics of the International Society of Aesthetic Plastic Surgery (ISAPS), this is the current fastest growing field.
A well-shaped buttock is characterized by several factors: it is more rounded than angular, the intergluteal fold is rather short than long, and the feminine gluteal cleavage has a superior and inferior buttock separation. Dividing the buttocks into an upper, middle, and lower section, the ideal maximum projection should be between the upper and middle third.
The infragluteal fold should run in a round rather than horizontal curve with a minimal crease, ideally without any droop. Patients' side view should illustrate an S-shaped contour in relation to the back and thigh, as a smooth inward sweep of the inferior back and waist area. To meet these ideal characteristics, several techniques are available to plastic surgeons. In the late 1960s, surgeons performed gluteal augmentation with existing breast implants. Currently, various gluteal implants are available, which can be implanted epifascially, subfascially, or submuscularly. Nowadays, gluteal contouring is most frequently performed through liposuction, particularly by sculpturing the adjoining regions such as the hips, flanks, and saddlebag deformities, achieving excellent results without any direct buttock approach.
During the past decade, buttock augmentation by autologous fat grafting has gained wider acceptance and success. Many different techniques such as macro- or micrografting are available for contour improvement of the gluteal region, solely or in combination with liposculpturing.
These techniques, however, are not always suitable for patients after massive weight loss (MWL). These specific patients suffer from atonic skin quality with a high degree of laxity and, consequently, with the indisputable requirement of tissue resection. These severe deformities have caused a continuous development of various lifting procedures, such as the pioneering circumferential lower bodylift, described by Ted Lockwood in 1993. Further developments of these procedures in combination with autologous tissue augmentation, such as the de-epithelialized gluteal flaps for buttock reshaping, enable an improvement of the postoperative results. In 2005, Sozer et al . reported on a series of 20 de-epithelialized turnover dermal fat flaps for buttock augmentation in bariatric and aesthetic patients undergoing lower bodylifts. After more than 200 cases, the technique has evolved to include a split portion of the gluteus maximus muscle, resulting in a better blood supply to the flap, more caudal reach, and dramatic decrease in fatty necrosis.
In this context, we established a technique of gluteal fat tissue transpositioning (transposition-gluteoplasty) during our modification of the lower lipo-bodylift, which has shown itself to be a reliable alternative for enhancement of the gluteal projection and shape.
A precise physical examination and assessment of patients' medical history during the first consultation is mandatory in every patient. We recommend a repeat of evaluation prior to surgery, if it is performed with a delay from the time of the first consultation. The assessment of medical history includes the current weight; initial and current body mass index (BMI) or in future the body shape index (BSI; a metric for assessing the health implications of a given human body height, mass, and waist circumference – the inclusion of the latter is believed to make the BSI a better indicator of the health risks from excess weight than the standard BMI). Formula: BSI (kg/m 2 ) = Waistline (m) ÷ (BMI (kg/m 2 ) {2/3} × Height (m) {1/2} ); the weight history, with weight fluctuations and constancy periods; the frequency of exercising; former bariatric procedures; nutritional disorders; medication; the number of pregnancies and children; history of Cesarean section; abdominal surgeries and abdominal hernias; gastrointestinal, cardiac, and pulmonary history; and a smoking history. It is important to know which bariatric procedure has been used. Look for the port, if a gastric banding was performed, that may be in your area of undermining or liposuction. Traction on your flap may result in a dislocation of the band causing strangulation of the stomach. Some anesthesiologists prefer to have the band deflated. Watch out for a proper supplement of vitamin B 12 in patients after bypass and sleeve resection.
The routine blood tests after bariatric surgery are hemoglobin, hematocrit, electrolytes, vitamin B 1 , B 12 , folic acid, iron/ferritin, vitamin D 3 , glucose, transaminases, and albumin. Total protein, total cholesterol, parathyroid hormone, A1C (the latter only if patient was diabetic before surgery).
The recommended annual lab work for post-bariatric patients:
Vitamin A
Vitamin B 6
Vitamin B 12
Vitamin E
Vitamin D (25-hydroxyvitamin D)
Copper
Calcium
Magnesium
Phosphorous
Zinc
Folate
Prealbumin/total protein/albumin
Iron/total iron-binding capacity (TIBC), ferritin, transferrin
CBC (complete blood count), hemoglobin and hematocrit
Chem. 7 (comprehensive metabolic panel)
Liver panel: serum glutamic-oxaloacetic transaminase (SGOT)/serum glutamic-pyruvic transaminase (SGPT), alkaline phosphatase, T/D bilirubin
Cholesterol/triglyceride levels
Hemoglobin A1C level (only if patient was diabetic before surgery)
Dehydroepiandrosterone (DHEA)
Thyroid-stimulating hormone, T 4 (required if patient has thyroid disease)
PTH.
Previous liposuction in the abdominal area has to be ascertained and specifically enquired about since the patient might conceal this prior treatment. Patients have to present a stable weight for at least 6–12 months preoperatively; weight loss should be completed prior to the surgery. As a guideline, we do not operate on patients with a BMI above 32. This is because local and general complications are at increased risk and aesthetic outcomes disappointing. Those patients are referred back to the bariatric surgeon to decide whether there is an option of conversion.
The clinical examination is the essential part of every medical history assessment. The examination of the lower trunk should include an accurate palpation of the abdominal, lateral thigh, and gluteal adipose tissue in patients upright, prone, and supine, as well as lateral position. This enables the examiner to assess the tissue conditions with regard to volume and mobility by pinching and metric measurement. It is crucial to consider the existent adipose tissue at the lateral and posterior lower gluteal and proximal thigh region. Unfortunately, untreated distinct masses of local adipose tissue in these regions will assuredly limit the gluteal improvements, since downward traction will displace gluteal tissue in a caudal direction. Skin quality with the presence of striae has to be evaluated, explaining to the patient that supraumbilical striae will not be resected in abdominoplasty procedures (except for fleur-de-lis procedures). Further, any existing lower and upper abdominal pannus has to be assessed and measured, documenting any existing eczema or consequent hyperpigmentation. Any pre-existing scar (subcostal, midline, horizontal) in the abdominal and gluteal area has to be documented in writing and photographically, since it can impair the blood supply of the tissue flap. Further, the status of the abdominal muscles has to be assessed, and any existing rectus diastasis, incisional, epigastric, or umbilical hernia has to be excluded, in specific cases by a supportive computed tomogram or magnetic resonance imaging. In cases of elevated intra-abdominal pressure, the abdominal wall extends above the costal margin and the level of the iliac crest in the supine position. Abdominoplasty procedures with fascial tightening have to be performed cautiously in such cases and are prone to a higher recurrence rate.
We recommend setting up a photographic documentation of pre- and postoperative conditions, consisting of different views (anterior, oblique, lateral, and posterior; Fig. 32.1 ).

Postoperative photo documentation can be made at 3, 9, and 12 months. In individual cases, we recommend performing additional photo documentation of various arm and thigh positions, tissue characteristics with relaxed and contracted muscles, the patient in sitting position to demonstrate redundant upper abdominal laxity and tissue excess, and additional views with the patient holding up and pinching excess tissue in the specific region. For a classification of the different deformities, we found the Pittsburgh Rating Scale to be helpful for patient demonstration and selection of the optimal operative approach. However, we experienced a wider indication for the combined technique of liposuction and excisional procedures in all body regions.
Patients' detailed information on the operative procedure; alternative techniques; and the general and operation-related risks and benefits is an essential part of preoperative documentation. Besides standard and individualized consent forms, which have to be reviewed and signed by the patient at the earliest opportunity, we recommend an audiovisual demonstration of intraoperative details, pre- and postoperative results, and possible complications. Patients should be informed about their postoperative care including their expected level of activity, and they have to understand the limitations of the surgical result in cases of existing variables of bone structure, fat distribution, and any existing scars.
Studies have evaluated differences in collagen and elastin content in the abdominal skin of patients without weight loss compared with those with bariatric weight loss, showing an impairment in skin quality in the bariatric group. This fact should be clarified to every single patient to limit their postoperative expectations. Patients with multiple striae have to be informed that secondary relaxation in their specific case may require a repetitive skin-tightening procedure. This has to be addressed also to the health insurance for coverage or discussed with the patient.
During clinical examination of the abdominal region, the following parameters should be noted:
Abdominal tissue excess
Abdominal skin quality (striae?)
Umbilical stalk deformity
Number of skin folds and their continuity to the flanks
Skin quality
Adipose tissue volume and mobility
Abdominal muscle tone
Mons pubis region.
During clinical examination of the gluteal region, the following parameters should be noted:
Gluteal height
Gluteal width
Maximum height of projection
Round shape versus rectangular shape
Skin quality
Adipose tissue volume and mobility
Gluteal muscle tone
Back folds
Vertebral status, e.g., scoliosis.
In our MWL patient group, we have established a classification for surgical planning of the gluteal region, which can be simply divided into three groups ( Fig. 32.2 , Algorithms 32.1–32.3 ):
Large buttocks with excess amount of gluteal adipose tissue
Normal-sized buttocks with ptosis and skin redundancy
Flattened, hypoplastic buttocks with ptosis and skin redundancy.
 , group 2 (B) , and group 3 (C) gluteal deformity showing the three different types of gluteal shape.")
The adipose tissue in the upper third of the gluteal region has an excess lobular and lamellar structure with a ratio of 1:2 in females and 1:1 in males, respectively, whereas the lower third presents a 1:1 ratio in both sexes ( Fig. 32.3 ).

Patients who are in group 1 may present with residual overweight. In order to reduce gluteal adipose tissue, a thorough liposuction is performed between lobular and lamellar adipose tissue and in all areas that are going to be resected. As this will also be done in the front, we call this procedure lipo-bodylift.
In patients with a group 2 deformity, we maintain an epifascial preparation with preservation of the entire superficial fascia. In this regard, we refrain from an extensive adipose tissue resection, maintaining the lobular adipose tissue. In cases of deflated and flattened buttocks of group 3 deformities, we stringently refrain from any adipose tissue reduction and perform preparation at a superficial subcutaneous level. In opposition to the technique of subfascial dissection described by Lockwood, we generally remain above the superficial fascia, which is a constant and strong structure, separating the lamellar and lobular adipose tissue. The gluteal superficial fascia provides comparable features such as the fascial superficial musculo-aponeurotic system (SMAS) during facelift surgery, e.g., the reduction of tension on skin level and the opportunity to provide a multivectoral remodeling on different tissue levels.
Circumferential tightening procedures have the goal of restoring and improving the body shape, including the abdominal, flank, and gluteal regions. The abdominal region can be reshaped through preparatory steps deriving from a standard abdominoplasty, a lipoabdominoplasty, or fleur-de-lis abdominoplasty. The main goals are maximal skin and fat tissue reduction with contouring of the abdominal wall. The flanks are mainly restored by vertical tissue resection; additionally in fleur-de-lis procedures, the waist circumference may be reduced by horizontal tissue resection. In the gluteal region, there are different approaches available, depending on the patient’s preoperative conditions. The available options are gluteal tissue reduction by direct excision or gluteal autoaugmentation in cases of volume and shape deficiency. In both cases, the goal of the bodylift procedure is a restoration of gluteal volume and gluteal reshaping in relation to the surrounding regions.
Smokers are advised to quit smoking at least 6 weeks prior to the surgery. Patients should take antiseptic showers in the evening and morning prior to the surgery; the skin folds and the umbilicus should be cleaned thoroughly with antiseptic solutions.
Since postoperative blood transfusion may be necessary in selected cases, patients have to be informed preoperatively, as this requires a blood typing and additional informed consent. Anticoagulant drugs and supplements must be avoided 14 days prior to surgery. In all cases, we advise patients for bowel purgation the night before surgery. In patients with a large hernia, they may be restricted to a fluid diet for 24 h prior to surgery.
Patients have to be informed about the intraoperative procedures including any change of position with the risks of postoperative complications, antithrombotic precautions, Foley catheter, drains and garment placement, as well as patient-controlled analgesia. Moreover, they have to be instructed about the postoperative course regarding thromboembolism prevention, respiratory exercises, early mobilization, avoidance of high abdominal pressure, the estimated time point for drain and suture removal, as well as the minimum time required off work and away from exercise.
Patients should avoid any skin irritation or inflammation in the area of the abdominal fold and umbilicus. An inspection of these areas during consultation as well as immediately prior to the operation is strongly advisable. Prophylaxis for pulmonary embolism and deep vein thrombosis is an essential consideration, especially in smokers and patients taking birth control medications or hormone replacement therapy. We initialize heparin therapy in all patients the evening before surgery or at latest 2 h prior to the surgical procedure, Fragmin 5000 I.U. SC 1× day. We inform patients that this specific risk will be decreased if hormonal therapy is discontinued 3–4 weeks prior to surgery.
In cases of a pre-existing diastasis or hernia, the reconstruction of the fascia results in an additional increase of intra-abdominal pressure, which may be a source of respiratory difficulties. Therefore, we advise preoperative breathing exercises (utilizing an incentive spirometer) and the wearing of a compression girdle beginning 1–2 weeks prior to the surgery. A cold, dry cough, or any kind of respiratory infection, should lead to postponement of surgery, since fits of coughing may provoke a rupture of the fascial sutures with consequent secondary bleeding.
We recommend starting the markings in a standing position ( Fig. 32.4 ). The patient should be asked to bring their favorite underwear so the borders can be marked and the future scar line can be adjusted to the patient's favored underwear. This means, ideally, that the future scar can be hidden. As the next step, the tissue should be pinched out to get an estimation of the mobility and quality of the excess tissue. The future scar line should be marked in red to get a better idea of where to plan the upper incision line.

It is very important to discuss with the patient their desired result and preferences. The main aim of the lower bodylift is that the scar can be completely hidden by underwear. This approach is different from the belt lipectomy, where the main goal is to achieve the best possible waistline.
After marking the future scar line in red, we start the markings on the back with the very top of the intergluteal fold. Then the excess tissue should be pulled down at the midaxillary line to estimate the laxity from cranial of the future scar line, so that, at the end of the surgery, the scar will end up within the borders of the underwear.
In most patients, the laxity from above the scar line is about 3–4 finger-breadths. This point should be marked symmetrically on both sides.
Now the point on top of the intergluteal fold is connected with the point in the midaxillary line following the natural contour in an arcuate manner. In such a manner, the upper back incision line is finalized.
As a next step, the lower incision line is marked. The excess skin should be pinched by pulling the tissue upwards at the level of the midaxillary line while stabilizing the upper incision line with the index finger. Quite commonly, this point of the lower incision line relates to the lateral zones of adherence.
Depending on the type of deformity of the buttock, the excess tissue is pinched again and either a curved or straight line is drawn from the midaxillary line back to the intergluteal fold. If gluteal augmentation is required – such as in deflated buttocks – the lower incision line should be drawn a little more cranially, since more tissue will be required to cover the augmented area. Over-resection of skin should be strictly avoided.
In the area of the rima ani , the incision line should end in a pointed angle, because a straight incision line across the intergluteal fold leads to an elongated intergluteal fold and an enlarged buttock.
Now the front markings can be started. Most commonly in MWL patients, an additional relaxation of the mons pubis is found and should be included in the surgical plan.
First, the patient should be asked to lift up the excess tissue of the abdomen so the vulva commissure or the root of the penis is exposed. Then a distance of 7–8 cm is measured and marked cranially from the vulva commissure/root of the penis. This is the lower border of your incision line.
Now the line can be drawn laterally connecting the ventral with the dorsal markings. The ventral incision line should be planned a little bit below the natural tissue fold, since the tissue quality within the folds is normally quite low. To make sure that the angle of the incision is correct, make the patient sit and double-check that your markings on the abdomen relate to the natural folds.
To estimate the upper incision line, the patient should lay down and bend the hips in about a 45° angle. After that, the excess tissue is pinched and the upper incision line is marked above the umbilicus if it allows a tension-free closure.
Then a line is drawn between the point above the umbilicus and the midaxillary line to connect the upper incision line of the back with the upper incision line of the front. To be safe, double-check your drawings by pinching the tissue circumferentially.
Experience has shown us that the resection above the future scar line can be estimated about a quarter of the excess tissue, and the resection below the future scar line makes up about three-quarters of the excess tissue, in general.
In the front, the excess tissue and amount of resection varies a lot. After finalizing your drawings in the front, the posterior vectors should be marked ( Fig. 32.5 ) to get better waist contouring. The idea is to rotate the tissue inwards to get a rounder and fuller projection of the buttock and a more defined waistline.
 and intraoperative (B) demonstration of posterior vector lines. Intraoperative lateral view after incision of vectors (C) .")
If additional liposuction is required, we recommend marking the areas in a different color in concentric circles while the patient is standing up.
After orotracheal intubation and bladder catheterization, the patient is transferred to the operating room in the supine position. Here the patient is turned into the prone position, ideally from the first operating table to a second. It is advisable to use prepared soft cushions for a secure, pressure-reduced, and symmetrical positioning. We drape the entire region of the lower back, the hips, the gluteal, and the dorsal thigh region with a sterile covering, ensuring a total overview of the gluteal and the surrounding regions, including the gluteal fold.
After final closure of the gluteal region, the lateral skin excess is temporarily closed with staples, and a sterile dressing is applied ( Fig. 32.6 ). The primary covering is then removed, and the patient is turned to a second operating table back in the supine position and then transferred back to the original table using a sterile cover. In this way, a change of tables is avoidable.

Dressings and staples are removed after symmetrical positioning, and the patient is draped and covered sterile. Posterior drains may now be connected. Further, the anterior part of resection is now continued, using either the standard horizontal or fleur-de-lis excision pattern.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here