Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Increases in cardiac biomarkers of myocardial injury and particularly cardiac troponin (cTn), in the absence of analytical confounders, define the presence of myocardial injury which in the proper clinical situation can lead to the diagnosis of acute myocardial infarction (AMI). Other biomarkers such as natriuretic peptides (NPs) facilitate the diagnosis and/or exclusion of heart failure (HF). These and other important biomarkers improve patient management by leading to an earlier diagnosis, facilitating triage, helping to define treatments, and allowing for an expediated assessment of short- and long-term outcomes. Not only is patient care enhanced but with proper use, costs are constrained.
Concepts and definitions of myocardial anatomy and physiology of the heart are briefly described, along with structural changes that occur during the onset and progression of heart disease. Analytical and biochemical characteristics of cardiac troponin I (TnI), cardiac troponin T (TnT), b type natriuretic peptide (BNP), and the NTproBNP fragment (NT-proBNP) and the assays used to measure them are discussed. The clinical use of cTn is discussed in helping to diagnose and rapidly exclude AMI. Modern-day high-sensitivity assays can also aid in both primary and secondary prevention. Outcome studies are reviewed to demonstrate the role of cTn in risk stratification and appropriate selection of treatments. The clinical role of BNP/NT-proBNP in diagnosing acute and chronic HF, their emerging role in predicting the development of HF, and their use in distinguishing dyspnea of a pulmonary origin from that due to myocardial dysfunction are highlighted. The use of NP assays in defining prognosis and identifying possible treatment options is addressed. Finally, novel biomarkers for detecting myocardial injury, hemodynamic stress, inflammation, plaque rupture, and ischemia are discussed.
Although the heart is an efficient and durable pump, a variety of pathologic processes are known to diminish cardiac function, leading to a multiplicity of dysfunctional clinical states, some subtle and incipient and some overt. Acute ischemic heart disease, mostly AMI, is the most common cardiac disease. Advances in treatment over the years have blunted the extent of damage done during an MI and thus its negative impact on mortality. This and the increasing longevity in developed nations such as the United States are in part responsible for an increase in the frequency of the heart failure (HF) syndrome. Other processes can also lead to HF and often are associated with abnormal biomarkers.
The term acute myocardial infarction (AMI) refers to a situation in which death of myocytes is due to an imbalance between myocardial oxygen supply and demand. When the blood supply to the heart is interrupted, first apoptosis and then necrosis of the myocardium results. Such extensive damage is most often associated with a thrombotic occlusion superimposed on coronary atherosclerosis. Initially, it was thought that the population of myocytes was fixed; however, it is now believed that the migration of a variety of precursor stem cells has the potential at least to replace some of the damaged myocytes although the mechanisms for these effects are controversial. , It is now thought that the process of plaque rupture or erosion and thrombosis is one of the ways in which coronary atherosclerosis progresses, and that we recognize only more severe events. , Total loss of coronary blood flow results in a clinical syndrome associated with what is known as ST segment elevation AMI (STE AMI). Partial loss of coronary perfusion, if severe, can lead to necrosis as well, which is generally less severe and is known as non–ST elevation myocardial infarction (NSTEMI). Other events of still lesser severity may be missed entirely or may be called angina, which can range from stable to unstable. With the increasing sensitivity of cardiac troponin (cTn) measurements, the frequency of unstable angina (UA) is disappearing and smaller NSTEMIs are being diagnosed more frequently, but UA is not totally gone. ,
Key facts about cardiovascular disease.
The age-adjusted death rate attributable to cardiovascular disease (CVD) in the United States, based on 2017 data, is 219.4 per 100,000.
On average, someone dies of CVD (AMI, stroke, HF, etc.) every 37 seconds in the US. There are 2353 deaths from CVD each day, based on 2017 data.
On average, someone dies of a stroke every 3.59 minutes in the United States. There are about 401 deaths from stroke each day, based on 2017 data.
CVD deaths have increased from 2303 each day in 2016. Stroke deaths increased from 389.4 per day in 2016.
A total of 116.4 million, or 46% of US adults have hypertension, based on 2013 to 2016 data.
Only 1 in 4 adults, or 24.3% of US adults, reported achieving adequate leisure-time aerobic and muscle-strengthening activities to meet the physical activity guidelines, based on 2017 data.
One in six males and one in eight females in the United States are current smokers, based on 2017 data.
By 2035, 45.1% of the US population is projected to have some form of CVD. Total costs of CVD are expected to reach $1.1 trillion in 2035, with direct medical costs projected to reach $748.7 billion and indirect costs estimated to reach $368 billion.
Coronary heart disease causes over 25% of all deaths in the United States. Historically, most deaths caused by ischemic heart disease were acute, but as our therapeutic abilities have increased, the disease is becoming more chronic. Deaths that occur acutely result from ventricular arrhythmias or pump dysfunction and congestive heart failure (CHF) with or without cardiogenic shock. Death rates increase sharply with age, both during hospitalization and in the year after infarction.
Before the advent of coronary care units, treatment of AMI was directed toward allowing healing of the infarcted area. The concept that infarctions evolve over time and that their size can be moderated led to rethinking of this passive philosophy. We now know that reestablishment of perfusion reduces the extent of myocardial injury and is an important determinant of prognosis. Today the management of AMI suggested by most guidelines is aggressive and invasively oriented in the hope of reducing the extent of myocardial damage and thus improving prognosis. , In addition, prevention is finally being recognized as a key element in the long-term treatment of patients with atherosclerosis. Recently, different types of MI have been recognized. Those not related to acute plaque rupture events particularly deserve consideration and they less often require invasive management. ,
The average human adult heart weighs approximately 325 g in men and 275 g in women and is 12 cm in length. The heart is a hollow muscular organ, shaped like a blunt cone, and is approximately the size of a human fist. It is located in the mediastinum, between the lower lobes of each lung, and rests on the diaphragm. It is enclosed in a sac called the pericardium. The cardiac wall is composed of three layers: the epicardium, which is the outermost layer; a middle layer; and an inner layer, called the endocardium. The heart has four chambers. The two upper chambers are termed the right and left atria, and the two lower chambers are termed the right and left ventricles ( Fig. 48.1 ). Under normal circumstances, the atria are compliant structures, so that intracavitary pressure is low. When anatomy is normal, each atrium is connected to its ventricle through an atrioventricular (AV) valve, which opens and closes (see discussion later in this chapter). The valve on the left side is called the mitral valve and the one on the right side, the tricuspid valve. The right ventricle is banana shaped and pumps blood into the pulmonary artery through a trileaflet pulmonic valve. The left ventricle pumps blood into the aorta through a trileaflet aortic valve. The ventricles, especially the left ventricle, are thicker and less compliant in keeping with the need to generate higher pressures than the right ventricle, and intercavitary pressures are much higher than in the atria. Under normal conditions, the conduction or electrical system of the heart coordinates the sequential contraction of first the atria and then the ventricles. Given that they are connected, each side can affect the other. This sequence of activation optimizes the interaction and thus the efficiency of cardiac function.

The right and left coronary arteries originate from two of three cusps of the aortic valve. They provide blood flow and thus nutritive perfusion to the heart. The largest vessels are on the epicardium, and these can be accessed therapeutically fairly easily. Subsequent smaller branches divide to supply the remaining myocardium. The endocardium is the layer most susceptible to ischemia because its perfusion relies on the smallest vessels.
The myocardium contains bundles of striated muscle fibers, each of which is typically 10 to 15 mm in diameter and 30 to 60 mm in length. The work of the heart is generated by the alternating contraction and relaxation of these fibers. The fibers are composed of the cardiac-specific contractile proteins actin and myosin and regulatory proteins called troponins. They also contain a variety of enzymes and proteins that are vital for energy use, such as myoglobin, creatine kinase (CK), and lactate dehydrogenase (LD), some of which can be used as markers of cardiac injury.
A typical cardiac cycle consists of two intervals known as systole and diastole ( Fig. 48.2 ). During diastole, oxygenated blood returns from the lungs to the left atrium via the pulmonary veins and deoxygenated blood returns from other parts of the body to fill the right atrium. During this period, the AV valves are open, allowing passive filling of the ventricle. At the end of diastole, the atria contract, forcing additional blood through the AV valves and into the respective ventricles. During systole, the ventricles contract. This closes the AV valves when ventricular pressure exceeds atrial pressure, and the pulmonary and aortic valves are opened when ventricular pressure exceeds pressure in the pulmonary arteries and/or the aorta, and blood flows into those conduits. During systole, a normal blood pressure in the aorta is typically 120 mm Hg; during diastole, it falls to about 70 mm Hg. At rest, the heart pumps between 60 and 80 times/min. Stroke volume (i.e., the amount of blood expelled with each contraction) is roughly 50 mL, so cardiac output per minute is roughly 3 L. Typically, values are corrected for body surface area and are usually in the range of 2.5 to 3.6 L/min/m 2 . Measurements of cardiac output and ventricular filling pressures are the standards for assessing cardiac performance and function. Furthermore, therapeutic intervention in patients with heart disease often includes assessment of cardiac output and ventricular pressures.

The cardiac cycle is tightly controlled by the cardiac conducting system, which initiates electrical impulses and carries them via a specialized conducting system to the myocardium. The surface electrocardiogram (ECG) records changes in potential and is a graphic tracing of the variations in electrical potential caused by excitation of the heart muscle and detected at the body surface. Clinically, the ECG is used to identify (1) anatomic, (2) metabolic, (3) ionic, and (4) hemodynamic changes in the heart. The clinical sensitivity and specificity of ECG abnormalities are influenced by a wide spectrum of physiologic and anatomic changes and by the clinical situation.
Under normal circumstances, cardiac cycles are similar and each includes three major components ( Fig. 48.3 ): atrial depolarization (the P wave), ventricular depolarization (the QRS complex), and repolarization (the ST segment and T wave). Atrial depolarization, which is depicted by the P wave, produces atrial contraction. Ventricular depolarization, marked by the QRS complex, produces contraction of the ventricles. It is composed of as many as three deflections: (1) the Q wave, which when present is the first negative deflection; (2) the R wave, which is the first positive deflection; and (3) the S wave, which is a negative deflection after the R wave. On occasion, there is an R′, which is a second positive deflection. Whether each of these occurs depends on the path of depolarization of the ventricles, as does the significance. Thus not every QRS complex will have discrete Q, R, and S waves. The ST segment and the T wave are produced by electrical recovery of the ventricles, and their mean electrical vector is under normal circumstances concordant (i.e., in roughly the same direction) with the mean QRS vector.

A routine ECG is composed of 12 leads. Six are called limb leads (I, II, III, aV R , aV L , and aV F ) because they are recorded between arm and leg electrodes; six are called precordial or chest leads (V 1 , V 2 , V 3 , V 4 , V 5 , and V 6 ) and are recorded across the sternum and left precordium. Each lead records the same electrical impulse but in a different position relative to the heart. Areas of abnormality on the ECG are localized by analyzing differences between the tracing in question and a normal ECG in the 12 different leads.
Cardiac disease occurs in many forms. This chapter briefly covers HF, including CHF and acute coronary syndromes (ACSs), such as AMI. The vast number of other cardiac diseases are not discussed in depth here because of the smaller role of clinical laboratory tests in these disorders.
CHF is a syndrome characterized by ineffective pumping of the heart, often leading to an accumulation of fluid in the lungs. At least half comes as a result of the loss of the function of the cardiac tissue and is called heart failure with reduced ejection fraction (HFREF). The other half is due to increased stiffness of the cardiac muscle. This type of HF is referred to as heart failure with preserved ejection fraction or HFPEF. Other forms include those related to valvular heart disease and so-called high-output HF. The condition is one in which there is an abnormality of cardiac function such that the heart cannot pump sufficient blood to satisfy the requirements of metabolizing tissues, which are abnormally high.
In the United States, CHF is the only CVD with an increasing incidence. The National Heart, Lung, and Blood Institute estimates current prevalence at 4.8 million Americans and 23 million worldwide with CHF. There are approximately 580,000 new cases each year, with approximately 1 million admissions to hospitals for CHF per year. CHF is the leading cause of hospitalization in individuals 65 years of age and older.
Therapeutic options for patients with HFPEF are more limited than for those who have systolic abnormalities. , Current prognosis depends on disease severity, but overall it is poor. Mortality at 5 years is approximately 50%, and 10-year mortality is 90%. These poor outcomes are not without substantial cost, estimated at $24 billion per year in the United States.
Currently, CHF patients are staged with the New York Heart Association (NYHA) functional classifications I to IV. Class I patients are generally considered asymptomatic, with no restrictions on physical activity; class IV patients are often symptomatic at rest, with severe limitations on physical activity. The problem with this classification system is that much of it is based on subjective criteria. Thus patients with comorbidities that reduce their activities are hard to classify. In addition, dyspnea, which is the primary symptom in many of these individuals, has many causes. Finally, many patients with ventricular dysfunction modify their activities to accomplish activities of daily living and thus lack overt symptoms until late in their disease. Therefore patients with CHF often go undiagnosed and untreated early in their disease or are misdiagnosed because of conditions such as pulmonary disease. Initiating treatment in the more advanced disease state (higher degree of irreversible cardiac function and patient deconditioning) is challenging and more expensive (often requiring extended inpatient stay) and leaves patients with considerable morbidity on a daily basis. Obviously, misdiagnoses often lead to patient morbidity. That is the reason why natriuretic peptides (NPs) have been such an important advance in facilitating the diagnosis of HF , and if used properly help with treatment.
The term ACS encompasses patients who present with unstable ischemic heart disease. If they have ST segment elevation, their events are called ST elevation myocardial infarctions (STEMI) ( Fig. 48.4 ). Usually, but not always, these individuals develop Q waves on their ECGs, hence the term Q-wave MI. If patients do not have STE but have biochemical criteria for cardiac injury, they are called non-STEMI (NSTEMI), and most do not develop ECG Q waves. Those who have unstable ischemia and do not manifest necrosis are designated patients with UA. Most of these syndromes occur in response to an acute event in the coronary artery, when circulation to a region of the heart is obstructed for some reason. If the obstruction is high grade and persists, necrosis usually ensues. Because necrosis is known to take some time to develop, it is apparent that opening the blocked coronary artery in a timely fashion can often prevent some of the death of myocardial tissue. This is clearly the case with STEMI. With NSTEMI (American Heart Association [AHA]/American College of Cardiology [ACC] guidelines), early but not immediate intervention is advocated, because most often the infarct-related coronary artery is not totally occluded, and thus immediate intervention is less necessary. These syndromes are usually but not always associated with chest discomfort (see discussion later in this chapter). ,

The major cause of ACS is atherosclerosis, which contributes to significant narrowing of the artery lumen and a tendency for plaque disruption and thrombus formation. Myocardial ischemia and infarction are usually segmental diseases. In up to 90% of patients with these diseases, focal occlusion of only one of the three large coronary vessels or branches occurs. The resulting impaired contractile performance of that segment occurs within seconds and is initially restricted to the affected segment(s). Myocardial ischemia and subsequent infarction usually begin in the endocardium and spread toward the epicardium. The extent of myocardial injury reflects (1) the extent of occlusion, (2) the needs of the area deprived of perfusion, and (3) the duration of the imbalance in coronary supply. Irreversible cardiac injury consistently occurs in animals when the occlusion is complete for at least 15 to 20 minutes. Most damage occurs within the first 2 to 3 hours. Restoration of flow within the first 60 to 90 minutes evokes maximal salvage of tissue, but benefits of increased survival are possible up to 4 to 6 hours. In some situations, the restoration of coronary perfusion even later is of benefit. , The percentage of tissue at risk for necrosis (infarct size) depends on the amount of antegrade flow, the existing collateral flow, which is highly variable and difficult to predict, and the metabolic needs of the tissue.
In almost all instances, the left ventricle is affected by AMI. However, with right coronary and/or circumflex occlusion, the right ventricle also can be involved, and there is a clinical syndrome in which damage to the right ventricle predominates and is the major determinant of hemodynamics. Coronary thrombi will undergo spontaneous lysis, even if untreated, in approximately 50% of cases within 10 days. However, for patients with STEMI, opening the vessel earlier with clot-dissolving agents (thrombolysis) and/or percutaneous intervention (PCI) can often save myocardium and lives. At present, immediate PCI with stenting is the preferred therapy for STEMI. However, many hospitals cannot or do not offer urgent PCI 24 hours per day, 365 days per year. Thus clot-dissolving medications still play a major role in the treatment of these patients. In addition, it is now apparent that urgent but not necessarily immediate invasive revascularization benefits those with NSTEMI. These individuals usually have only partial coronary occlusion and smaller amounts of cardiac damage acutely. However, untreated, repetitive episodes often eventually damage larger amounts of myocardium, leading to increased morbidity and mortality over time. Treatments such as newer anticoagulants and antiplatelet and anti-inflammatory agents, in conjunction with coronary revascularization, save lives in this group.
The prognosis for patients with ischemia but without necrosis is far better. Some studies based on biomarkers would suggest that in patients with no troponin elevation, interventional therapies may be harmful. , Many of these patients are women who are known to have lower levels of cTn. With high-sensitivity assays, they will require different cutoff values, but the use of such assays will identify more women who are at risk. , A major determinant of mortality and morbidity is the amount of myocardial damage that occurs. With STEMI, most damage is acute, whereas with NSTEMI, damage may evolve as the result of repetitive events over many months; thus interrupting the process improves survival.
In many patients with AMI, no precipitating factor can be identified. Studies have noted the following patient activities at the onset of AMI: (1) heavy physical exertion, 13%; (2) modest or usual exertion, 18%; (3) surgical procedure, 6%; (4) rest, 51%; and (5) sleep, 8%. Exertion before infarction is somewhat more common among patients without preexisting angina than in those who have a history of angina.
Causes of infarction other than acute atherothrombotic coronary occlusion have been identified. For example, prolonged vasospasm can induce infarction, and spontaneous dissection is becoming more commonly appreciated in women, many of whom have fibromuscular dysplasia. In addition, it is now clear that some patients, particularly women, can have acute infarction with normal-appearing angiographic coronary arteries. Other conditions ( Box 48.1 ) can cause the death of cardiomyocytes, leading to a biochemical signal (such as increased circulating concentrations of cTns) of myocyte damage, but these conditions should not be confused with MI. Pulmonary embolism (PE) is another common cause of biochemical elevations that is secondary to right ventricular damage related to acute increases in wall stress and reduced subendocardial perfusion. ,
Trauma (including contusion, ablation, pacing, and cardioversion)
Congestive heart failure—acute and chronic
Aortic valve disease and hypertrophic cardiomyopathy with significant left ventricular hypertrophy
Hypertension
Hypotension, often with arrhythmias
Postoperative noncardiac surgery patients who seem to do well
Renal failure
Critically ill patients, especially those with diabetes, respiratory failure
Drug toxicity (e.g., adriamycin, 5-fluorouracil, herceptin, snake venoms)
Hypothyroidism
Coronary vasospasm, including apical ballooning syndrome
Inflammatory disease (e.g., myocarditis, parvovirus B19, Kawasaki disease, sarcoid, smallpox vaccination)
Post–percutaneous intervention patients whose condition appears to be uncomplicated
Pulmonary embolism, severe pulmonary hypertension
Sepsis
Burns, especially if total body surface area is greater than 30%
Infiltrative disease, including amyloidosis, hemochromatosis, sarcoidosis, and scleroderma
Acute neurologic disease, including cerebrovascular accident, subarachnoid bleeds
Rhabdomyolysis with cardiac injury
Transplant vasculopathy
Vital exhaustion/strenuous exercise
Viruses
There is a pronounced periodicity for the time of onset of STE AMI. , Often an AMI occurs in the morning hours soon after rising; this is a period of (1) increasing adrenergic activity, (2) increased plasma fibrinogen levels, (3) increased inhibition of fibrinolysis, and (4) increased platelet adhesiveness. Studies have demonstrated that the early morning peak in MI parallels the peak incidence of death from ischemic heart disease, which occurs at approximately 8 am to 9 am. A second peak has been noted at approximately 5 pm. Diurnal differences affect many physiologic and biochemical parameters; the early morning hours are associated with rises in plasma catecholamines and cortisol and increases in platelet aggregability. Tissue plasminogen activator (t-PA) activity is low and plasminogen activator inhibitor (PAI) activity is high during the early morning hours. Thus it is possible that some cyclic aspects of combined vasospastic, prothrombotic, and fibrinolytic factors, in the setting of preexisting atherosclerosis, lead to AMI. NSTEMI does not exhibit this diurnal pattern.
STE and non-STE infarctions have distinctly different short-term prognoses. STE AMI is associated with higher early and in-hospital mortality. It is said that mortality associated with STE AMI can occur up to 6 months after the event, but the vast majority (at least two-thirds) occurs during the first 30 or 40 days. It is this risk that coronary recanalization seems to benefit. NSTE AMI is associated with lower acute mortality and complication rates but a longer period of vulnerability to reinfarction and death. As a result, 1- to 2-year survival rates are similar to those for STEMI. This is why intervention has been so effective in this group.
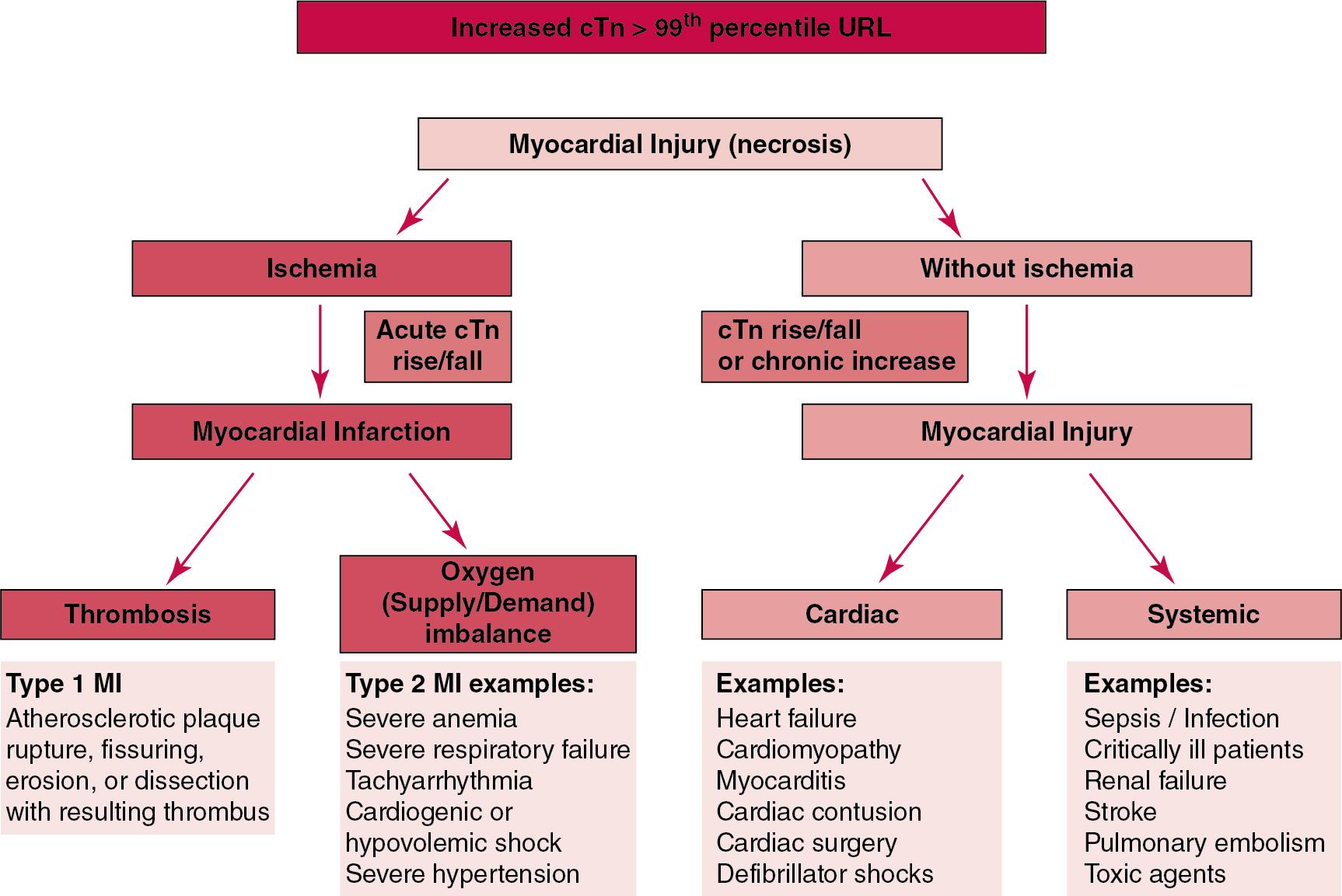
There is an additional subset of patients who have what are known as type 2 MI. Type 1 MI is the typical one due to acute atherothrombotic plaque disruption. Type 2 MI is due to supply-demand imbalance leading to ischemia. Coronary artery disease (CAD) may or may not be present but changes in oxygen demand and, usually concomitantly, myocardial supply can lead to acute ischemia and if severe enough to acute myocardial injury (an increased cTn value with a rising and/or falling pattern). An example might be severe anemia where there is reduced oxygen carrying capacity along with compensatory increases in systemic volume and with these, increased myocardial work. Type 2 MI events can have ST segment elevation, ST segment depression, or even normal ECGs. The prognoses of these patients in terms of mortality and cardiovascular events is at least as adverse as that of those with type 1 events. A similar process can occur with supply-demand imbalance or direct myocardial injury due to circulating toxins such as carbon monoxide which can cause the same pattern of cTn release. However, if ischemia is not present, the proper term for this situation is “acute myocardial injury.” Acute myocardial injury can also occur after coronary interventions and cardiac bypass surgery. Criteria for MI exist in both those situations. The key to being able to make the diagnosis is having a normal baseline cTn value.
The clinical history remains of substantial value. A prodromal history of angina is elicited in 40 to 50% of patients with AMI. Among patients with AMI who present with prodromal symptoms, approximately one-third have had symptoms from 1 to 4 weeks before hospitalization; in the remaining two-thirds, symptoms predate admission by a week or less, with one-third of patients having had symptoms for 24 hours or less. In most patients the pain of AMI is severe, but it is rarely intolerable. The pain may be prolonged, lasting up to 30 minutes. The discomfort is described as constricting, crushing, oppressing, or compressing; often the patient complains of something sitting on or squeezing the chest. Although usually described as a squeezing, choking, viselike, or heavy pain, it may be characterized as a stabbing, knifelike, boring, or burning discomfort. The pain is usually retrosternal in location, spreading frequently to both sides of the chest, and favoring the left side. Often the pain radiates down the left arm. Some patients note only a dull ache or numbness in the wrists in association with severe substernal discomfort. In some instances, the pain of AMI may begin in the epigastrium, simulating a variety of abdominal disorders; this often causes MI to be misdiagnosed as indigestion. In other patients, the discomfort of AMI radiates to the shoulders, upper extremities, neck, and jaw, again usually favoring the left side. In patients with preexisting angina, the pain of infarction usually resembles that of the angina pain with respect to features and location. However, it is generally much more severe, lasts longer, and/or is not relieved by rest and nitroglycerin.
Older individuals, patients with diabetes, and women often present atypically. For example, among individuals older than 80 years, less than 50% of those with AMI will have chest discomfort at the time of AMI. Sometimes these patients will present with shortness of breath, fatigue, or even confusion. The pain of AMI may have disappeared by the time a physician first encounters the patient (or the patient reaches the hospital), or it may persist for a few hours.
Fig. 48.5 shows the temporal sequence of early biochemical, histochemical, and histologic findings after the onset of AMI. On gross pathologic examination, AMI can be divided into subendocardial (nontransmural) infarctions and transmural infarctions. In the former, necrosis involves the endocardium, the intramural myocardium, or both without extending all the way through the ventricular wall to the epicardium. In the latter, myocardial necrosis involves the full thickness of the ventricular wall. The histologic pattern of necrosis may differ: contraction band injury occurs almost twice as often in nontransmural infarctions as in transmural infarctions. Unfortunately, the pathologic changes correlate poorly with clinical, ECG, and biochemical markers of necrosis, which is why those terms are no longer used clinically. Statistically, patients are more apt to have STE MI Q waves on the ECG and larger biochemical signals when the infarction is transmural pathologically.

In experimental infarction, the earliest ultrastructural changes in cardiac muscle after occlusion of a coronary artery, noted within 20 minutes by electron microscopy, consists of reduction in the size and number of glycogen granules, intracellular edema, and swelling and distortion of the transverse tubular system, the sarcoplasmic reticulum, and the mitochondria. These early changes are partially reversible. Changes after 60 minutes of occlusion include myocardial cell swelling; mitochondrial abnormalities, such as swelling and internal disruption; development of amorphous, flocculent aggregation and margination of nuclear chromatin; and relaxation of myofibrils. After 20 minutes to 2 hours of ischemia, changes in some cells become irreversible, and progression of these alterations occurs; additional changes include swollen sacs of the sarcoplasmic reticulum at the level of the A band, greatly enlarged mitochondria with few cristae, thinning and fractionation of myofilaments, disorientation of myofibrils, and clumping of mitochondria. Cells irreversibly damaged by ischemia are usually swollen, with an enlarged sarcoplasmic reticulum. Defects in the plasma membrane may appear, and the mitochondria are fragmented. Many of these changes become more intense when blood flow is restored.
Although it was previously believed that no light microscopic changes could be seen in infarcted myocardium until 8 hours after interruption of blood flow, in some infarcts a pattern of wavy myocardial fibers may be seen 1 to 3 hours after onset, especially at the periphery of the infarct. After 8 hours, edema of the interstitium becomes evident, as do increased fatty deposits in the muscle fibers, along with infiltration of neutrophilic polymorphonuclear leukocytes and red blood cells.
By 24 hours, clumping of the cytoplasm and loss of cross-striations are seen, with the appearance of irregular cross-bands in the involved myocardial fibers. The nuclei sometimes even disappear. Myocardial capillaries in the involved region dilate, and polymorphonuclear leukocytes accumulate, first at the periphery and then in the center of the infarct. During the first 3 days, the interstitial tissue becomes edematous. Generally, on approximately day 4 after infarction, removal of necrotic fibers by macrophages begins, again commencing at the periphery. By day 8, the necrotic muscle fibers have become dissolved; by about 10 days, the number of polymorphonuclear leukocytes is reduced, and granulation tissue first appears at the periphery. Removal of necrotic muscle cells continues until the fourth to sixth week after infarction, by which time much of the necrotic myocardium has been removed. This process continues, along with increasing collagenization of the infarcted area. By the sixth week, the infarcted area usually has been converted to a firm connective tissue scar with interspersed intact muscle fibers.
Gross alterations of the myocardium are difficult to identify until at least 6 to 12 hours after the onset of necrosis. However, several histochemical approaches have been used to identify zones of necrosis that can be observed after only 2 to 3 hours. Initially, the myocardium in the affected region may appear pale and slightly swollen. By 18 to 36 hours after onset of the infarct, the myocardium is tan or reddish purple (because of trapped erythrocytes). These changes persist for approximately 48 hours; the infarct then turns gray, and fine yellow lines, secondary to neutrophilic infiltration, appear at its periphery. This zone gradually widens and during the next few days extends throughout the infarct.
Eight to 10 days after infarction, the thickness of the cardiac wall in the area of the infarct is reduced as necrotic muscle is removed by mononuclear cells. The cut surface of an infarct of this age is yellow and is surrounded by a reddish-purple band of granulation tissue that extends through the necrotic tissue by 3 to 4 weeks. Over the next 2 to 3 months, the infarcted area gradually acquires a gelatinous, gray appearance, eventually converting into a shrunken, thin, firm scar that whitens and firms progressively with time. This process begins at the periphery of the infarct and gradually moves centrally. In addition, more hemorrhage is seen in the area of damage because of the use of potent thrombolytic and anticoagulant agents.
Intrinsic to modern-day understanding of ischemic heart disease and to the intense interest in the development of markers of inflammation is the concept that atherosclerosis is a chronic inflammatory disease. The concept is that some event damages the endothelium of blood vessels, which facilitates the egress of lipid into the subendothelial space. Putative injurious stimuli include turbulent flow in a blood vessel, which could occur for example because of hypertension or a noxious metabolite from a lipid fraction. This damage tends to occur at branch points of blood vessels. Regardless of the initial stimulus, once damaged, low-density lipoprotein (LDL) can cross into the vessel wall more easily in a nicotinamide adenine dinucleotide phosphate (NADPH) oxidase–mediated fashion. Whether minimal oxidation facilitates that egress or it occurs once the LDL is within the vessel wall is unclear, but a minimal degree of oxidation once in the vessel wall facilitates the egress of smooth muscle cells from the media of the vessel and macrophages that ingest cholesterol, hence the rationale for the measurement of oxidized lipids in blood. The process of atherosclerosis progresses slowly, with involvement of lymphocytes, monocytes, macrophages, and smooth muscle cells. The dynamic within a given plaque may vary, but there clearly is an inflammatory milieu, in part mediated by substances such as CD40 ligand, which can be measured directly or indirectly as C-reactive protein (CRP). Interleukins (IL)-1, IL-6, IL-8, and IL-18 also participate to various extents as part of this chronic inflammatory process. This process involves adherence of white blood cells to the damaged endothelial surface, with subsequent degranulation and elaboration of myeloperoxidase (MPO). A procoagulant component is due predominantly to the presence of tissue factor, which is localized immediately under the cap of the plaque. Intermittent instability is noted because of inflammatory products within the plaque that release chemicals, such as metalloproteinases. Initially the plaque expands by stretching the adventitia through a process of small ruptures with release of procoagulant and proinflammatory materials and then remodeling over time as anti-inflammatory and anticoagulant and thrombolytic substances are elaborated. This process of stretching the adventitia preserves the lumen such that by the time luminal encroachment occurs, there is a very large plaque burden.
A categorization of plaques has been proposed to facilitate identification of those at risk for rupture that could lead to an acute event. It is acknowledged that the propensity for a plaque to rupture probably reflects a systemic predilection rather than a local one. Thus for a given patient at risk, there likely are many plaques that are metabolically at risk for rupture at any given time. , High-risk plaques have the following:
an active inflammatory environment that not only may be intrinsic but may be stimulated additionally by systemic infection;
a thin fibrous cap on the endothelial surface with a large lipid core that is filled with procoagulant substances, predominantly tissue factor;
endothelial denudation and fissuring caused by the elaboration of metalloproteinases;
local high shear stress, usually because they are severe, at branch points in the vessel.
Events likely occur because of superimposed thrombosis. This can be the result of erosions on the surface of the plaque or more often rupture of the plaque at its edges, where the cap is thinnest and most of the metalloproteinases reside. If rupture induces total thrombotic occlusion, the event is usually a STE AMI. If lesser degrees of occlusion occur, an NSTE AMI or UA may ensue. One of the causes that may participate in subtotal occlusive plaque rupture involves platelets and abnormal coronary vasomotion. It is known that diseased coronary arteries respond atypically to many stimuli, often constricting rather than dilating. Because the cross-sectional area of a vessel is related to the square of the radius, even modest amounts of constriction can markedly increase the extent of occlusion. Whether constriction occurs first, leading to changes of coronary flow and platelet aggregation on the plaque, or whether platelets stick and cause the aggregation, is not certain, but these processes reinforce one another. Platelets secrete vasoconstricting substances in response to a denuded area, which expresses cell adhesion molecule (CAM) receptors. This, in addition to stagnant blood flow, will cause platelets and white blood cells to adhere to the surfaces of vessels. It appears likely that platelets adhere and enhance vasoconstriction and then break off, causing small vessel emboli, sometimes in association with plaque debris and sometimes without. These processes, in addition to a reduction in flow, can lead to necrosis or at least recurrent ischemia. It is apparent that the process that eventually leads to acute events involves a systemic propensity to platelet aggregation and inflammation, because effluent flowing from the nonculprit vessel (distant from the putative coronary lesion causing the acute event) elaborates inflammatory mediators (e.g., MPO) similar to those observed from the affected vessel. This pathophysiology has recently been supported by the Cantos trial where inhibition of the interleukin one beta inflammasome was shown to reduce ischemic events. Of interest, the antibody therapy used also reduced the incidence of lung cancer. A separate trial of low-dose methotrexate was null. Finally, necrosis when present stimulates an acute-phase reaction and inflammation. Given this pathophysiology, many therapies are now oriented toward inhibition of thrombosis, fibrinolysis, platelet aggregation, and inflammation. Many inflammatory markers are used diagnostically and for assessment of therapeutic efficiency.
The more recent appreciation of the high frequency of type 2 MI has changed some of the thinking in regard to MI. Type 1 events which depend on acute atherosclerosis are benefited by invasive intracoronary interventions. Type 2 events due to supply-demand mismatch often do not require mechanical interventions even when coronary heart disease is present. In many instances, the coronary arteries may be normal or at least not badly diseased. This entity has also resulted in rethinking which has moved those studying atherogenesis in multiple additional directions.
The diagnosis of AMI established by the World Health Organization in 1986 included biomarkers as an integral part of the disorder and required that at least two of the following criteria be met: (1) a history of chest pain, (2) evolutionary changes on the ECG, and/or (3) elevations of serial cardiac markers to a level two times the normal value. However, over time, it became rare for a diagnosis of AMI to be made in the absence of biochemical evidence of myocardial injury. A 2000 European Society of Cardiology (ESC)/ACC consensus conference updated in 2007 and 2012 (Global Task Force) , codified the role of markers by advocating that the diagnosis should be regarded as evidence of myocardial injury based on markers of cardiac damage in the appropriate clinical situation ( Box 48.2 ). The guidelines thus recognized the reality that neither the clinical presentation nor the ECG had adequate sensitivity and specificity. This guideline does not suggest that all elevations of these biomarkers should elicit a diagnosis of AMI—only those associated with appropriate clinical and ECG findings (see discussion later in this chapter). When elevations that are not caused by acute ischemia occur, the clinician is obligated to search for another cause for the elevation. In the 2007 revision of the guidelines, several types of AMI were recognized, including the spontaneous type, which is associated with plaque rupture or erosion, and the type associated with fixed or transient coronary abnormalities but not thrombotic occlusion. These are discussed in greater detail in the following paragraphs. It is also recognized that one can have a classic AMI and succumb before markers are obtained or become elevated, and cardiac injury can occur in association with cardiac procedures. In addition, criteria for different types of MI, including after coronary interventions and bypass surgery were suggested ( Box 48.3 ).
Detection of a rise and/or fall of cardiac biomarker values (preferably cardiac troponin) with at least one value above the 99th percentile upper reference interval and with at least one of the following.
Ischemic symptoms
ECG changes of new ischemia (new ST-T changes or new left bundle branch block)
Development of pathologic Q waves in the electrocardiogram
Imaging evidence of new loss of viable myocardium or new regional wall motion abnormality
Identification of an intracoronary thrombus by angiography or autopsy
Pathologic Q waves with or without symptoms in the absence of nonischemic causes
Imaging evidence of a region of loss of viable myocardium that is thinned and fails to contract in the absence of a nonischemic cause
Pathologic findings of a prior myocardial infarction.
Evidence of an imbalance between myocardial oxygen supply and demand unrelated to acute atherothrombosis meets criteria for type 2 MI.
Related to atherosclerotic plaque rupture, ulceration, fissuring, erosion, or dissection with resulting intraluminal thrombosis in one or more of the coronary arteries leading to decreased myocardial blood flow or distal platelet emboli with ensuing myocyte necrosis. The patient may have underlying severe coronary artery disease (CAD) but on occasion nonobstructive or no CAD.
Myocardial injury with necrosis in which a condition other than CAD contributes to an imbalance between myocardial oxygen supply and/or demand, for example, coronary endothelial dysfunction, coronary artery spasm, coronary embolism, tachyarrhythmia, bradyarrhythmia, anemia, respiratory failure, hypotension, and hypertension with or without left ventricular hypertrophy.
Cardiac death with symptoms suggestive of myocardial ischemia and presumed new ischemic electrocardiogram (ECG) changes or new left bundle branch block (LBBB), but death occurring before blood samples could be obtained or before cardiac biomarkers could rise; in rare cases cardiac biomarkers were not collected.
Myocardial infarction (MI) associated with percutaneous coronary innervation (PCI) is arbitrarily defined by elevation of cardiac troponin (cTn) values greater than 5×99th percentile upper reference interval in patients with normal baseline values (<99th percentile upper reference interval) or a rise of cTn values above 20% if the baseline values are elevated and are stable or falling. In addition, (1) symptoms suggestive of myocardial ischemia; (2) new ischemic ECG changes or LBBB; (3) angiographic loss of patency of a major coronary artery or a side branch or persistent slow- or no-flow or embolism; or (4) imaging demonstration of new loss of viable myocardium or new regional wall motion abnormality are required. Postmortem demonstration of a procedure-related thrombus in the culprit artery, or a macroscopically large, circumscribed area of necrosis with or without intramyocardial hemorrhage meets the type 4a MI criteria.
MI related to stent thrombosis is detected by coronary angiography or autopsy in the setting of myocardial ischemia and with a rise and/or fall of cardiac biomarker values, with at least one value above the 99th percentile upper reference interval.
MI associated with coronary artery bypass grafting (CABG) is arbitrarily defined by elevation of cardiac biomarker values greater than 10×99th percentile upper reference interval in patients with normal baseline cTn values (<99th percentile upper reference interval). In addition, (1) new pathologic Q waves or new LBBB, (2) angiographic documented new graft or new native coronary artery occlusion, or (3) imaging evidence of new loss of myocardium or new regional wall motion abnormality.
At one time, the initial ECG was thought to be diagnostic of AMI in approximately 50% of patients. As the frequency of STE AMI has diminished and the diagnosis has been made with increasingly greater sensitivity, this percentage has been greatly reduced. Serial tracings are helpful for STE AMI but not for what is now almost 70% of AMIs that are known as non-STE (NSTE) AMIs. The classic ECG changes of a STE AMI is ST segment elevation, which often evolves to the development of Q waves if intervention is not provided (see Fig. 48.4 ). Pericarditis, some normal variants, and transient causes that may result in myocardial injury such as myocarditis are well described and on occasion can mimic the changes of AMI. Most NSTE AMIs manifest as ST segment depression, with or without T-wave changes, as T-wave changes alone, or on occasion in the absence of any ECG findings. Those with ST segment change have a substantially worse prognosis.
In some patients, the clinical history and ECG may be definitive. In others, they may not be as clear. Many other clinical aspects might suggest acute ischemia as the origin of a given biomarker elevation. For example, the finding of significant coronary obstructive lesions, especially in a pattern suggestive of recent plaque rupture, is highly suggestive. At times, a positive stress test with or without imaging may be what helps in making the diagnosis. However, if the clinical situation is not suggestive, other sources for cardiac injury should be sought.
The most recent Universal Definition while providing similar operational metrics as the third iteration did increase the emphasis on the concept that an elevated cTn value was a marker of myocardial injury and that myocardial injury was an entity in and of itself. If there are changes in values over time, the myocardial injury is deemed acute. If there are not changes over time, the myocardial injury is chronic. This clarification became important as higher-sensitivity cTn assay became available and it was clear that the largest percentage of increases were not associated with ischemia. This does make the clinical triage of an increased cTn value more difficult and clinicians have in the past wished that all increases might be attributable to MI. ,
Myocardial injury/damage detected by increases of cTn above the sex-specific 99th percentile upper reference limit (URL) is almost invariably associated with adverse clinical outcomes. This statement summarizes more than 30 years of analytical and clinical investigations pertaining to the clinical utility of cTnI and cTnT. This section of the chapter will focus on cTn biochemistry; the analytical aspects of assays used to measure cTn in whole blood, serum, and plasma; preanalytical and analytical specifications that manufacturers of cTn assays need to strive to optimize; 99th percentile (normal) URL determinations; central laboratory and point-of-care (POC) testing strategies; recommendations for implementation of high-sensitivity cTn assays for appropriate (cost) utilization recommendations in clinical practice to assist in early ruling in and ruling out AMI.
The contractile proteins of the myofibril include the three troponin regulatory proteins ( Fig. 48.6 ). The troponins are a complex of three protein subunits: troponin C (the calcium-binding component), TnI (the inhibitory component), and TnT (the tropomyosin-binding component). The subunits exist in a number of isoforms. The distribution of these isoforms varies between cardiac muscle and slow- and fast-twitch skeletal muscle. Only two major isoforms of troponin C are found in human heart and skeletal muscle. These are characteristic of slow- and fast-twitch skeletal muscle. The heart isoform is identical to the slow-twitch skeletal muscle isoform, thus the reason why cTnC was never developed as a cardiac-specific biomarker. Isoforms of cardiac-specific troponin T (cTnT) and cardiac-specific troponin I (cTnI) have been identified and are the products of unique genes. Troponin is localized primarily in the myofibrils (94 to 97%), with a smaller cytoplasmic fraction (3 to 6%). Some experts in the field think that 100% of cTn is myofibril bound and that the cytoplasmic fraction represents a more easily mobilizable fraction, rather than representing a different cellular localization.
 complex and troponin forms released after myofibril necrosis. cTn1, Cardiac troponin I; cTnT, cardiac troponin T.")
cTnI and cTnT have different amino acid sequences from the skeletal isoforms and are encoded by unique genes. Human cTnI has an additional 31-amino-acid residue on the amino terminal end compared with skeletal muscle TnI, giving it complete cardiac specificity. Only one isoform of cTnI has been identified. cTnI is not expressed in normal, regenerating, or diseased human or animal skeletal muscle. cTnT is encoded for by a different gene than the one that encodes for skeletal muscle isoforms. An 11-amino-acid amino-terminal residue gives this marker unique cardiac specificity. However, during human fetal development, in regenerating rat skeletal muscle, and in diseased human skeletal muscle, small amounts of immunoreactive cTnT are expressed as one of four identified isoforms in skeletal muscle. , In humans, cTnT isoform expression has been demonstrated in skeletal muscle specimens obtained from patients with neuromuscular diseases, including muscular dystrophy, polymyositis, and dermatomyositis, as well as end-stage renal disease. , Thus care is necessary to choose antibody pairs for the cTnT assay that do not detect these reexpressed isoforms or the immunoreactive proteins expressed in neuromuscular skeletal diseases that show cross-reactivity to the commercial (Roche) cTnT assays. This may result in positive cTnT findings in the blood from noncardiac tissue (diseased skeletal muscle), that indicates a false-positive myocardial injury indication (as discussed later). Recently, a POC hs-cTnT assay (Pylon, ET Healthcare) was approved in China (by cFDA) for clinical use that does not have skeletal muscle interference, as their antibodies capture and detect different epitopes compared to the Roche antibodies. A substantial body of evidence shows that after myocardial injury or because of genetic disposition, multiple forms of cTn are elaborated both in tissue and in blood ( Fig. 48.7 ). , , These include the T-I-C ternary complex, IC binary complex, and free I; multiple modification of these three forms can occur, involving oxidation, reduction, phosphorylation, and dephosphorylation, as well as both C- and N-terminal degradation. Depending on the selection of antibodies used to detect cTnI, different antibody configurations can lead to a substantially different recognition pattern. This was recently demonstrated in a study describing cTnI and cTnT forms released after MI and how the ability to measure different post-translation cTn forms varies depending on the antibody selection used in immunoassay, as shown in Fig. 48.8 . The conclusions derived from these observations are that assays need to be developed in which the antibodies recognize epitopes in the stable region of cTnI and, ideally, demonstrate an equimolar response to the different cTnI forms that circulate in the blood. At present, standardization of cTnI assays has not been obtained. ,
 proteolysis in human heart tissue visualized with monoclonal anti-cTnI antibody. Protein extracts from tissue samples were incubated at 37 °C for 0 hour (lane 1), 2 hours (lane 2), 5 hours (lane 3), 8 hours (lane 4), and 20 hours (lane 5), separated by 10 to 20% gradient sodium dodecyl sulfate (SDS)-gel electrophoresis, transferred to a nitrocellulose membrane, and visualized by MAb 19C7. The apparent molecular masses and peptides are marked by arrows.")
 the amount of ITC complex decreases, with no full-size cardiac troponin T (cTnT) or cardiac troponin I (cTnI) found, and how antibodies are chosen are important to detect maximum amount of cTn circulating. What is not clear is whether these processes occur in the myocardium only and or in blood.")
Cummins and coworkers were the first to develop a radioimmunoassay (RIA) to measure cTnI, using polyclonal anti-cTnI antibodies. The first of many monoclonal enzyme-linked immunosorbent assays, an anti-cTnI antibody–based immunoassay was described by Bodor and colleagues. , Current contemporary, POC, and high-sensitivity (hs-cTn) assays in the marketplace are well described on the IFCC Committee on the Clinical Application of Cardiac Biomarkers (C-CB) website that is updated 2 to 3 times a year, as shown for hs-cTn assays in Table 48.1 . A timeline of hs-cTn assay regulatory approvals are shown in At A Glance. The tables demonstrate the similarities and differences in capture and detection antibodies in the heterogeneous assays used in clinical practice. In addition to these quantitative assays, several less frequently used qualitative (positive/negative) assays are also marketed as shown for representative assays in Table 48.1 .
| Company/Platform/Assay | LoD (μg/L) | 99 th % (μg/L) | %CV at 99 th | 10% CV (μg/L) | Risk Stratification | Epitopes Recognized by Antibodies | Detection Antibody Tag |
|---|---|---|---|---|---|---|---|
| Contemporary Assays | |||||||
| Abbott ARCHITECT | <0.01 | 0.028 | 15 | 0.032 | No | C: 87–91, 24–40; D: 41–49 | Acridinium |
| Beckman Coulter Access 2 | 0.01 | 0.04 | 14 | 0.06 | Yes | C: 41–49; D: 24–40 | ALP |
| Roche E170 | 0.01 | <0.01 | 18 | 0.03 | Yes | C: 125–131; D: 136–147 | Ruthenium |
| Siemens Centaur Ultra | 0.006 | 0.04 | 10 | 0.03 | Yes | C: 41–49, 87–91; D: 27–40 | Acridinium |
| Siemens Dimension RxL | 0.004 | 0.07 | 20 | 0.14 | Yes | C: 27–32; D: 41-56 | ALP |
| Siemens VISTA | 0.015 | 0.045 | 10 | 0.04 | Yes | C: 27–32; D: 41–56 | Chemiluminescent |
| Tosch AIA II | 0.06 | <0.06 | 8.5 | 0.09 | No | C: 41–49; D: 87–91 | ALP |
| Ortho Vitros ECi ES | 0.012 | 0.034 | 10 | 0.034 | Yes | C: 24–40, 41–49; D: 87–91 | HRP |
| Point-of-Care Assays | |||||||
| Abbott i-STAT | 0.02 | 0.08 | 16.5 | 0.10 | Yes | C: 41–49, 88–91; D: 28–39,62–78 | ALP |
| LSI Medience PATHFAST | 0.008 | 0.029 | 5.1 | 0.014 | No | C: 41–49; D:71–116, 163-209 | ALP |
| Quidel/Alere Triage True hs-cTnI | 1.9 | 26/14 (M/F) | 6.5 | 8.4 | No | NP (not provided) | Fluorophore |
| Radiometer AQT90 cTnI | 0.009 | 0.023 | 17.7 | 0.039 | NA | C: 41–49, 190–196; D: 137–149 | Europium |
| Radiometer AQT90 cTnT | 0.01 | 0.017 | 20.0 | 0.03 | NA | C: 125–131; D:136–147 | Europium |
| Response Biomedical RAMP | 0.03 | <0.1 | 18.5 | 0.21 | No | C: 85–92; D: 26–38 | Fluorophore |
| Roche Cardiac Reader | <0.05 | <0.05 | NA | NA | No | C: 125–131; D:136–147 | Gold particles |
| Siemens Stratus CS | 0.03 | 0.07 | 10.0 | 0.06 | Yes | C: 27–32; D: 41–56 | ALP |
| Siemens Atellica VTLi hs-cTnI | 1.6 | 27/19 (M/F) | 6.1 | 6.7 | No | C: 41–49; D: cTnC, 2 antibodies in 20-100 range | Gold nanoparticles |
| High-Sensitivity Assays | ng/L | M/F (ng/L) | ng/L | % Normals Measurable | |||
| Abbott ARCHITECT hs-cTnI | 1.2 | 34/16 | <6.0 | 3 | 96 | C: 24–40; D: 41–49 | Acridinium |
| Beckman Coulter Access hs-cTnI | 2.1 | 11/9 | <5.0 | 3.3 | 80 | C: 41–49; D: 24–40 | ALP |
| Ortho Vitros hs-cTnI | 1.0 | 19/16 | <5.0 | 6.5 | 75 | C: 24–40, 41–49 D: 87–91 | HRP |
| Roche E170 hs-cTnT (Gen 5 USA) | 5 | 20/13 | <8.0 | 13 | 25 | C: 136–147; D: 125–131 | Ruthenium |
| Siemens Atellica hs-cTnI | 1.6 | 54/34 | <4.0 | <6 | No | C: 41–50C: 41–50, 171–190 D: 29–34 |
|
Nonstandardization challenges do prevent the ease of switching from one assay to another in clinical practice or research. First, no primary reference cTnI material is currently available for manufacturers to use in standardizing cTnI or cTnT assays. Second, cTn concentrations fail to be consistently harmonized between assays because cTnI circulates in its numerous forms and the different antibodies used in assays recognize different epitopes of cTnI, even for different assays and instruments marketed by the same manufacturer, as shown in the IFCC website. The cTnI Standardization Subcommittee of the American Association for Clinical Chemistry (AACC) in collaboration with the National Institute of Standards and Technology (NIST) did develop a cTnI reference material (SRM 2921), a TnC-cTnI-cTnT complex purified from human heart under nondenaturing conditions. A cTnI value was assigned by a combination of reversed-phase liquid chromatography with ultraviolet detection and amino acid analysis. However, it appears to be of limited value, at best used for the potential of harmonization or possible use for cTnI traceability but was not helpful as a common calibration material for either cTnI or cTnT. Further, it appears this material is now out of stock. For complete standardization for cTnI assays, manufacturers would need to agree to use the same capture and detection antibodies showing similar specificity for the many cTnI molecules circulating in the blood. This would also overcome matrix effects that a current IFCC working group is investigating based on a serum-based common reference material for calibration, a process that will unlikely solve any of the above limitations. Several adaptations of the Roche cTnT immunoassay have been described over the years. , , , The current Roche FDA-cleared assay available in the United States (Gen 5) and the assay used worldwide outside the United States (designated hs-cTnT by Roche) involve two monoclonal, anti-cTnT antibodies. During one of those alterations, the negative effects of heparin were eliminated. Although skeletal muscle TnT itself may appear to be a potential interferent, recent studies in patients with neuromuscular disease have described false-positive cTnT findings in plasma, proposed to be an immunoreactive protein that does cross-react with both cTnT assays. Because of calibration differences between the 4th generation, high-sensitivity (hs-TnT), or what is called Gen 5 in the USA by Roche, and POC assays or cTnT, minor differences in measured cTnT concentration have been shown between instruments. , , , Further, the two different hs-cTnT assays from ET Healthcare and Roche, as for cTnI assays, are not standardized or harmonized.
In 2001 and 2004 the IFCC Committee on Standardization of Markers of Cardiac Damage (C-SMCD) recommended quality specifications for contemporary cTn assays. , These specifications were intended for use by the manufacturers of commercial assays and by clinical laboratories using cTn assays. The overall goal was to attempt to establish uniform criteria so that all assays could be evaluated objectively for their analytical qualities and clinical performance. Both analytical and preanalytical factors were addressed. With the increasing conversion rate of contemporary assays to the hs-format, expert consensus recommendations were published by the AACC Academy in collaboration with the International Federation of Clinical Chemistry and Laboratory Medicine Task Force on Clinical Applications of Bio-Markers (IFCC TF-CB). The document focused on clinical laboratory practice recommendations for hs-cTn assays utilizing expert opinion class of evidence to focus on the following 10 topics ( Box 48.4 ): (a) quality control (QC) utilization, (b) validation of the lower reportable analytical limits, (c) units to be used in reporting measurable concentrations for patients and QC materials, (d ) 99th percentile sex-specific URLs to define the reference interval; (e ) criteria required to define hs-cTn assays, (f ) communication with clinicians and the laboratory’s role in educating clinicians regarding the influence of preanalytical and analytic problems that can confound assay results, (g ) studies on hs-cTn assays and how authors need to document preanalytical and analytical variables, (h ) harmonizing and standardizing assay results and the role of commutable materials, (i ) time to reporting of results from sample receipt and sample collection, and (j ) changes in hs-cTn concentrations over time and the role of both analytical and biological variabilities in interpreting results of serial blood collections. Publications have also attempted to provide guidance to regulatory agencies, health care providers, and laboratories. , A meeting between US laboratory medicine, emergency medicine, and cardiology biomarker experts and the FDA resulted in an opinion/perspective article with the objective of providing guidelines for uniform analytical and clinical standards for 510k studies being performed by manufacturers seeking cTnI and cTnT 510k assay clearance. Recommendations provided to the FDA addressed the following points: (1) the number of reference individuals for determination of a 99th percentile upper reference interval, (2) limit of quantification, (3) total imprecision requirements, (4) enrollment of subjects for diagnostic studies, (5) patient adjudication processes, and (6) clinical end points and time limits to assess outcomes. A primary focus was to ensure that the suggested protocols also apply to hs-cTn assays. Unfortunately, the expert recommendations were not endorsed by the FDA.
Quality control (QC) utilization
Assay limits validating the lower reportable analytical limits (LOD)
Units to use in reporting measurable concentrations for patients and QC materials
99th percentile sex-specific upper reference limits defining the reference interval
Criteria required to define hs-cTn assays
Communication with clinicians and laboratory role in educating clinicians on the influence of preanalytic and analytic issues that confound assay results
Authors/manuscripts need to document preanalytical/analytical variables on hs-cTn assays
Harmonizing and standardizing assay results and role of commutable materials
Time to reporting of results from sample receipt and sample collection
Changes in hs-cTn concentrations over time and role of both analytical and biological variabilities in interpreting results of serial blood collections
Advancements in cTn assay technology have challenged clinicians and laboratory scientists to better understand the analytical characteristics of cTn assays to determine which assays are best for optimal patient care. International guidelines have defined an increased cTn above the 99th percentile URL as an abnormal result, as described in the clinical section. , , , , , Whether a clinical laboratory defines an abnormal result above the 99th percentile as a critical value needs to be assessed and determined by each individual laboratory. What has been lacking until recently was a uniform approach to define the 99th percentile across the heterogeneity of assays. A review article has addressed the vast literature regarding defining normality, on a global basis. Guidance is now proposed by experts (cardiology, emergency, laboratory medicine) by the joint AACC Academy and IFCC C-CB publication. Despite evidence-based literature demonstrating that cTn concentrations tend to increase in individuals older than 60 years, likely because of unrecognized comorbidities, 99th percentiles are often determined across wide age ranges using subjects as old as 80 years (convenience samples). , , , , Further frustrating the problem of selecting relevant reference subjects is the fact that in clinically defined normal individuals without known CVD, increased cTn concentrations are indicative of a significantly higher risk for death. , Given such problems, most laboratories (1) accept the manufacturer’s reference interval from the package insert, (2) perform an underpowered normal study to establish a reference interval, or (3) accept a URL cutoff value published in the literature, which vary for the same assay between studies depending on the populations studied. Implementation of the 99th percentile URL, especially by sex-specific URLs, has not been globally accepted by laboratories, most likely because of pressures by clinicians who have been concerned that the imprecision of assays at the 99th percentile does not always meet the Fourth Universal Definition of MI (2018) recommendation of a 10% CV at the 99th percentile; analytical noise around the 99th percentile could result in a false-positive increase of cTn in patients without myocardial injury. However, the Universal Definition does clearly state that assays are clinically usable with up to a 20% CV at the 99th percentile. At least two serial samples are required to demonstrate a rising or falling cTn pattern.
A recent study has attempted to define how to select healthy reference subjects in deriving 99th percentiles for cTn assays. Its goal was to determine overall and sex-specific 99th percentile URLs in 9 hs-cTnI and 3 hs-cTnT assays using a universal sample bank (USB). The USB comprised healthy subjects, 426 men and 417 women, screened using a health questionnaire. Hemoglobin A1c (>URL 6.5%), NT-proBNP (>URL 125 ng/L), and eGFR (<60 mL/min) were used as surrogate biomarker exclusion criteria along with statin use. 99th percentiles were determined by nonparametric, Harrell-Davis bootstrap, and robust methods. Subjects were ages 19 to 91 years, Caucasian 58%, African American 27%, Pacific Islander/Asian 11%, other 4%, Hispanic 8%, and non-Hispanic 92%. The overall and sex-specific 99th percentiles for all assays, before and after exclusions ( n = 694), were influenced by the statistical method used, with substantial differences noted between and within both hs-cTnI and hs-cTnT assays. Men had higher 99th percentiles (ng/L) than women, as shown in Fig. 48.9 . The Roche cTnT and Beckman and Abbott cTnI assays (after exclusions) did not measure cTn values at ≥ the limit of detection (LOD) in ≥ 50% women. Representative histograms for the current hs-cTnI and hs-cTnT assays used worldwide demonstrate substantial differences in their abilities to measure concentrations greater than LOD especially in females, as shown in Fig. 48.10 . The findings have important clinical implications in that sex-specific 99th percentiles varied according to the statistical method and hs-cTn assay used, not all assays provided a high enough percentage of measurable concentrations in women to qualify as a hs-assay, and the surrogate exclusion criteria used to define normality tended to lower the 99th percentiles.
 and percent measurable concentrations (circles) in a presumably healthy population for high-sensitivity cardiac troponin assays for males (A) and females (B). cTnI, Cardiac troponin I ; cTnI, cardiac troponin T; ETH, ET healthcare.")
 hs-cTnI and (B) hs-cTnT assays of plasma specimens from apparently healthy individuals. cTnI, Cardiac troponin I ; cTnI, cardiac troponin T.")
Consensus guidelines from the Fourth Universal Definition of Myocardial Infarction (2018), the joint laboratory medicine AACC Academy and International Federation of Clinical Chemistry (IFCC) C-CB, the ACC/AHA and Epidemiology groups, the ACC Foundation, and the European Clinical and Laboratory groups have recommended that, in patients who present with ischemic symptoms, a rising or falling serial pattern with at least one cTn concentration higher than the sex-specific 99th percentile URLs, during the first 24 hours after onset of symptoms indicates myocardial injury/necrosis/cell death. Fig. 48.11 shows a representative profile of the rise and fall pattern of cTn for type 1 MI, type 2 MI, and chronic myocardial injury patients. If this elevation occurs in the clinical setting of ischemia consistent with MI, that diagnosis should be made (see Box 48.2 ). It is recommended that cTn assays with appropriate QC and optimal total imprecision (CV ≤ 10%) at the 99th percentile URL are preferred. , Better imprecision at low cTn concentrations, based on high-sensitivity assays, appears to improve the value of interpreting cTn as an early rule out and rule in diagnostic tool and risk indicator (within 3 hours of baseline sampling), as will be discussed in the clinical section. Use of contemporary or POC cTn assays with intermediate imprecision (10 to 20% CV) at the 99th percentile, however, is deemed clinically acceptable and does not lead to patient misclassifications when serial cTn results are interpreted.

A challenge that needs to be considered as hs-cTn assays with improved analytical sensitivity become increasingly incorporated in laboratory practice is determining how these new assays compare with the older contemporary assays. In essence, as will be discussed below, the hs-assays improve clinical practice for diagnostics and risk assessment for more rapid (early) and improved patient management and care. Diagnostic clinical sensitivities using specimens collected serially from presentation for detection of MI have improved from 15 to 35% for the initial generations of cTn assays, to 50 to 75% for current contemporary assays, and to more than 80% for hs-assays, as shown in Fig. 48.12 . To exclude an AMI with contemporary assays, the Global Task Force originally recommended a 6-hour period for assessing the optimal negative predictive value (NPV) for ruling out AMI. With hs-cTn assays, the timing for ruling out an AMI with greater than 99.5% NPV and 99% clinical sensitivity has decreased to less than 2 to 3 hours from the time of baseline/first blood draw, better defining the clinical playing field for hs-assays used to assist in the diagnosis of MI, rule out MI, and better stratify patients for risk of adverse events. The basis for these early approaches was that these early signals anticipated that eventually the criteria proposed by the Universal Definition of MI would be met. Further, studies consistently now show by using hs-assays that in patients presenting with a low clinical likelihood of ACS, both hs-cTnI and hs-cTnT baseline concentrations below an assay’s LOD with a nonischemic ECG can be used to rule out AMI, as will be discussed later in the chapter. Measurable cTn concentrations but less than the sex-specific 99th percentile URL or less than overall 99th percentile URL and without a significant delta (change) value (assay dependent) 1, 2, or 3 hours after the baseline sample, can also provide an NPV greater than 99.5% for early rule out in a substantial number of patients, as will be discussed later in the clinical section that addresses the caveat of early presenters at less than 2 hours following the index event onset. As the use of hs-cTn assays grows in the USA, having already done so worldwide outside the USA, triage of patients in the emergency department (ED) will be significantly improved, allowing for more rapid triage to an appropriate level of care or earlier discharge home, with minimal risk for an adverse event, with substantial financial savings to the health care system/hospital. Ongoing analytical and clinical development is underway to validate hs-POC cTn assays.
 comparing a high-sensitivity and contemporary cardiac troponin I assay (cTnI) .")
To address the conundrum of concentration differences across assays that have been shown for contemporary cTn assays, appropriate-sized, population-based, direct comparisons of hs-cTn assays have been carried out. Only the IFCC C-CB and the AACC Academy have provided an international group of experts that have published their opinion or guideline that defines an “apparently healthy population.” This approach suggests the use of a common normal reference population within a focused, healthy, age-defined group similar in age to patients presenting with symptoms suggestive of ACS to establish 99th percentile URLs, with the use of surrogate biomarkers to exclude silent pathophysiologies. Multiple studies using first-generation, contemporary, and hs-cTn assays have demonstrated that the cTn 99th percentile strongly depends on selection of individuals to be included in the reference population. Examining multiple contemporary and POC assays, the percent of measurable concentrations below the 99th percentile concentration were all less than 50%. Further, the 99th percentile URL variability among assays is substantial, further exemplifying the lack of cTnI and cTnT assay standardization. hs-cTn assays in comparison have demonstrated near-Gaussian distributions (see Fig. 48.10 ; assay dependent), with sex-specific URL differences that are not observed with contemporary and POC assays because of their lack of analytical sensitivity.
A two-tiered system of analysis using both 99th percentiles and imprecision values at the 99th percentile, based on a younger, healthy reference population that is diversified by sex, race, and ethnicity, has been proposed. This approach has been challenged because (1) it does not provide an age-matched normal cohort matching the ACS patient population that typically presents to rule out an AMI and (2) it is not based on clinical diagnostic or outcomes data at the 99th percentile URL. The scorecard approach was based on a published scorecard concept to capture the essence of which assays are acceptable for use in clinical practice and to facilitate the transition to hs-cTn assays; based on designations of the total imprecision (% CV) of each assay at the 99th percentile and how many specimens from normal individuals have cTn concentrations that are actually measurable below the 99th percentile. The ultimate goal is to have all assays be level 4 guideline acceptable. A point of controversy does exist regarding the way Roche has commercially designated their cTnT assay as high-sensitivity; the evidence-based literature does not support its designation as an hs-assay because the assay consistently measures less than 50% of normal female subjects above the LOD (see Fig. 48.9 ); as such they have designated their FDA-cleared assay as Gen 5 (even though it is the same assay designated high sensitivity for sale outside the USA). The likely clinical effects of using hs-assays rated by the scorecard as “guideline acceptable” (≤10% CV) or contemporary “clinically usable” (11 to 20% CV) include: (1) all providers will more accurately detect patients within the normal range and with minor myocardial injury, independent of the pathophysiologic mechanism; (2) emergency medicine physicians will achieve improvements in triage through earlier ruling out (improved NPV and sensitivity) and ruling in (improved positive predictive value [PPV] and specificity) of patients with MI; (3) cardiology, internal medicine (hospitalists), and family practice physicians will see improved outcomes for both inpatients (hospitalized, short-term risk) and outpatients (posthospitalization, long-term risk) because of the ability to detect injury earlier, and manage patients accordingly, compared to other diagnostic tools; (4) other medical specialty physicians will be better able to identify patients early at presentation, often without clinical symptoms, who may be at risk of cardiac-related adverse outcomes; and (5) clinical trial investigators will be able to identify appropriate and optimal patient reenrollment and outcome measures.
Optimal discrimination between a small amount of myocardial injury and analytical noise requires assays that have low limits of quantitation (LOQ; lowest concentration at 20% CV) and LOD, and require low imprecision at low cTn concentrations. Efforts to improve the imprecision of cTn assays are always warranted. Irrespective of how the testing is performed, whether in the central laboratory or at the bedside using POC assays, manufacturers need to define the imprecision profile (i.e., the scatter graph showing the %CV versus increasing cTn concentrations obtained using the Clinical and Laboratory Standards Institute [CLSI] EP5-A2 protocol) by assessing pools of human samples containing different cTn concentrations. In particular, at least two cTn concentrations that cover the range between the LOD and the 99th percentile URL of the assay are recommended to be included; one around the LOD and one around the female and or male 99th percentile URL. Imprecision characteristics, including the 10 and 20% CV concentrations, the LOD, and 99th percentile data from current commercially available assays for contemporary, POC, and hs-cTn assays need to be addressed. It is concerning in the context of clinical practice that there still is some variability for an individual patient’s cTn concentration caused by different lots of calibrators and different antibodies that do not recognize the same epitopes when the same sample is measured using the same manufacturer’s assay in different laboratories. Such discrepancies highlight the need for local analytical validation whenever feasible. Laboratories at a minimum should determine total imprecision at the LOD and at each sex-specific URL and should continue to monitor assay performance over time using internal QC materials that include the lowest concentration corresponding to the 10 and 20% CVs, as well as at the 99th percentile if different from the 10% CV concentration. Patient specimen comparisons such as regression analysis and bias assessment should be performed according to CLSI guidelines and as outlined by AACC Academy and IFCC C-CB.
Many organizations, including the AACC Academy, IFCC C-CB, Global Task Force, and Cardiology and Epidemiology Societies have outlined analytical recommendations for cTn (as well as for other biomarkers of ACS). The most current recommendations by the AACC Academy and IFCC C-CB for the appropriate implementation and utilization of cardiac biomarkers, specifically for hs-cTn assays, to aid in the early rule-in and rule-out diagnosis of MI, complementing the quality specifications for contemporary cTn assays previously published, follow (see Box 48.4 ). ,
Recommendation 1: For hs-cTn assays, laboratories should measure at least three different concentrations of QC materials at least once per day. For contemporary cTn assays, at least two different concentrations of QC materials must be assessed at least once per day. Before patient testing can be initiated, the values for acceptable imprecision must be, at a minimum, consistent with those specified by the manufacturer.
QC concentrations for hs-cTn assays (ng/L units with one decimal place):
Concentration 1: a concentration between the LOD and the lowest sex-specific 99th percentile.
Concentration 2: a concentration that is higher than but close (within 20%) to the highest sex-specific 99th percentile URL.
Concentration 3: a concentration that challenges the upper analytical range of reportable cTn results (e.g., multiples above the 99th percentile concentration).
QC concentrations for contemporary (pre-hs assays) cTn assays (ng/mL or μg/L units) with three decimal places:
Concentration 1: a concentration at or close to (within 20%) the overall 99th percentile.
Concentration 2: a concentration that challenges the upper analytical range of reportable cTn results (e.g., manufacturer).
Recommendation 2: During initiation of hs-cTn testing, clinical laboratories should validate the LoB, LOD outside the United States, or LoQ as applicable per FDA regulations in the United States. These analytical parameters should be validated minimally on an annual basis or more frequently as deemed necessary.
Recommendation 3: Report hs-cTn in whole numbers, using ng/L without decimal points. For reporting QC values, we recommend one decimal point. For contemporary cTn assays, units are reported in ug/L to two significant figures, with QC values reported to three significant figures.
Recommendation 4: Use a defined reference population to report 99th percentile concentrations according to sex-specific cutoffs for hs-cTn assays. This recommendation is not relevant for contemporary cTn assays. A minimum of 300 men and 300 women per group of healthy individuals is required for appropriate statistical determination for the 99th percentile (the robust statistical method is not recommended) of a normal reference URL for both cTn and CK-MB.
Recommendation 5: We recommend that assays unable to detect cTn at concentrations at or above the LOD in at least 50% of healthy men and women be labeled as contemporary cTn assays.
Recommendation 6: Laboratories should communicate with clinicians on the influence of preanalytic and analytic problems that confound hs-cTn assays. For institutions or health systems using 2 or more cTn assays, differences in the sensitivity of the various cTn assays should be explained to assist clinicians in understanding discrepancies when patients are transferred from other facilities
Recommendation 7: Authors of studies using cardiac biomarkers, including hs-cTn, should document preanalytical and analytical variables important to the study and be explicit concerning their postanalytical interpretative approaches.
Recommendation 8: Commutable materials should be developed for use in harmonizing and standardizing cTn measurements.
Recommendation 9: cTn results should be reported within 60 minutes or less of when a sample is received. There should be continued efforts to improve this to a time of 60 minutes from when the sample was collected.
Recommendation 10: The laboratory should help educate clinicians on the importance of specific metrics by which true clinical changes in cTn concentrations can be distinguished from analytical and biological variabilities.
Defined by:
%CV 10% or less at 99th percentile URL
cTn above the limit of detection (LOD) in 50% or greater of normal for both males and females individually, not for combined of both sexes.
Values will be reported as whole numbers, in nanogram per liter (ng/L), and sex-specific URLs
Laboratory Medicine Practice Guidelines for non–hs-cTn POC testing in ACS will be updated in 2021 by the AACC Academy and IFCC C-CB. Current guidelines address administrative issues, cost-effective usage, and clinical and technical performance of cardiac biomarkers in the ED. Eleven proposed elements of the guidelines are as follows:
Members of EDs, primary care physicians, cardiologists, hospital administrators, and clinical laboratory staff should work collectively to develop an accelerated protocol for the use of biomarkers in the evaluation of patients with possible ACS.
This protocol should be applied to facilitate the diagnosis of MI in the ED or to continue the diagnosis at other locations in the hospital.
Quality assurance measures should be used with monitoring to reduce medical errors and improve patient treatment.
Blood collection should be referenced to the time of presentation in the ED and, if available, to the reported time of symptom onset.
The interdisciplinary team should include personnel who are knowledgeable about local reimbursement.
The laboratory should perform biomarker testing with a maximum turnaround time (TAT) of 1 hour and optimally 30 minutes. The TAT is defined as the time from blood collection to reporting of results to the provider.
Institutions that cannot consistently provide a 1-hour TAT should consider POC testing assays if clinically necessary.
Performance specifications and characteristics for central laboratory and POC testing assays should not differ.
Laboratory personnel must be involved in selection of POC assays, training of individuals to perform the analysis (whether laboratory or nonlaboratory personnel), maintenance of POC equipment, oversight of proficiency and competency of operators, and compliance with requirements of regulatory agencies.
POC assays should provide quantitative results.
Manufacturers are encouraged to work closely with professional organizations to develop structured committees and establish quality performance specifications for new biomarkers.
No hs-cTn assays are available in a POC assay format for use in the USA. , Globally, POC testing is available for both hs-cTnI and hs-cTnT in China (ET Healthcare both cleared by cFDA). Some companies claim using plasma their POC assays to be hs, however, evidence-based studies are lacking for whole blood and their ability to detect greater than 50% of normal subjects for females. For both POC and central laboratory testing, and for practical considerations, anticoagulated whole blood or plasma appears to be the optimal specimen for rapid emergent processing. This eliminates the extra time needed for clotting and additional sample handling. Differences have been described among different plasmas, whole blood, and serum specimens for cTnI concentrations measurement by an individual assay. Both ethylenediaminetetraacetic acid (EDTA) and heparin are known to interfere with cTnI and cTnT antibody-binding affinity, as well as produce some matrix effect differences. , It is not recommended that different sample types are mixed during an individual’s work-up when serial, timed samples are being drawn to rule in or out an MI. The interfering effect of blood tube additives has been extensively described in the Chapter 5 .
Although clinicians and laboratorians continue to publish guidelines supporting TATs of less than 60 minutes for cTn, most studies demonstrate that TAT expectations are not being met in a large proportion of hospitals. While no recent studies have examined this question, as an example, the College of Pathologists (CAP) Q-Probe Survey study of 7020 cTn and 4368 CK-MB determinations in 159 hospitals demonstrated that median and 90th percentile TATs for troponin and CK-MB were as follows: 74.5 minutes, 129 minutes; and 82 minutes, 131 minutes, respectively. Less than 25% of hospitals were able to meet the less than 60-minute TAT, representing the biomarker order-to-report time. However, data have shown that implementation of POC cTn testing can decrease TATs to less than 30 minutes in cardiology critical care and short-stay units. ,
With the implementation of hs-cTn testing, which has been shown to provide early rule-out and early rule-in protocols within 3 hours of baseline blood sampling (discussed later in the chapter), the role of POC testing will need to be better defined. In medical centers where acceptable TATs are not being meet, where contemporary cTn assays are still utilized, the role of POC, especially in rural settings, may still be important whether a contemporary or hs assay is used. The following example, while 10 years old, demonstrates how an institution that addressed a poor TAT problem for a contemporary cTn assay improved laboratory services through cross-department cooperation. , Based at a 400-bed county hospital with 120,000 patient presentations per year through the ED, approximately 30,000 cTn orders per year were tested for both outpatients and the 1800 to 2000 patients admitted for short- or long-term care. A 2-month survey of the TAT for cTn showed a 90% TAT of 118 minutes. To better meet the published guideline of 60 minutes 100% of the time, the laboratory medical director, the emergency medicine staff whose primary responsibility involved ACS MI presentations, and the cardiology medical director who was responsible for the 11-bed cardiac 24- to 48-hour observation unit (cardiac short-stay unit [CSSU]), 28-bed telemetry unit, and 8-bed cardiac care unit (CCU) met and designed an ACS triage protocol. POC cTnI assay systems (using whole blood) were placed in the small ED laboratory, staffed by the clinical laboratory around the clock, in support of the hospital’s level 1 trauma center. Additional POC assays were placed in the CSSU, in which 42 nurses were trained by the laboratories’ POC coordinators. The flow of specimens was such that initial presentation cTnI requests ordered through the ED were analyzed in the ED laboratory, approximately 6000 to 8000 per year. TAT from the time of blood draw to the provider result report was less than 18 minutes, 100% of the time. The use of POC testing eliminated the additional time needed to transport and process specimens that would have been needed to analyze specimens in the central laboratory. Patients admitted to the hospital to rule in or rule out MI who were at low risk were admitted to the CSSU, where staff nurses provided less than 20-minute TAT 100% of the time from blood draw to results to provider. In the CSSU, in compliance with the hospital protocol that at least a 6-hour post-presentation sample had to remain normal for cTnI, two blood specimens, in addition to the ED presentation sample, were measured at 4 and 8 hours. The uniform timed ordering protocol for ruling out MI included four timed draws at 0, 4, 8, and 12 hours. In patients admitted to the telemetry unit or the CCU, a dedicated blood draw was tubed to the central laboratory, where specimens were given priority-testing status, and thus met a TAT of less than 60 minutes 98% of the time. During this process, it was recognized that POC testing was not cost-effective for patients in telemetry or CCU units. These were mostly patients at moderate to high risk in whom a clinical diagnosis had already been made; thus urgent cTn values were less necessary. The CSSU was successful in decreasing the length of stay in the unit by 0.8 day through implementation of POC testing, allowing triage to lower levels of care and/or discharge on a 24/7 basis. Although the direct cost per assay reagent increased from $3.83 (central laboratory) to $10.51 (POC testing), the overall cost to the patient decreased by more than $4000 per admission, primarily based on decreased bed charges from a costlier cardiac bed to a less expensive general medicine bed or to discharge. These data highlight the continued need for laboratory services and health care providers to work together to develop better processes to meet a TAT less than 60 minutes, as requested by physicians. A list of POC testing assays and manufacturers’ analytical claims is found on the IFCC C-CB website.
It has been shown that a less-sensitive POC assay may miss a positive cTn value that would be detected as increased by a more-sensitive contemporary assay, as noted in Fig. 48.13 . Further, POC cTnI assays also suffer from the lack of assay standardization. Fig. 48.14 shows that in a representative patient presenting with an evolving AMI, serial cTnI concentrations vary substantially between three POC assays versus a contemporary assay, with substantial variability in clinical sensitivities between assays. Contrary to the poor analytical sensitivity of POC assays, Fig. 48.15 shows that for an hs-cTnI assay, rising values are detected earlier even compared to a contemporary cTnI during the early course of an AMI. These data point to the need for clinical laboratories to replace contemporary cTn assays with hs-cTn assays.

 versus cTnI concentration for 5 cTnI assays; respective clinical sensitivities shown at baseline for assays.")

With the increasing number of hs-cTnI and hs-cTnT assays cleared for clinical use globally (see IFCC website tables) numerous early rule-out and rule-in protocols are being used in clinical practice, including a recently published machine learning algorithm. The Fourth Universal Definition of Myocardial Infarction (2018) provides an excellent expert consensus resource for navigating both the pathophysiology of myocardial infarction (MI) and the role of cTn monitoring, complementing the IFCC-C-CB and AACC Academy analytical guidelines. The guideline provides new and updated information addressing the following pertinent to our chapter.
New:
Differentiation of MI from myocardial injury.
Highlighting peri-procedural myocardial injury after cardiac and noncardiac procedures as discrete from MI.
Use of cardiovascular magnetic resonance to define etiology of myocardial injury.
Use of computed tomographic coronary angiography in suspected MI.
Updated:
Type 1 MI: Emphasis on the causal relationship of plaque disruption with coronary atherothrombosis.
Type 2 MI: Settings with oxygen demand and supply imbalance unrelated to acute coronary atherothrombosis.
Type 2 MI: Relevance of presence or absence of CAD to prognosis and therapy.
Differentiation of myocardial injury from type 2 MI.
Types 4–5 MI: Emphasis on distinction between procedure-related myocardial injury and procedure-related MI. The need for a normal baseline value is a key element.
cTn: Analytical issues for cTns.
Emphasis on the benefits of high-sensitivity cTn assays.
Considerations relevant to the use of rapid rule-out and rule-in protocols for myocardial injury and myocardial infarction.
Issues related to specific diagnostic change (“delta”) criteria for the use of cTns to detect or exclude acute myocardial injury.
International guidelines have suggested general times that cTn testing should be used to evaluate ruling in or out an AMI after a patient presents to an ED. It is not atypical for the laboratory to receive excessive cTn test orders well after a patient has been ruled in or ruled out for an MI, at a considerable unnecessary expense to the health care system. There is a substantial diversity across hospitals within the United States and internationally on how cTn testing is ordered, ranging from a hospital-wide serial order set such as at presentation, 3, 6, and 12 hours for contemporary assays compared to 0/1 hour, 0/2 hours, 0/3 hours, and 6 hours for hs-cTn assays or to the ability to order cTn as a single test order at any time without any uniformity across a hospital/medical center. These orders are often complicated within teaching hospitals where both attending physicians and resident physicians may place multiple order sets, with substantial duplication and excessive cTn testing. Studies have made interesting observations in this regard. First, in a monitored telemetry unit staffed by attending and resident physicians, an excessive number of cTnI tests were ordered after the diagnosis of both an MI (48% over testing) and no-MI (39% over testing) already had been established, with an average of approximately 6 to 7 cTn tests per diagnosis. Second, in the course of reviewing approximately 6000 cTn orders over 2 months in a 420-bed primary care hospital, providers (42% of whom were residents) acknowledged and overrode an electronic alert 97% of the time after a second set of serial cTn orders was placed, with 93% in non–ACS-related patients. Third, among patients with cTn increases, cardiologists are less likely than emergency medicine physicians to classify cTn orders as appropriate; discordance in appropriateness occurred most frequently when the diagnoses were myocardial injury or type 2 myocardial infarction, and perceived appropriateness of cTn testing is influenced by sub-specialty, diagnoses, and symptoms, with more research and guidance needed to refine the use of the test.
Overall, better education and monitoring of cTnI orders in the diagnosis or exclusion of MI is needed, with the need for electronic ordering review and/or electronic hard stop or manual discontinuation to be implemented when excessive testing is recognized. Proactive test use by laboratory professionals regarding cTn orders, working in concert with their clinical colleagues and information technology counterparts, should become a high priority in clinical laboratory practice to assist in health care savings.
cTns have been available for clinical use since 1995, when the first cTn T (cTnT) assay was regulatory approved outside the USA. Since that time, enhanced diagnostics and particularly improved sensitivity in females led to more frequent and more accurate diagnosis of cardiovascular abnormalities, especially with the growing implementation of high-sensitivity cTn assays. Initial use of these assays was influenced in large part by CK-MB. CK-MB is substantially less sensitive and less cardiac specific than cTn, but because of its long use, it became entrenched in the thinking of clinicians and laboratorians. For this reason, perhaps, the first set of guidelines by the National Academy of Clinical Biochemistry (NACB) attempted to compromise between the use of these CK-MB and cTn using two cutoffs. One cutoff was selected to be equivalent to values of CK-MB in the clinical identification of patients. This cutoff, known as the receiver operating characteristic (ROC) curve–derived cutoff value, considered CK-MB the standard. However, this cutoff did not take advantage of the increased analytical sensitivity of cTn values. A second cutoff was recommended for use at a lower level, the 97.5th percentile of a normal patient population, from subjects who were poorly clinically defined, above which patients were considered to have cardiac injury. But even patients with a classic history of AMI were designated as having “unstable angina with minimal myocardial necrosis.” The guidelines followed extensive research demonstrating large numbers of patients with chest pain (roughly an additional 33%) whose prognoses in terms of subsequent frequency and timing of events were identical, and who had increased cTn values but normal CK-MB values. These findings were documented despite the fact that the initial version of cTn assays was relatively insensitive compared with contemporary assays.
This concept of using prognosis to confirm diagnosis rapidly became the paradigm not only for cTn but for the validation of most other markers as well. It was not until 1999, when a task force empaneled by the ESC/ACC took issue with these guidelines, that the concept of using only one cutoff value was initiated. ESC/ACC guidelines suggested the use, not of the 97.5th percentile of a reference population but the 99th percentile, in recognition of increased sensitivity of cTn that led to many elevations that were difficult to explain. This had the potential benefit of reducing the overlap to 1% between those with disease and normal individuals. It was conceptually important because even by this time, it was clear that enhanced sensitivity of cTn was leading to the identification of a substantial number of patients in whom the pathophysiologic cause of cardiac injury (see later sections) could not be determined. This is often the case when one moves from a relatively insensitive measure to one that has substantially greater sensitivity (i.e., when one uncovers new diagnostically and prognostically important increases). Nonetheless, clinicians had difficulty understanding this because such elevations had not been described previously and the pathophysiology was obscure. This problem has been revisited today as hs-cTn assays become increasingly sensitive and replace contemporary cTn assays. The ESC/ACC biochemical group at that time also recommended that the 99th percentile should be measurable with excellent imprecision and suggested, not mandated, a criterion of a total 10% CV or less at the 99th percentile. The group did not, however, recommend that if assays did not reach that level of precision, the decision values should be raised above the 99th percentile value. Unfortunately, this was the extrapolation of some, and it led to even greater heterogeneity in how cTn values were interpreted.
Some individuals persisted in using the NACB recommendations, some used the ESC/ACC recommendations, and some because of fear of false-positive results caused by imprecision employed a value higher than the 99th percentile, usually at the level of the 10% CV value. Add to this the fact that local laboratories often felt the need (appropriately) to validate the assays in their own hands and come up with different values, and one can see how the use of cTn values became fragmented and idiosyncratic. This problem also led to tremendous heterogeneity in the published literature and confusion on the part of clinicians.
It is now very clear that normal hs-cTn values are substantially lower than concentrations that are being reported for healthy individuals by contemporary assays. The reported concentrations in healthy individuals often represent “noise” (<LOD) in the contemporary assays. hs-cTn assays are growing worldwide, including in the United States, to have the ability to measure healthy individuals’ low concentrations accurately. For the past 2 years, the IFCC C-CB has posted and revised quarterly updates provided by manufacturers, current hs-cTn assays, along with POC and contemporary assays. A wealth of clinical information has made it clear that for contemporary assays, the 99th percentile value is the key value to use when measuring cardiac cTn. , Any value above the 99th percentile should be considered abnormal, indicative of myocardial injury. Concerns about false-positive results induced by such criteria should be minimal because assuming adequate quality assurance of the assays, even reduced imprecision should not lead to false-positive results provided cTn is measured in two serial samples. Usually reduced imprecision simply impairs the sensitivity of the assay. Statistical modeling of this issue suggests that the clinical impact of using even an imprecise assay is negligible with regard to false-positive results.
For this reason, along with the clinical data, the criteria in all guideline papers now include use of the 99th percentile, revised in 2018 from an overall URL to the use of individual, sex-specific 99th percentile URLs for males and females. Although some studies have suggested a return to the use of the 97.5th percentile value for high-sensitivity cTn assays, this is unlikely to occur unless important clinical reasons for such a change can be demonstrated. , , Once one recognizes that the 99th percentile is the only criterion for abnormality, one can progress to understanding how to use hs-cTn assays with sex-specific URLs in a variety of clinical situations for early rule out, early rule in, and risk assessment. Numerous publications have clearly demonstrated this point, which will be discussed in the following section.
AMI is a state characterized by abnormalities between nutrient perfusion and myocardial oxygen consumption. It is usually diagnosed when abnormalities in coronary flow at least in part contribute to the pathogenesis of cardiac injury. Because of the high sensitivity and specificity of cTn for the heart, cTn has become the cornerstone of the diagnosis of MI (see Boxes 48.2 and 48.3 ). As shown in Fig. 48.16 high-sensitivity cTn assays eliminate the noise of contemporary (and POC) assays, providing greater reliability of true measurement of cTn at the 99th percentile upper reference interval, and is now the standard assay of use in all clinical and research laboratories if available. An increased concentration of cTn greater than the 99th percentile URL is required in the appropriate clinical setting along with a rising or falling pattern for the diagnosis of AMI. With the growing use of high-sensitivity assays, earlier and more accurate diagnoses for ruling in and ruling out MI are being made within 1 to 3 hours of first blood draw compared to contemporary and POC assays. At A Glace 3 shows schematics of representative strategies to consider for early rule in and rule out based on implementation of hs-cTnI testing. Specifics of the MI definition are as follows.
 concentrations in two patients measured by a contemporary and a high-sensitivity cTnI (hs-cTnI) (with sex-specific cutoffs) assay demonstrating analytical “noise” of the contemporary assay.")
The clinical substrate (usually risk factors for AMI in the patient) is key. An increased cTn value is not synonymous with the diagnosis of MI. First, risk factors and the presentation (most often chest discomfort) must be compatible with the diagnosis. At times, imaging, whether performed at the time of intervention by angiography or thereafter, may provide proof of the substrate. , , , Many clinical situations can mimic AMI, the most common of which is myocarditis. Apical ballooning is another. Because of the increased sensitivity of cTn, clinicians need to be astute to the possibility that a given elevation in cTn, even with a rising pattern suggesting that it is acute, may not be due to ischemic heart disease (see Box 48.1 ). In addition, many groups such as women, the elderly, and diabetics can present atypically so interdigitating the biomarker information with the clinical is essential. This is conceptually difficult for some clinicians because when CK-MB, which was reasonably insensitive, was used, most substantive elevations were associated with coronary heart disease, albeit not all.
Acute events leading to cardiac injury (see Box 48.1 ) usually will manifest a changing pattern of values. , The rationale for this is that as assays have become more analytically sensitive, it has become clear that elevations of cTn can exist chronically. , The most overt case of this is seen in patients with renal failure. This is also the pattern manifest when artifactual increases occur as the result of analytical problems caused by interferences from human anti-mouse antibodies and heterophilic antibodies in the blood of some patients. , However, hs-cTn assays do not appear prone to as many analytical problems as early generations of assays. Nevertheless, a list of assay interferences involving hemolysis and biotin as potential interferents that are assay dependent is available on the IFCC C-CB website. Although patients with chronic elevations (not those with artifactual causes) are at long-term high risk, they are not necessarily at high risk over the short term. For this reason, the guidelines groups have advocated the need for a rising pattern of cTn values in patients who present early after the onset of symptoms, because such increases usually are indicative of an acute process. However, the acute process may not be AMI. Whether AMI is present is a clinical decision. When cTn values are not rising, one might seriously question whether acute disease of any kind is present or whether the elevations are of a more chronic nature. Care is necessary to ensure that one does not miss individuals who come in late after the onset of symptoms, whose cTn values may be near peak values, or whose values are on the long persistent tail of the time-concentration curve. They may appear not to have a changing pattern of values because they are near the peak (that can range from 12 to 48 hours) of the time-concentration curve or on the gradual downslope. This may occur in greater than 20% of patients.
With hs assays, there will be more AMIs that are not due to plaque rupture (so called supply-demand type 2 AMI, which has its own ICD-10 code) because these usually elaborate less cTn than plaque rupture events (type 1 AMI). , However, the criteria for a rising and/or falling pattern do not differ. These will occur more frequently in women than in men. There are good data that the use of sex-specific cutoff values with hs-cTnI assays (limited data for hs-cTnT assays) improve the diagnosis of these patients. While switching from a contemporary cTnT (fourth generation) to the hs-cTnT or Gen 5 cTnT assays is associated with an increased number of patients with the diagnosis of MI, this is not the case for replacing a contemporary to a hs-cTnI assay, as shown in Fig. 48.17 .

The guidelines distinguish five types of MI (see Box 48.3 ); two will be considered here because they both manifest with chest discomfort and increased biomarkers. One (type 1 MI) is the so-called spontaneous, or “wild type,” in which acute plaque rupture leads to some degree of thrombosis, or an episode in which platelet accretion occurs on a plaque, leading to thrombosis. , The second type (type 2 MI) includes coronary abnormalities with possible supply-demand imbalance, vasospasm, or endothelial dysfunction, which provides evidence of myocardial injury. ,
Individuals with spontaneous AMI can have STEMI or non-STEMI as indicated by the ECG pattern they manifest. , , Data indicate that immediate treatment aimed at opening the occluded artery is mandatory for patients with STEMI. This should be done based on the ECG pattern alone, even before biomarker values become available to assist with diagnosis. Opening of the artery is currently done with primary PCI and/or thrombolytic agents. The former is preferred when the two are available in similar time frames. With prompt coronary recanalization, the amount of myocardium lost is minimized and mortality is reduced. It should be noted that coronary recanalization increases the rapidity of biomarker release, and thus the rate of rise of the time-concentration curve is increased and the time to peak values is shortened.
A non-STEMI is less often associated with total coronary occlusion and usually is identified by ECG changes, which show not ST segment elevation but rather ST segment depression or T-wave changes. Given the sensitivity of hs-cTn for this diagnosis, the ECG is even at times totally normal. Patients who present with chest pain as a result of CAD should have risk factors, an appropriate presentation, or imaging evidence of this syndrome. Patients with an increased cTn, and the recommended 99th percentile URL are known to have more severe coronary heart disease than individuals without increased cTns. Likely for this reason they also have more procoagulant activity. Multiple intervention studies have shown that these patients benefit from aggressive anticoagulation, including heparin (the data for low-molecular-weight heparin are much stronger than the data for unfractionated heparin), glycoprotein IIb/IIIa antiplatelet agents, and an early invasive strategy consisting of PCI or coronary artery bypass grafting (CABG). Use of these strategies in patients without increased cTn values has been shown to be of no benefit and, in some trials, has actually proved detrimental. For these patients, expeditious but not necessarily immediate coronary interventions are suggested. Studies using hs-cTn assays have demonstrated that within the sex-specific reference interval for hs-cTn assays ( Fig. 48.18 A and B) as has been documented for patients above the 99th percentiles Fig. 48.19 , increasing levels of risk are associated with increasing cTn concentrations. However, given the increased frequency of type 2 MIs, it is unclear that invasive intervention will be necessary in all such patients. However, it is now well documented that among patients presenting to the EDs with an increased cTn, those with type 2 MI and myocardial injury from non-MI pathophysiology are at greater risk of adverse outcomes compared to type 1 MIs ( Fig. 48.20 ). Importantly, although patients with nonSTEMI who have an increased cTn value benefit from an invasive strategy, those who do not, as a group, do worse. ,
 for men (A) and women (B).")
 in women and men with suspected acute coronary syndrome. Outcomes are shown for women and men with no MI (solid line) and with MI (dashed red line), in which both assays were concordant, and for those reclassified as having MI using the high-sensitivity assay with sex-specific thresholds (dashed pink line).")

Not all patients have easily identifiable culprit lesions in which to intervene, and this explains some apparent spontaneous AMIs without severe CAD. , , , These patients, often women, may have endothelial dysfunction, coronary vasospasm, coronary dissection, or some other transient process that has resolved before investigation. These patients have type 2 MI according to the guidelines. This group might also include those individuals who have fixed but stable CAD but have some degree of damage as a result of excessive myocardial oxygen consumption, such as that caused by severe tachycardia, hypotension, or hypertension. Coronary arteries that are diseased tend to vasoconstrict rather than dilating in response to stimuli that would normally evoke vasodilation and increases in coronary flow. These patients are probably fundamentally different from individuals who have spontaneous MIs and likely are not a subgroup that has nearly as much procoagulant activity; it is unclear whether they benefit from interventional therapy. This may be one of the reasons why women who tend to have more severe endothelial dysfunction seem to have a different profile. , Nonetheless, depending on the specific study reviewed, 10 to 30% of patients may not have an identifiable lesion that has caused the event, leading to consideration of this alternative pathophysiology. From the perspective of diagnosis, however, the cTn criteria are identical.
Distinctions among the MI types have to be made on the basis of clinical characteristics and other diagnostic studies. It is now clear that women can have type 2 MI secondary to spontaneous coronary dissection. It used to be thought that this occurred almost exclusively during pregnancy, but that is clearly not the case. This diagnosis can be easily missed angiographically and is associated in at least half of patients with coronary tortuosity and evidence of fibromuscular dysplasia in other vascular beds. Preliminary data suggest that unless these patients are hemodynamically compromised or have total coronary occlusion, a strategy of watchful waiting rather than intervention may be preferred.
Other types of MIs are recognized. First, one type does not use biomarkers at all. This includes patients who may present classically with both chest pain and ECG changes but succumb either before blood tests can be obtained or before enough time has elapsed for the circulating concentration of cTn to exceed the 99th percentile. Two other types of MIs have been designated; these are related to PCI and CABG and will be covered later under “Special Situations.”
This can be a challenging area but has been substantially resolved with early measurements using hs-cTn assays that eliminate small changes in values due to analytical causes. In general, two values are different if they differ by more than 2.77 standard deviations (SDs) (assuming the variances are comparable at the two concentrations). Ideally, both analytical and biological variation would be included in calculation of the SDs. , Unfortunately, analysis of biological variation requires studies of stable subjects, and only hs-cTn assays can provide data on healthy people. Most analysis has focused on the use of data on analytical (total) imprecision alone. At high concentrations greater than 99th percentiles of cTns, the CV are 5 to 7%, so a difference of 20% is unlikely to be attributable to measurement imprecision. But as values begin to approach the low concentrations between the LOD and the 99th percentile, analytical %CV increases with contemporary assays, making the relative difference between two consecutive values prone to increases by random error alone. Local analysis of imprecision should be used to guide interpretation of differences in results for consecutive samples, with larger percentage changes necessary to suggest real change at very low levels of cTn. Defining a consistent period for analysis is also key to an accurate approach to this analysis. High-sensitivity assays improve this problem; their excellent imprecision at low cTn concentrations (10 to 20% CV at or above the LOD) make it possible to calculate a reference change value (RCV). , , , hs-cTn assays show RCV values (biological variation) ranging from 50 to 85% (as shown in Tables 48.2 and 48.3 ). , Although it is now clear that these values may work well when the baseline value is near the 99th percentile URL, when the baseline value is elevated, these values are less sensitive. Accordingly, for example, a recommendation (expert opinion) has been made for hs-cTnT to use a 50% change near the 99th percentile upper reference interval and a 20% change when the baseline value is elevated. Similar percent change recommendations are now available for hs-cTnI assays, but can differ by assay as they are not standardized, as it appears different studies for different hs-assays may use different percent changes. Others have advocated for the use of absolute concentration change criteria if examining changes within the reference limits. In general, these are similar to percentage criteria when baseline values are near the 99th percentile URL but are much lower when the baseline values are elevated. It appears that these values provide better accuracy, especially when the baseline value is elevated, compared to percent criteria. , , What is known is that individual hs-cTn assays will need to develop their own change values because there will not be a universal value that will be applicable to all hs-cTnI assays. Early clinical studies in this area often used convenience cohorts that may have had incomplete sample sets, used insensitive gold standards, and lacked early patients.
| Abbott | Beckman | Roche (E170) | Siemens | Singulex | |
|---|---|---|---|---|---|
| CV A (%) | 13.8 | 14.5 | 7.8 | 13.0 | 8.3 |
| CV I (%) | 15.2 | 6.1 | 15.0 | 12.9 | 9.7 |
| CV G (%) | 70.5 | 34.8 | NA | 12.3 | 57 |
| Index of individuality | 0.22 | 0.46 | NA | 0.11 | 0.21 |
| RCV (%) | NA | NA | 47.0 | NA | NA |
| RCV increase (%) | 69.3 | 63.8 | NA | 57.5 | 46.0 |
| RCV decrease (%) | −40.9 | −38.9 | NA | −36.5 | −32. |
| Within-subject mean (ng/L) | 3.5 | 4.9 | NA | 5.5 | 2.8 |
| LOD (1.9 ng/L) | High-STEACS (<5 ng/L) | |||
|---|---|---|---|---|
| Parameter | Baseline hs-cTnI < LOD | Baseline hs-cTnI< LOD and Normal ECG | Baseline hs-cTnI <5 ng/L | Baseline hs-cTnI <5 ng/L and Normal ECG |
| Acute Myocardial Infarction | ||||
| Proportion qualifying | 444/1631 (27) | 254/1631 (16) | 812/1631 (50) | 406/1631 (25) |
| Proportion of missed MIs | 2/170 (1.2) | 1/170 (0.6) | 9/170 (5.3) | 2/170 (1.2) |
| NPV | 99.6 (98.9–100) | 99.6 (98.8–100) | 98.9 (98.2–99.6) | 99.5 (98.8–100) |
| Sensitivity | 98.8 (97.2–100) | 99.4 (98.3–100) | 94.7 (91.3–98.1) | 98.8 (97.2–100) |
| PPV | 14.2 (12.2–16.1) | 12.3 (10.5–14.0) | 19.7 (16.9–22.4) | 13.7 (11.8–15.6) |
| Specificity | 30.3 (27.9–32.6) | 17.3 (15.4–19.3) | 55.0 (52.4–57.5) | 27.7 (25.4–30.0) |
| Type 1 Myocardial Infarction | ||||
| Proportion qualifying | 443/1529 (29) | 254/1529 (17) | 807/1529 (53) | 405/1529 (27) |
| Proportion of missed MIs | 1/68 (1.5) | 1/68 (1.5) | 4/68 (5.9) | 1/68 (1.5) |
| NPV | 99.8 (99.3–100) | 99.6 (98.8–100) | 99.5 (99.0–100) | 99.8 (99.3–100) |
| Sensitivity | 98.5 (95.7–100) | 98.5 (95.7–100) | 94.1 (88.5–99.7) | 98.5 (95.7–100) |
| PPV | 6.2 (4.7–7.6) | 5.3 (4.0–6.5) | 8.9 (6.8–10.9) | 6.0 (4.6–7.3) |
| Specificity | 30.3 (27.9–32.6) | 17.3 (15.4–19.3) | 5.5 (5.2–5.8) | 27.7 (25.4–30.0) |
| Type 2 Myocardial Infarction | ||||
| Proportion qualifying | 443/1563 (28) | 253/1563 (16) | 808/1563 (52) | 405/1563 (26) |
| Proportion of missed MIs | 1/102 (0.98) | 0/102 (0) | 5/102 (4.9) | 1/102 (0.98) |
| NPV | 99.8 (99.3–100) | 100 (100–100) | 99.4 (98.8–99.9) | 99.8 (99.3–100) |
| Sensitivity | 99.0 (97.1–100) | 100 (100–100) | 95.1 (90.9–99.3) | 99.0 (97.1–100) |
| PPV | 9.0 (7.3–10.7) | 7.8 (6.3–9.2) | 12.9 (10.5–15.2) | 8.7 (7.1–10.4) |
| Specificity | 30.3 (27.8–32.6) | 17.3 (15.4–19.3) | 55.0 (52.4–57.5) | 27.7 (25.4–30.0) |
It has long been appreciated that interventions done on the coronary arteries can result in the release from heart muscle of biomarkers indicative of cardiac injury. , For this reason, a variety of criteria have been promulgated, starting years ago with CK-MB. It was shown initially that elevations of CK-MB that occurred after the procedure were highly predictive of adverse events over the long term. These findings were difficult to explain because the amount of injury involved often was very minor but was nonetheless easy to document with sophisticated techniques such as cardiac magnetic resonance imaging (cMRI). However, controversy about the mechanisms continued and a large number are being hypothesized. The advent of cTn biomarkers has rendered this issue far less complex. Patients who have elevations of circulating cTn and who present with acute coronary problems have much more severe abnormalities in coronary anatomy than those who do not have cTn elevations. In recent studies, the baseline cTn value has been added to the analysis of these post-PCI elevations. , This was done for many years, but not with assays that measured cTn concentrations even close to the 99th percentile. Accordingly, it is only recently that the data have confirmed several important conceptual issues.
The first concept is that a vast majority of patients with significant elevations (threefold to fivefold increase in CK-MB or cTn) that in the past were associated with an adverse prognosis are those with increased cTn values at baseline. This usually (although not always) is indicative of an acute presentation and therefore a rising pattern of values. In the setting with a rising pattern of values, it is hard to know whether one should attribute the increases to the PCI or to the initial insult. Nonetheless, when one incorporates the baseline value into the analysis, most of the prognostic significance of the post procedure cTn values is ablated. Data suggest that it is only at an elevation of cTn at baseline that marked post-procedure elevations in cTn are apt to be frequently found, suggesting that in most instances at least a blend of the two processes occurs. These issues have been confounded not only by failure to use appropriate cutoffs for cTn, but by the use of insensitive cTn assays. More recent guidelines clarify this circumstance substantially by indicating that if one has an increased cTn at baseline before PCI, the diagnosis of post-PCI injury is confounded and cannot be made. Thus a normal baseline cTn is required in almost all instances to identify procedure-related myocardial injury. If the baseline cTn is increased, subsequent increases may or may not be able to be attributable to the procedure itself and a diagnosis of post-PCI injury cannot be made with absolute confidence.
Marked elevations, as indicated previously, are uncommon but can occur. When they do occur, they are rarely of cardiovascular importance, in the sense that the more marked elevations are easily presaged by clinical information at the time of the procedure. Thus post-PCI cTn values add very little that is new. In addition, it is unclear whether patients have an adverse cardiovascular prognosis over time. In the most recent analysis done by using the most appropriate cutoff values and contemporary cTn assays, borderline statistical significance was attributed to post-PCI elevations. However, most events that did occur were noted during procedures in patients who had severe underlying noncardiac comorbidities and therefore underwent palliative procedures. The event rate, if patients with non–cardiac-related subsequent complications are excluded, would not have been of statistical importance, even if their inclusion were of only borderline significance. Thus it now appears that collection of this information after PCI is not necessary. Recent data suggest that values even modestly below the 99th percentile upper reference interval have important prognostic significance, presaging in our opinion the likelihood that with hs-cTn assays, this effect will be strengthened and the prognostic impact of post-PCI values attenuated still further.
Nonetheless, criteria still exist for these occasional patients who may have post-PCI injury. The appropriate cutoff cTn value is unclear, but it is clear that very few patients will reach the marked fivefold elevation previously advocated if the baseline cTn is not increased. , This is likely to change, however, with hs-cTn assays. If cTn is increased post-PCI more than fivefold, with a normal baseline cTn value assumed, the patient can be diagnosed as having had a periprocedural MI if they have had symptoms or have ECG changes and/or had complications of the procedure. No specific therapy is mandated. Regarding biomarker changes that occur after reperfusion of an occluded vessel after PCI or thrombolytic therapy in AMI patients, greater than twofold increases in biomarkers occur within 90 minutes of reperfusion, the rate of increase of biomarkers within the first 4 hours separates reperfused from nonreperfused patients, and after myocardial reperfusion in AMI patients, washouts of all biomarkers parallel each other. However, increased washout does not define the level of reperfusion and cannot be used to define a post-PCI AMI.
One unique subset needs to be considered, and that is the small group of patients who may have chronic preprocedural elevations in cTn. These individuals will manifest a rising pattern, albeit from an increased baseline, when they have events, including post-PCI events. Accordingly, what has been suggested is that the criteria used for reinfarction of an increased value of 20% or more should be used to define post-PCI infarction in this group.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here