Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

 Access video content for this chapter online at Elsevier eBooks+
Access video content for this chapter online at Elsevier eBooks+
The goal of breast reconstruction is to give patients the opportunity to move beyond breast cancer and mastectomy by creating symmetric and naturally appearing breasts. One method of reconstruction that has been utilized for decades is the transverse rectus abdominis myocutaneous (TRAM) flap. This method of reconstruction, when utilized as a pedicled flap, is based on the superior epigastric system, in contrast to a free TRAM flap, which is based on the inferior epigastric system. The muscular make-up of the abdominal wall provides the opportunity to utilize the rectus abdominis in breast reconstruction with acceptable postoperative strength loss that allows patients to resume all activities of daily living. Reconstruction of the abdominal wall is a key portion of the operation and is critical to minimizing potential postoperative complications. Our goals in this chapter are to describe the history and anatomic details of the TRAM flap, its common usage, intraoperative details, methods of minimizing postoperative complications, as well as address variations and different iterations of the TRAM flap.
Since the first attempt at breast reconstruction by Czerny in 1893, surgeons have endeavored to find the best method of reconstruction following radical mastectomies with different methods being utilized over the decades. The first TRAM flap was performed in 1980 after significant work by Carl Hartrampf. His original TRAM flap design was based on the upper abdominal skin and fat with a resultant mid-abdominal scar. This eventually evolved into a lower abdominal TRAM that utilized the lower abdominal skin and fat, resulting in a low transverse scar. Further modifications included a delay procedure that involved ligation of the deep inferior epigastric vessels to augment the perfusion from the superior system. The TRAM flap provided an alternative to other methods of reconstruction, such as the latissimus dorsi flap, which frequently had to be augmented with implants to reach a desired size. Often, there are chest wall defects that require a greater amount of tissue than can be provided with other methods of reconstruction. Over the years, depending on reconstructive needs, the TRAM flap has undergone several variations, which will be covered later in this chapter.
The rectus abdominis is a type III muscle according to the Mathes and Nahai classification scheme and is based on both the superior and inferior epigastric system with minor contributions from the 7th–12th intercostal perforators. The superior epigastric vessels originate from the internal thoracic (mammary) artery and vein and proceed deep to the rectus abdominis muscle, eventually anastomosing with the deep inferior epigastric vessels in the periumbilical area. Perforators to the overlying skin lie medial to the linea semilunaris and can be found along the course of the vascular pedicle, most concentrated around the periumbilical region. When used for breast reconstruction as a pedicled transverse rectus abdominis myocutaneous flap, the principal blood supply is the superior epigastric system which differs from a free TRAM and deep inferior epigastric perforator (DIEP) flap as that is based off the inferior epigastric system. According to Moon and Taylor, the inferior epigastric vessels can be classified by their path and form as follows: type I pattern is a single intramuscular vessel, type II pattern is a dual branching pattern of the inferior epigastric artery at the level of the arcuate line, and type III is an inferior epigastric artery that branches into three vessels as it travels above the arcuate line to connect to the superior epigastric system. These branching patterns can vary between patients as well as from one rectus to the contralateral side in the same patient. Motor innervation is from the T8–T12 intercostals. When considering the contribution to the relative perfusion of the lower abdomen from the superior versus the inferior epigastric system, there is no dispute that the inferior epigastric system, due to its size and proximity of take-off from parent vessels, is dominant, but our experience has shown that superiorly based flaps can also be safely and expeditiously used in breast and chest wall reconstruction.
The blood supply to the inferior abdominal tissue, when taken as a pedicled TRAM flap, can be broken down into four different zones of perfusion when considering a unilateral TRAM flap versus two zones in bilateral TRAM flaps ( Fig. 28.1 ). Zone I lies directly over the muscle while zone II lies immediately across midline. Zone III is ipsilateral to the zone directly overlying the muscle and zone IV is the most lateral contralateral zone. Initially, it was thought that the perfusion of zone II was superior to zone III, but experience and perfusion studies have shown that zone III has similar if not more reliable vascularity. When performing a unilateral breast reconstruction, many surgeons prefer to utilize zone I and adjacent parts of zones II and III and discard zone IV since it has the poorest blood supply. In unilateral breast reconstruction, the surgeon has the option of utilizing an ipsilateral or contralateral pedicled TRAM flap. Although both can result in a satisfactory outcome, the authors prefer to transfer an ipsilateral TRAM versus a contralateral TRAM when possible, as an ipsilateral TRAM will place the better perfused zone III versus zone II in a superior position. Additionally, an ipsilateral TRAM provides a longer pedicle length allowing for greater mobilization of movement and inset while producing less of a bulge in the epigastrium than a contralateral flap.
 of right-sided TRAM flap.")
It is often said that the most important aspect of an operation is the preoperative planning, primarily the preoperative and intraoperative markings. Patients undergoing a TRAM flap reconstruction should have the following markings done in the preoperative area:
A midline drawn from the sternal notch down to and past the umbilicus, delineating the central portion of the chest and abdomen.
Bilateral inframammary fold (IMFs) as well as a tangent line extending to the midline.
A line marking the superior aspect of the breast tissue in line with the peak of the axilla.
Marking the planned mastectomy incisions.
At this point, if planned, the “Bikini Inset” can be marked. This design and marking will be described and demonstrated later in this chapter.
Intraoperative markings of the flap are determined by the extent of the mastectomy defect and volume of tissue required, as well as an assessment of the expendable lower abdominal tissue that can be harvested to allow safe abdominal closure. The intraoperative markings consist of:
Superior abdominal incision is usually 2–4 cm above the umbilicus to make sure the periumbilical perforators are incorporated.
Inferior abdominal incision placed 6–7 cm above the introitus.
When a unilateral TRAM flap is to be done, the flap mainly constitutes zone 1 and proximal parts of zone 3 and 2; a bilateral TRAM will incorporate zones 1and proximal part of 3 ( Fig. 28.2 ).
 Preoperative picture. (B) Intraoperative markings for a bilateral TRAM flap. (C) 10-month postoperative result.")
The TRAM flap can repair many defects involving not only breast reconstruction but also chest wall and sternal defects. When used in breast reconstruction, the TRAM flap can be utilized for immediate reconstruction at the time of the mastectomy or in a delayed fashion to create a natural, ptotic breast. Delayed breast reconstruction is often in the setting of prior radiation and following mastectomy. Radiation is unpredictable and is recommended to be performed prior to the final TRAM flap reconstruction as it has been shown to be detrimental to not only the aesthetic outcome and shape of the flap but also cause contracture and pigmentation changes if performed after the flap reconstruction. Therefore, the authors approach is to perform flap reconstruction 6–9 months after the completion of radiation therapy with preoperative evaluation and assessment performed in clinic around 6 months after completion of radiation.
As with any method of reconstruction, both advantages and disadvantages of the TRAM flap must be considered as part of the patient selection process and preoperative planning. Not only can the TRAM flap provide enough tissue for large reconstructions, but it also provides an added benefit of removal of excess abdominal tissue similar to that of an abdominoplasty. Due to the large amount of tissue that can be transferred with the TRAM flap, total autologous reconstruction is often obtained without the need for implants. If the patient is able to undergo a skin and nipple-sparing mastectomy, bilateral TRAM flaps can also be utilized in a complete buried and de-epithelialized fashion to provide an adequate and overall symmetric result ( Fig. 28.3 ). An often-cited disadvantage of a pedicled flap reconstruction utilizing the rectus abdominis muscle is a possible weakening of the abdominal wall and resultant abdominal wall herniation. By meticulous closure of the abdominal wall, which will be discussed later in this chapter, this perceived disadvantage may be minimized. In addition, the blood supply for a pedicled TRAM flap can be augmented by a delay procedure, which will also be discussed later in this chapter.
 Preoperative photo. (B) Intraoperative markings with planned mastectomies through an inframammary fold incision. (C) 3-year postoperative result.")
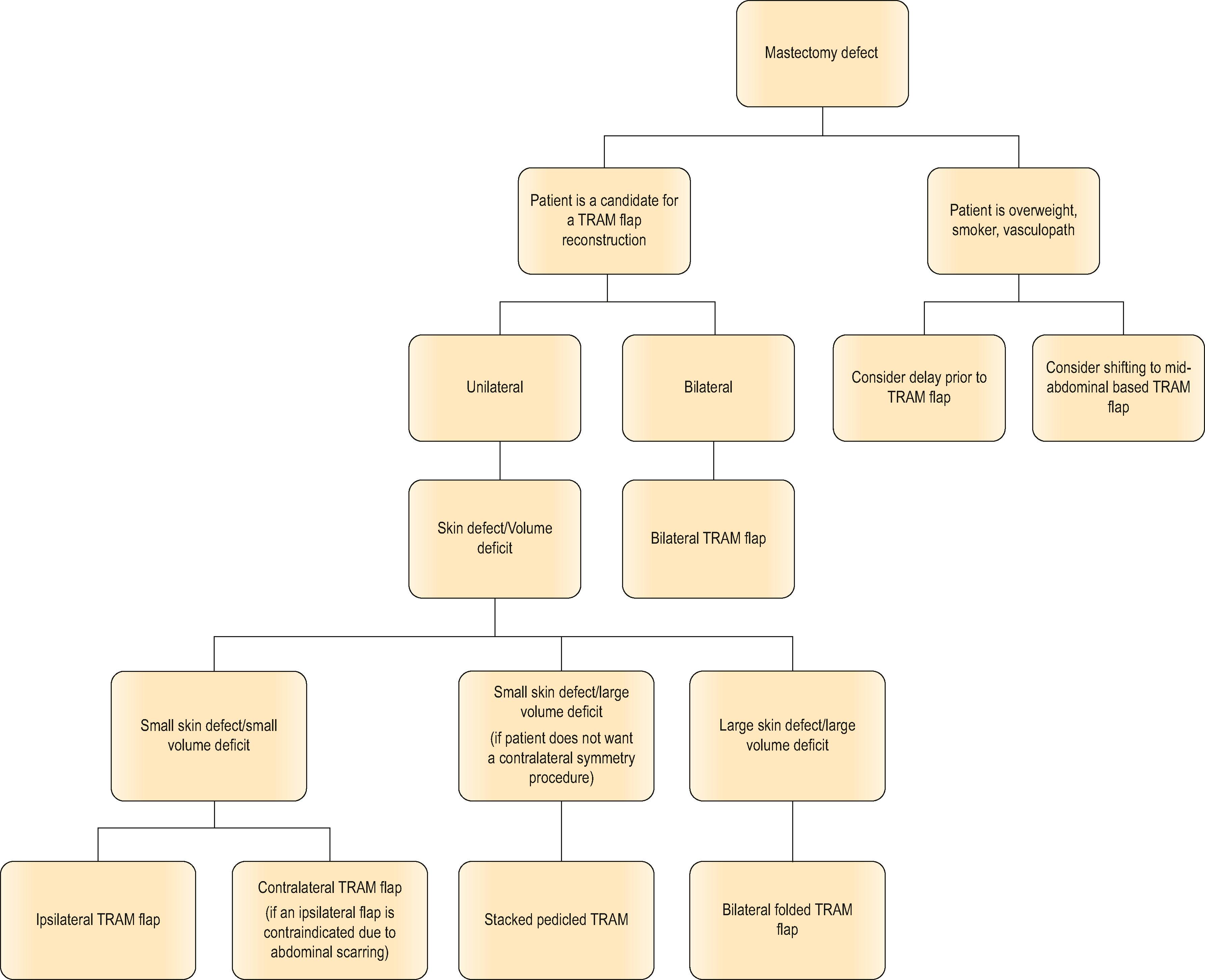
As previously stated, the primary purpose of breast reconstruction is to create a naturally looking breast to facilitate the recovery and healing process and to help them look and feel as natural as possible. As with any surgical procedure, initial patient assessment is important to determine which patients would best benefit from the procedure ( Algorithm 28.1 ). Specifically, for breast reconstruction, preoperative considerations include breast size, shape, desired breast size, patient goals, expectations, and desires. In assessing the state of the patient’s breast cancer treatment, additional considerations include whether to perform a unilateral ( Fig. 28.4 ) or bilateral ( Fig. 28.5 ) reconstruction in an immediate or delayed fashion as well as whether the patient will be undergoing chemotherapy or radiation as part of their treatment algorithm. Another important aspect is the patient’s abdominal exam, whether there has been any prior abdominal operations, and if there is sufficient abdominal tissue to form an adequately sized proportional breast.
 Intraoperative markings. (B) 9-month postoperative result.")
 Intraoperative markings. (B) Patient result 2 weeks after her nipple reconstruction, 11 months after her original reconstruction.")
Patients not considered as appropriate candidates for this operation are those with significant medical co-morbidities, psychiatric disorders, considerably overweight or obese, heavy tobacco users, as well as patients who have had significant prior abdominal operations such as an abdominoplasty or have a large subcostal incision from a prior open cholecystectomy. It is also not a recommended procedure for patients with uncontrolled back pain, fibromyalgia, or chronic pain syndromes due to the potential for aggravation of their pain postoperatively. Future childbirth is not an absolute contraindication as there are reports in the literature of patients becoming pregnant after having a TRAM flap and not experiencing an increase in abdominal wall complications.
The following section will describe the steps for both unilateral ( ) and bilateral ( ) breast reconstruction with the TRAM flap. As previously mentioned, the general breast markings are completed in the preoperative holding area with the actual TRAM flap markings done on the operating room table. For unilateral reconstructions, it may be necessary to extend the flap beyond the midline to obtain adequate volume and skin to facilitate reconstruction of the defect. At this point, it is imperative to assess the tissue needed for reconstruction of the skin defect created by the mastectomy as well as the mastectomy skin flaps for adequate perfusion. The mastectomy skin flaps can be cut back until healthy bleeding dermal tissue is observed or SPY technology may be used. The skin defect and required skin design can then be transferred to the abdominal tissue.
The TRAM flap elevation begins by incising around the umbilicus. Next, we prefer to de-epithelialize the part of the abdominal tissue that will eventually be buried under the mastectomy flaps while it still remains in situ on the abdomen and under a mild degree of tension. The upper abdominal flap is then elevated initially at the sub-Scarpa level for 4–5 cm and then at the fascial level, all the way up to the epigastrium, while beveling superiorly to capture as many perforators as possible. Dissection should also be limited laterally and should not be performed above the costal margin in order to maintain as many lateral perforators to the overlying abdominal tissue as possible. The lower abdominal incision is then made, and dissection is carried down to the abdominal wall. At this point, in a unilateral case, if the flap design extends across the midline into the medial part of zone 2, it is incised and dissected down to the abdominal wall and then dissected to the midline, 1–2 cm past the linea alba, preserving all ipsilateral perforators seen. The flap can then be elevated from lateral to medial until the linea semilunaris and lateral rectus sheath is reached.
Inferiorly, the skin flap is elevated off the fascia to the arcuate line (approximately midway between the pubis and umbilicus). The rectus sheath overlying the muscle is then incised transversely and dissected to the medial and lateral aspects of the muscle. The medial aspect of the fascia is now incised down to muscle all the way up to the epigastrium, and the medial edge of the rectus muscle is dissected free from the fascia. Next the lateral rectus sheath is incised down to the rectus muscle and, of note, there are two layers of this sheath inferiorly, which fuse into a single layer at a variable distance above the umbilicus. Again, the fascia is separated from the lateral border of the muscle, and multiple intercostal perforators are seen to be entering the undersurface of the muscle. These are cauterized and divided.
The muscle is then divided with electrocautery inferiorly at the level of the arcuate line and the inferior epigastric vessels are ligated and divided. The flap is then elevated in an inferior to superior fashion and developed as a superiorly based flap based on the superior epigastric vessels. There are multiple small perforators supplying the posterior sheath, which are best cauterized and divided to avoid them retracting into the muscle and bleeding. Once the superior vessels are identified, the lateral aspect of the muscle can be partially divided, as this assists with the rotation. With the flap completely elevated, the distal part of zone 3 is incised to check its vascularity and then discarded and thinned at the sub-Scarpa level, as this will be used to reconstruct the upper part of the breast.
At this point, the flap is allowed to sit in situ while the mastectomy pocket is prepared. With delayed reconstructions, the goal is to recreate the original breast defect; whereas, with immediate reconstruction, the pocket may need to be adjusted with suture plication if it has been over-dissected. We feel the best access point for flap transfer is medially as this provides a natural turn for the muscle and pedicle and does not violate the inframammary fold inferiorly. A medial tunnel is therefore created that connects with the abdominal dissection in the epigastrium, and it is made large enough to allow the flap to pass through.
When all is ready, to assist in transfer of the flap into the superior mastectomy pocket an arrow can be drawn pointing laterally toward zone 3. Zone 3 is then grasped and brought through into the breast pocket to be oriented superiorly, ensuring minimal pedicle twist. Therefore, a right TRAM flap is rotated clockwise and a left-sided TRAM flap is rotated counter-clockwise because the ipsilateral abdomen is being used. Utilizing an ipsilateral flap lessens the bulk crossing the epigastrium, as would be seen in a contralateral flap. The medial bulk of the flap transfer does diminish over time due to denervation-induced flap atrophy. A Blake drain is placed along the IMF and exists laterally and inferior to the fold. Another Blake drain can also be used in the axilla if a full axillary dissection was performed or if a significant axillary defect exists.
Flap inset varies depending on whether it was performed as an immediate or delayed reconstruction. With immediate reconstruction, it is not uncommon for the aesthetic boundaries of the breast to be violated and therefore they must be re-established, usually using quilting sutures. With delayed reconstruction, the mastectomy defect must be recreated and often a significant amount of scarred skin removed. The mastectomy skin flap quality can either be assessed with intraoperative fluorescent angiography or can be cut back to healthy bleeding skin edges. The flap itself is then inset with buried and running 3-0 monofilament absorbable sutures. Various inset techniques have been devised over the years and one type will be discussed later in this chapter.
At this point, the abdominal wall is repaired. Meticulous closure of the abdominal wall is important to minimize the risk of postoperative complications such as abdominal wall hernias or bulges. In addition, to maximize the function of the remaining abdominal wall muscles, it is key to restore the disinserted lateral abdominal muscles back to their normal resting tension, as described below and represented in the accompanying video which demonstrates closure of the abdominal wall in a bilateral TRAM flap operation ( ). In a unilateral based reconstruction, the contralateral side is first excised using cautery. We recommend utilizing a polypropylene mesh placed as an inlay into the defect created from the muscle harvest, with the width of the mesh approximating the width of the rectus muscle. The mesh stretches in only one direction and that is placed in a superior to inferior orientation to prevent bulging. In a unilateral case, the mesh is sutured in place to the linea alba medially and the conjoint fascia of the external and internal oblique fascia within the rectus sheath. We find that this suturing is best done with interrupted, buried polypropylene sutures first, and then supplemented with a running polypropylene suture used to advance the fascia over the mesh, burying approximately 30% of the mesh while ensuring appropriate tension is placed to restore the normal resting muscle tension. In bilateral cases, a larger piece of the mesh is used to span the abdominal wall and is secured to both lateral aspects of the rectus fascia as described above and is secured with buried interrupted polypropylene stitches to the linea alba as well to ensure there is no shift of the midline. A new hole in the mesh is made to accommodate the umbilicus.
Abdominal skin closure is performed by first flexing the patient at the hips to relieve tension on the abdominal closure. A narrow inferiorly based V-incision is made in the skin at the site of the new umbilical opening. Part of the abdominal fat in this area can be thinned and the umbilicus can then be brought through and sutured in place with a 2-0 buried braided absorbable suture as well as interrupted Monocryl sutures and, finally, a running 5-0 chromic suture. An incision is made at the inferior aspect of the umbilicus and the small V-shaped flap is inset into the defect to prevent umbilical contraction. Two drains are usually inserted into the abdomen, one directed superiorly and one inferiorly and are brought out through separate incisions laterally. The abdominal closure is temporarily approximated with staples and the authors’ preference is to close with interrupted 2-0 braided absorbable sutures and a running intracuticular 3-0 barbed absorbable suture.
Anatomic structures must be considered throughout the operation. It is important to preserve the abdominal wall integrity as much as possible including the linea alba and lateral fold of the rectus fascia including the linea semilunaris as well as the muscle and fascia below the arcuate line. The umbilicus with its deep vascular supply as well as perforators to the abdominal skin, which are not restricting TRAM flap movement, must also be preserved. The central and inframammary fold are also integral to maintaining a correct and aesthetic breast shape. When performing the flap, it is important to include the skin, subcutaneous tissue and muscle with as many periumbilical perforators as possible, as well as a strip of the fascia overlying the recuts muscle.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here