Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Blood is a specialized type of connective tissue that consists of cells suspended in a circulating fluid known as plasma. The total amount of circulating blood in men is 5-6 L; that in women, 4-5 L. Fresh blood is a red, viscous fluid, whereas plasma is translucent and yellow. Cellular elements of blood constitute about 45% of blood volume in adults, with plasma making up the other 55%. These elements include erythrocytes (or red blood cells ), granular and agranular leukocytes (or white blood cells ), and circulating cytoplasmic fragments known as platelets (or thrombocytes ). Plasma consists of plasma proteins, such as fibrinogens, globulins, and albumin, and a ground substance called serum. Bone marrow, a highly vascularized tissue in medullary cavities of bones, consists of both vascular and hematopoietic (blood-forming) compartments. Like most other connective tissue types, blood and bone marrow derive embryonically from mesoderm. In the first few weeks of gestation, blood islands in the yolk sac are the first sites of hematopoiesis, or production of blood cells. During the rest of fetal life until about 2 weeks after birth, blood cells form in the liver and spleen. In children and adults, bone marrow is the major site of hematopoiesis. Lymphocytes are also produced in lymphoid organs. Bone marrow is a large tissue and accounts for 4%-5% of body weight. Its total weight exceeds that of the liver and has been estimated at 1.6-3.7 kg in the adult.
A complete blood count (CBC) is a valuable screening test in medical practice that is used to diagnose and manage many conditions and diseases such as acute and chronic infections, allergies, and anemias. It measures the number of erythrocytes (RBCs) and leukocytes, total amount of blood hemoglobin, and fraction of blood composed of RBCs—the hematocrit. The CBC also includes other information about RBCs, such as mean corpuscular hemoglobin (MCH) and mean corpuscular hemoglobin concentration (MCHC), as well as the platelet count.
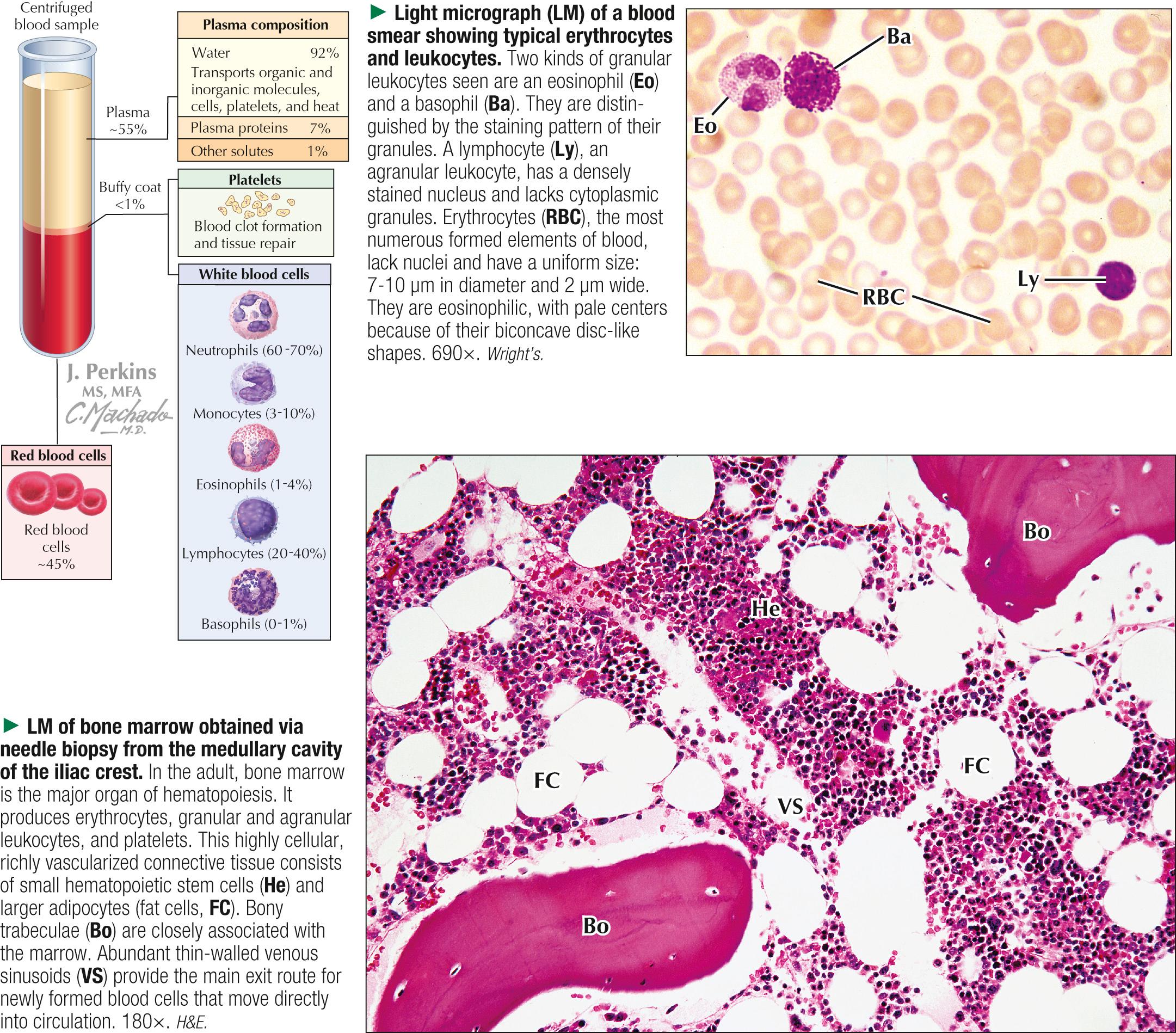
Blood cells can be studied via tissue sections, but a blood film or smear is preferred for routine microscopic evaluation. The procedure for a blood film involves placing a drop of blood on a glass slide, spreading it thinly and evenly over the surface with another slide on edge, and then air-drying and staining it. Rather than using a conventional hematoxylin and eosin (H&E) stain, special stains that utilize a combination of acid (eosin), basic (methylene blue), and neutral dyes better demonstrate the formed elements. Many blood stains are available, but Giemsa and Wright stains are superior for elucidating different blood cell types with an oil immersion objective lens. In blood films so stained, erythrocytes (RBCs) are typically orange-red to pink, and nuclei of leukocytes, with an affinity for basic dyes, stain blue. Various types of granules in granular leukocytes show different affinities for stains, and cells containing them are thus named eosinophils, basophils, or neutrophils. Determining RBC numbers, shapes, and sizes in blood smears provides useful data for diagnosis and treatment of many diseases such as microcytic and macrocytic anemias. Normal RBCs are usually uniform in size and shape, but poikilocytes —RBCs with distorted shapes—occur in certain conditions. Many pathologic conditions can alter the number of leukocytes. To determine relative proportions of leukocytes, a differential white blood count is obtained via a blood smear; normal values are listed in the table.
A valuable clinical test is the hematocrit. It is determined via centrifugation of a freshly drawn blood sample in a test tube with added anticoagulant (e.g., heparin). Three layers typically appear in the tube. The top layer of plasma constitutes about 55% of the column. A thin, white, middle layer—the buffy coat—consists of leukocytes and platelets and is only 1%. The hematocrit is represented by the lowest layer of packed red blood cells, normally about 45% of the volume. Significant changes in its value may be a sign of disease.

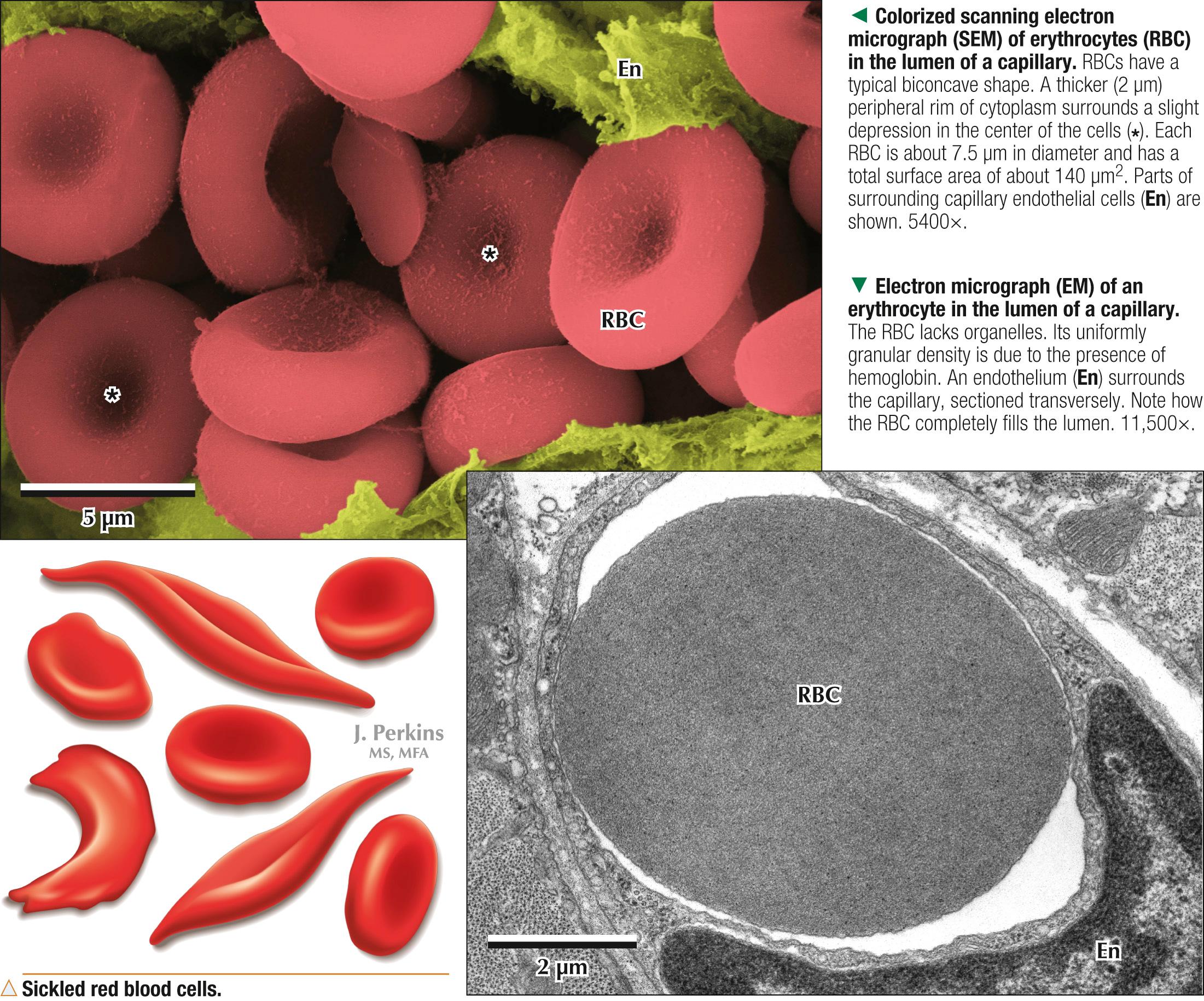
RBCs are anucleate biconcave discs that are highly flexible and malleable as they travel in narrow capillary lumina. They make up 99% of the formed elements of blood and have a lifespan in circulation of about 120 days. Numbers of RBCs per liter of blood usually average 5 × 10 12 in men and 4.5 × 10 12 in women. In the human embryo, RBCs are initially nucleated, up to 7 weeks of gestation. During final stages of erythropoietic development in bone marrow, RBCs lose the nucleus and almost all organelles except the cytoskeleton and then enter the circulation. Because RBCs lack a nucleus but have a plasma membrane, they are more aptly termed corpuscles than true cells. A sticky surface often causes RBCs to adhere to each other in circulating blood and form loose rows known as rouleaux. In standard blood smears, the RBC center is a pale area surrounded by a thicker, eosinophilic peripheral zone. A biconcave shape provides a large surface area for primary functions: transporting O 2 from lungs to tissues and returning CO 2 from tissues to lungs for elimination. The iron-containing protein hemoglobin in RBCs accounts for their red color. Hemoglobin rapidly binds to O 2 for transport. It is a conjugated protein containing the pigment heme and the protein globin. Heme is a porphyrin combined with iron. Normal values of hemoglobin in whole blood are about 14-18 g/dL for males and 12-16 g/dL for females. Several forms of inherited hemoglobin abnormalities, including anemias and thalassemia syndromes, occur in humans.
A deficiency of RBCs and/or hemoglobin is anemia, many different types of which exist. Correct diagnosis relies on calculating the RBC number in peripheral blood, determining hemoglobin concentration, and examining RBC morphology in blood smears. Sickle cell anemia is an autosomal recessive disorder leading to faulty synthesis of the β-globin chain of hemoglobin. Resulting hemoglobin S causes RBC deformities. Instead of biconcave discs, they become crescent-shaped sickle cells, which lose malleability and malfunction. Current treatment alleviates symptoms, but bone marrow transplants may provide a cure in some cases.
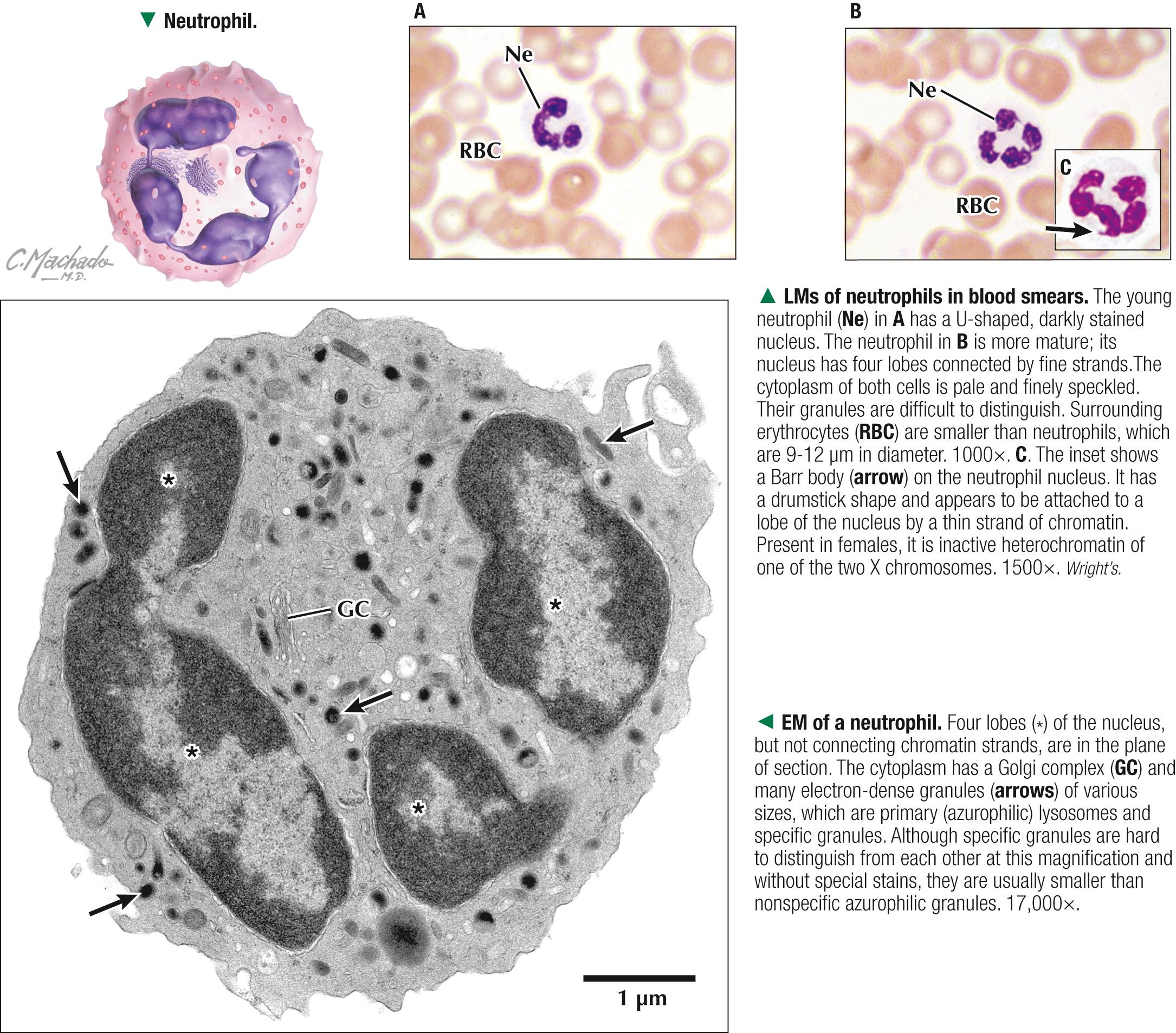
Neutrophils are the most numerous leukocytes and constitute 60%-70% of the leukocyte count. The nucleus has a distinctive morphology and many forms (thus the name polymorphonuclear leukocytes ), with a clump-like pattern and three to five lobes connected by fine chromatin strands. Immature neutrophils show only slight nuclear lobulation; older cells have more, dark-staining lobes. Females often have a small drumstick-shaped lobe—the Barr body. It is absent in males and may be useful in determining chromosomal sex. Neutrophil cytoplasm is lightly eosinophilic and, as in other granular leukocytes, contains two types of granules. Many small, membrane-bound specific granules are not acidophilic or basophilic but stain faintly with neutral dyes. Occasional large azurophilic granules that stain reddish purple are primary lysosomes containing peroxidase and hydrolytic enzymes. A small Golgi complex, a few scattered mitochondria, and some glycogen deposits are also in the cytoplasm. Like all other leukocytes, neutrophils are actively motile and function outside the circulation. After they develop in bone marrow, they stay in the bloodstream for 8-12 hours. They then migrate across venule and capillary walls. Their lifespan may be 4 days in connective tissues, where they are avidly phagocytic—scavengers that engulf bacteria, cell debris, and foreign matter. The specific granules contain bactericidal enzymes for receptor-mediated phagocytosis. Neutrophil numbers increase in acute bacterial infections.
Like all leukocytes, neutrophils circulate in the blood for a short time and migrate across small blood vessel walls to perform functions outside the circulation. Neutropenia is an abnormal decrease in neutrophil numbers in peripheral blood so that too few cells are available to defend against bacterial infections. Neutropenia may be caused by genetic, drug-induced, or other factors, but it is often associated with autoimmune diseases and is a common feature of AIDS.
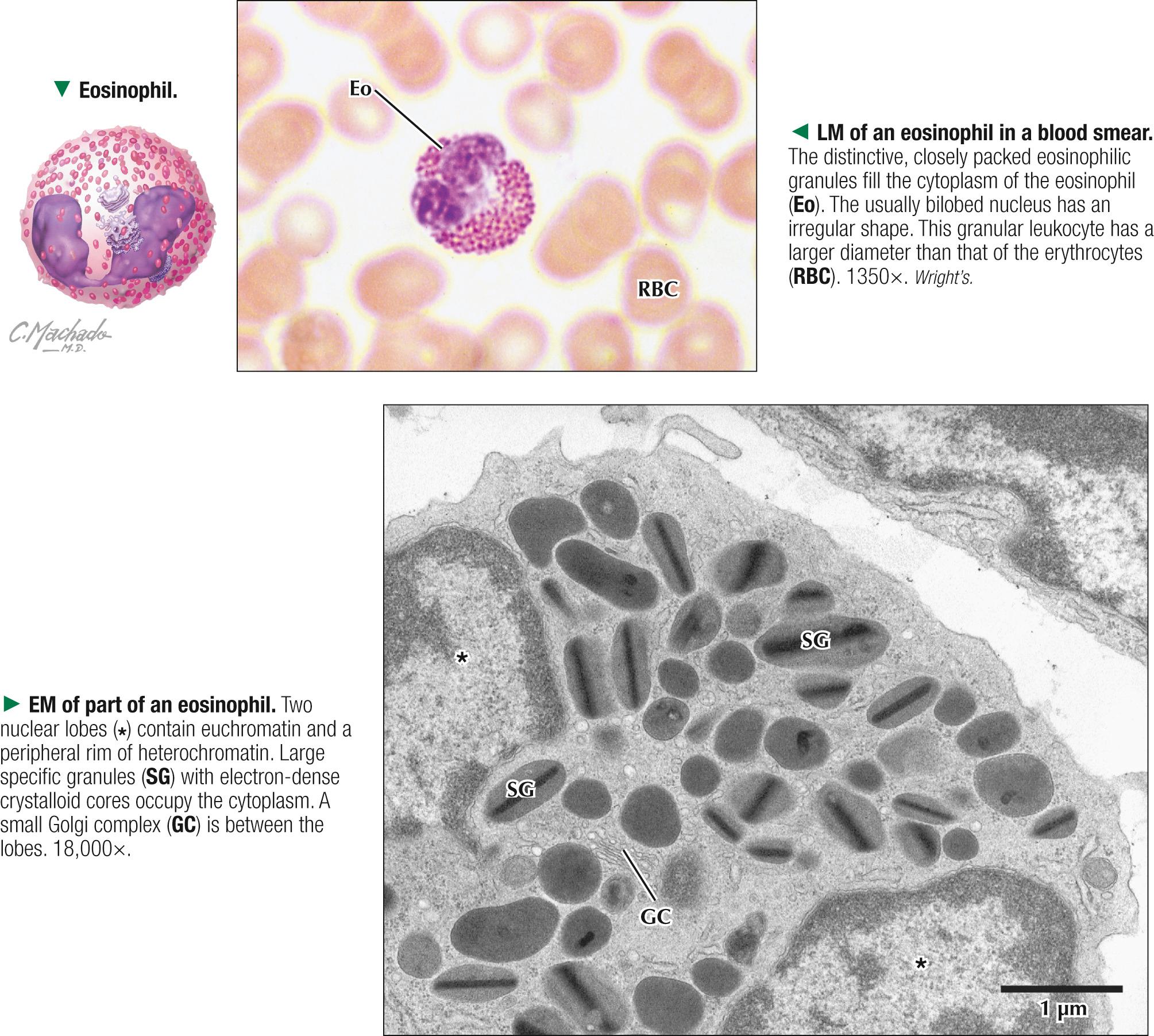
Eosinophils make up a small proportion of leukocytes in peripheral blood: 1%-4% of the leukocyte count. Eosinophil numbers normally fluctuate and show a diurnal pattern, with larger numbers often at night and lower numbers in daytime. With a diameter of 12-15 µm, they are slightly larger than neutrophils. Their nucleus is typically bilobed, but multiple lobes are not unusual. Their specific granules are distinctive, uniform in size, highly refractile, and have an affinity for acid dyes and thus stain dark pink to crimson. These granules contain various hydrolytic enzymes and secrete histaminase, which inactivates histamine produced by basophils and mast cells. Electron microscopy shows the membrane-bound specific granules to have an irregular shape, ranging from ellipsoid to a football form, and in some species, including humans, to have an internal crystalloid core. This core makes them highly refractile by light microscopy. Eosinophils circulate in the bloodstream for 6-8 hours; once they migrate to connective tissues, their lifespan is 8-10 days. Eosinophils are common in mucosal connective tissues in the respiratory and gastrointestinal tracts. The cells release various substances including major basic protein, peroxidase, and eosinophilic cationic protein. The cells phagocytose antigen-antibody complexes and parasites, and elevated cell numbers occur in parasitic infections and allergic responses such as hay fever and asthma.
Eosinophilia —an increased absolute number of circulating eosinophils above normal—occurs in parasitic infestations, allergic reactions, and some malignancies. Eosinophils play a central role in controlling parasitic diseases such as schistosomiasis. They kill parasitic larval helminths by releasing toxic molecules from the specific granules. In bronchial asthma and allergic eczema, local eosinophil accumulations in tissues may cause severe cell injury and necrosis. These harmful effects are likely related to major basic protein and eosinophil cationic protein, which are components of the specific granules.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here