Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Atrioventricular (AV) septal defects are characterized by a deficiency or absence of septal tissue immediately above and below the normal level of the AV valves, including the region normally occupied by the AV septum, in hearts with two ventricles. The AV valves are abnormal to a varying degree.
These defects have also been called AV canal defects, AV defects, endocardial cushion defects, ostium primum atrial septal defects (when there is no interventricular communication), and common AV orifice (when there is only a single AV valve orifice).
Abbott apparently recognized ostium primum atrial septal defect (ASD) and common AV canal defect, but it was Rogers and Edwards who in 1948 recognized their morphologic similarity. This concept was further elaborated by Wakai and Edwards in 1956 and 1958. The terms partial and complete atrioventricular canal defects were introduced by these investigators, who realized nonetheless that not all cases fit their definitions. During this period, Lev was formulating his concepts of ostium primum ASD (or partial AV canal) and common AV orifice (or complete AV canal), and he described the position of the AV node and bundle of His in these malformations. Wakai and Edwards and later Bharati and Lev became dissatisfied with trying to compress all cases into two categories and added the terms intermediate and transitional . During this period, Van Mierop's scholarly studies added a great deal of knowledge about the overall anatomic features of AV septal defects.
By the early 1960s, surgical treatment of these defects provided a stimulus to further morphologic studies. In 1966, Rastelli and colleagues at the Mayo Clinic described in more detail the morphology of AV valve leaflets in cases with common AV orifice. The error made in this study was to compress into the designation common anterior leaflet a leaflet that was in fact divided in two by a commissure (i.e., the divided common anterior leaflet of type A). The description of AV valve leaflets by Rastelli and colleagues was accepted for some years, but in 1976 a publication by Ugarte and colleagues emphasized the idea of leaflets bridging the ventricular septum, a concept also held by Lev. Meanwhile, based on anatomic and cineangiographic studies and in accordance with the description of Baron and colleagues and Van Mierop and colleagues, it was recognized in the late 1960s that the basic defect in these malformations was absence of the AV septum . This concept is particularly important because the AV septum can be imaged by echocardiography and in the left ventriculogram in the right anterior oblique projection. These concepts were further expanded by Piccoli and colleagues under the direction of Anderson, who further emphasized that all the variations of the defect were part of a spectrum ,P8 ( Fig. 34-1 ).
 valves viewed from atrial side (surgical orientation). A, Normal, with anterior and posterior mitral valve (MV) leaflets and septal, anterior, and posterior tricuspid valve (TV) leaflets. B, Leaflets in partial AV septal defects. Left superior (LSL) , left inferior (LIL) , and left lateral (LLL) leaflets form left AV valve; right superior (RSL) , right inferior (RIL) , and right lateral (RLL) leaflets form right AV valve. C, Leaflets in complete AV septal defects, or common AV orifice, are similar to those in B . However, LSL and LIL are not connected. LIL usually bridges a little (grade 1 or 2, based on 1 to 5) across crest of ventricular septum. LSL may bridge slightly or not at all (grade 0 or 1, Rastelli type A), moderately (grade 2 or 3, Rastelli type B), or markedly (grade 4 or 5, Rastelli type C). Key: AL, Anterior leaflet; PL, posterior leaflet; SL, septal leaflet.")
In 1952 at the University of Minnesota Hospital in Minneapolis, after a long period of laboratory investigation, Dennis and Varco attempted for the first time a cardiac operation in a human using a pump-oxygenator. The preoperative diagnosis was ASD, and at operation the defect was thought to be closed. The patient died, and autopsy showed the true diagnosis to be partial AV septal defect (Edwards JE: personal communication, 1980). The first successful repair of a complete AV septal defect was performed by Lillehei and colleagues in 1954, using cross-circulation and direct suture of the atrial rim of the septal defect to the crest of the ventricular septum. In 1954, Kirklin and colleagues successfully repaired a partial AV septal defect through the atrial well of Watkins and Gross, and in 1955 began repairing AV septal defects by open cardiotomy and use of the pump-oxygenator.
Early experiences with complete AV septal defects were all associated with a high hospital mortality, often related to complete heart block, postrepair left AV valve regurgitation, or creation of subaortic stenosis. Interestingly, in many of these early operations, a two-patch technique was used (see “ Two-Patch Technique ” under Technique of Operation later in this chapter). In 1958, Lev's description of the location of the bundle of His provided the basis for repair techniques that avoid heart block. In 1959, Dubost and Blondeau reported their early experience and emphasized that the “cleft” in the “mitral leaflet” need not be sutured in repairing partial AV septal defects, a concept currently challenged. In 1962, Maloney and colleagues described two cases in which a single patch was used to close both defects and with the valve tissue suspended from the patch. This technique was again described by Gerbode in 1962 and was associated with decreased in-hospital mortality. McGoon recognized the importance of “taking from the tricuspid valve” to leave sufficient tissue from which to create an adequate left AV valve. These technical advances allowed repair of even the more complex variants of the defect. Subsequently, good results were obtained in patients older than about 2 years of age, but results in infants remained relatively poor. Between 1968 and 1971, Barratt-Boyes successfully repaired this anomaly in four severely ill infants ; subsequently, improved results in infants were reported by many others.
In 1978, Carpentier again emphasized (as did Dubost and Blondeau ) that generally, the left AV valve functions best when repaired as a three-leaflet valve. As a result of these advances, risks of operation for nearly all types of AV septal defect are now low.
AV septal defects have as defining characteristics a deficiency or absence of the AV septum, resulting in an ostium primum defect immediately above the AV valves and a deficiency (or scooped-out area) in the inlet (basal) portion of the ventricular septum immediately below the AV valves.
Patients with partial AV septal defects have a normal length of atrial septum, and the ostium primum ASD is the result of absence of the relatively small AV septum plus some deficiency in the inlet portion of the ventricular septum. The deficiency in the inlet portion of the ventricular septum is variable, but on average is greater in patients with complete AV septal defects than in those with partial defects.
These septal deficiencies may or may not result in interatrial or interventricular communications, depending on configuration and attachments of the AV valves ( Tables 34-1 and 34-2 ). Whereas the basic defect in these malformations is absence of the AV septum, whether the ventricular septal or atrial septal deficiency or the AV valve abnormality is the result only of AV septal absence is still debated.
a Study is based on data from 310 surgical patients.
b Condition in which the characteristic atrioventricular (AV) septal deficiency is present, but the AV valves are adherent on their atrial side to the edge of the defect, resulting in no interatrial communication.
| Beneath Left Superior Leaflet | Beneath Left Inferior Leaflet | |||
|---|---|---|---|---|
| Size | No. | % of 310 | No. | % of 309 a |
| 0 b | 158 | 51 | 176 | 57 |
| 1 | 3 | 1.0 | 3 | 1.0 |
| 2 | 9 | 2.9 | 9 | 2.9 |
| 3 | 4 | 1.3 | 16 | 5.2 |
| 4 | 9 | 2.9 | 22 | 7.1 |
| 5 c | 127 | 41 | 82 | 27 |
a Data not available for one patient.
b Condition in which the characteristic atrioventricular (AV) septal deficiency is present, but the AV valves are adherent on their ventricular side to the crest of the ventricular septum, resulting in no interventricular communication (if this occurs under both left AV valve leaflets, it is commonly called partial AV septal defect . If size greater than 1 occurs under both AV valve leaflets, the condition is commonly called complete AV septal defect ).
Five or more AV valve leaflets of variable size are usually present (see Fig. 34-1 ), but there is often variability in completeness of commissures and prominent crenations in the leaflets ( Fig. 34-2 ). For example, among the 43 hearts with all types of AV septal defects and 2 ventricles in the GLH autopsy series in which the number of leaflets could be accurately assessed, 10 (23%) had 4 leaflets, 18 (42%) had 5 leaflets, 14 (33%) had 6 leaflets, and 1 (2%) had 7 leaflets. When a large interventricular communication was present (complete AV septal defect), the most common number of leaflets was 5 (16 of 28, or 57%).
 valves in AV septal defects viewed from atrial aspect in a series of fixed specimens. A, Specimen with partial AV septal defect in which left superior (LS) and left inferior (LI) leaflets are adherent to crest of ventricular septum and there is no interventricular communication. Arrow marks line of closure between LS and LI leaflets, formerly called the “cleft in the anterior mitral leaflet.” Note that as usual, LS leaflet does not bridge septum (there is no leaflet tissue in the position of the superior portion of the normal tricuspid septal leaflet). In this heart, as is not uncommon, there are two left lateral and two right lateral leaflets. B, Specimen with complete AV septal defect in which there are interventricular communications beneath LS and LI leaflets. LS leaflet does not bridge crest of septum. Right superior (RS) leaflet is characteristically large. LI leaflet is bridging (grade 2) and very distinct from right inferior (RI) leaflet. C, Specimen of a complete AV septal defect in which LS leaflet markedly bridges crest of septum. Correspondingly, RS leaflet is small. LS leaflet is characteristically larger than LI leaflet. Key: LA, Left atrium; RA, right atrium.")
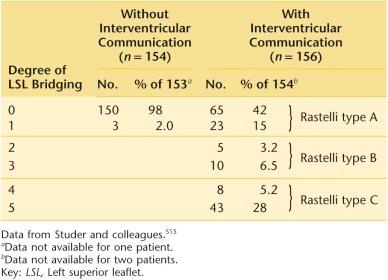
The left superior leaflet (LSL) and left inferior leaflet (LIL) are particularly variable in size, connections one to another ( Table 34-3 ), and degree of bridging across the crest of the ventricular septum ( Table 34-4 ; see Figs. 34-1 and 34-2 ). There may be one or two AV valve orifices ( Table 34-5 ).
| Degree of LSL-LIL Connection a | No Interventricular Communication ( n = 154) |
Interventricular Communication ( n = 156) |
||
|---|---|---|---|---|
| No. | % of 154 | No. | % of 156 | |
| 0 | 2 | 1.3 | 139 | 89 |
| 1 | 55 | 36 | 11 b | 7 |
| 2 | 82 | 53 | 5 b | 3 |
| 3 | 9 | 6 | 0 | — |
| 4 | 5 | 3 | 0 | — |
| 5 | 1 | 0.6 | 0 | — |
| Connected, unknown degree | 0 | 0 | 1 b | 0.6 |
a 0, Separate LSL and LIL, such as in common AV orifice; 1 and 2, narrow connections (deep cleft in “anterior mitral leaflet”); 3 and 4, broad connection (shallow cleft or notch); 5, no cleft, anterior mitral leaflet.
b Among these 17, in four the LSL and LIL were connected but free-floating, with large interventricular communications beneath them and their connections (Bharati type C ). In 11, very small interventricular communications were present beneath the LSL and/or LIL. In two, no interatrial communication was present.
| Type | No. | % of 310 |
|---|---|---|
| Two AV valves | 171 b | 55 |
| Common AV valve | 139 | 45 |
a Database is same as in Table 34-1 .
b Includes the 154 patients without interventricular communications; 11 with small interventricular communications beneath the left superior (LSL) and/or inferior leaflets (LIL); four with connected but free-floating and connected LSL and LIL (see Table 34-3 ); and two with no interatrial communication but large interventricular communication (not inlet atrioventricular septal-type ventricular septal defects).
Hearts with AV septal defects are also characterized by absence of the usual wedged position of the aortic valve above the AV valves. Instead, it is elevated and deviated anteriorly. Details of the aortic-mitral fibrous continuity often differ from those in the normal heart. Thus, continuity was abnormal in more than half of 21 specimens with normally related great arteries in the GLH autopsy series; continuity was to the base of the noncoronary cusp in only 5 (24%) and to both the noncoronary and right coronary cusps in 7 (33%). In addition, the left ventricular (LV) inflow tract is shortened in relationship to length of the outflow portion, and there is a related reduction in length of the diaphragmatic wall of the LV. The LV outflow tract is also narrowed, although rarely is the narrowing sufficient to be of hemodynamic importance in the unrepaired heart.
AV septal defects include a spectrum of malformations. At one end is the simplest type, in which there is an interatrial communication but no interventricular communication and a connection of variable width between the LSL and LIL; this is called a partial AV septal defect or ostium primum defect . At the other end of the spectrum is the most extreme form, with large deficiencies in atrial and ventricular septa, a common AV valve orifice, and large interatrial and interventricular communications; this is called a complete AV septal defect . Because a continuous spectrum of gradations lies between these extremes, some anomalies have been grouped as intermediate or transitional AV septal defects . Definitions of these intermediate types have varied but usually include presence of two AV valve orifices and a restrictive inlet ventricular septal defect (VSD), with dense chordal attachments to the ventricular septum (see “ Unusual Atrioventricular Combinations ” under Morphology). Added complexity is provided by occurrence of a large variety of major and minor associated cardiac anomalies ( Tables 34-6 and 34-7 ). In addition, Down syndrome is common, particularly in patients with an interventricular communication.
| Anomaly | No. | % of 310 |
|---|---|---|
| None | 237 | 76 |
| Patent ductus arteriosus | 31 | 10.0 |
| Tetralogy of Fallot | 20 | 6.5 |
| Completely unroofed coronary sinus with left SVC | 9 | 2.9 |
| Situs ambiguus | 7 | 2.3 |
| DORV without PS | 6 | 1.9 |
| Additional VSDs | 5 | 1.6 |
| DORV + PS | 3 | 1.0 |
| Situs inversus totalis | 3 | 1.0 |
| TAPVC | 2 | 0.6 |
| Left ventricular outflow obstruction | 2 | 0.6 |
| Transposition of the great arteries | 1 | 0.3 |
| PS, supravalvar mitral stenosis, Ebstein malformation, coarctation, isolated dextrocardia | 1 each | 0.3 |
| Without Interventricular Communication ( n = 154) |
With Interventricular Communication ( n = 156) |
|||||
|---|---|---|---|---|---|---|
| Anomaly | No. | % of 154 | CL (%) | No. | % of 156 | CL (%) |
| (Sizable) ASD a | 17 | 11 | 8-14 | 32 | 21 | 17-24 |
| Left SVC without unroofed coronary sinus | 10 | 6 | 4-9 | 7 | 4 | 3-7 |
| Partially unroofed coronary sinus | 5 | 3 | 1-5 | 2 | 1 | 0.4-3 |
| Azygos extension of IVC | 4 | 3 | 1-5 | 3 | 1 | 0.6-3 |
| IVC to lower left common atrium | 1 | 1 | 0.1-2 | |||
| Bilateral IVCs | 1 | 1 | 0.1-2 | |||
| TASVC to common atrium | 1 | 1 | 0.1-2 | |||
| Right PVs to RA | 1 | 1 | 0.1-2 | |||
| Anomalous origin LAD from RCA (TF) | 1 | 1 | 0.1-2 | |||
| Origin stenosis LPA (not TF) | 1 | 1 | 0.1-2 | |||
| Wolff-Parkinson-White syndrome | 1 | 1 | 0.1-2 | |||
| Spontaneous heart block | 1 | 1 | 0.1-2 | |||
| Coronary artery disease requiring CABG | 1 | 1 | 0.1-2 | |||
Because it is virtually impossible to subdivide the spectrum of AV septal defects into satisfactory noncontroversial subgroups, this chapter describes cases based on morphologic and functional variables rather than categorizing them into subgroups. The older imprecise terms continue to be useful as shorthand, and in this chapter, partial AV septal defect refers to a malformation with two AV valve orifices and no interventricular communication, whereas complete AV septal defect refers to a malformation with a common AV valve orifice and large (grade 2 or more) nonrestrictive interventricular communication.
Usually there is an interatrial communication related to deficiency of the AV septum, the so-called ostium primum ASD ( Fig. 34-3 ). The defect is bounded below by the inferiorly displaced AV valve leaflets and above by a crescentic ridge of atrial septum that fuses with the AV valve anulus only at its extremities.
 septal defect. A, View from right atrium and right ventricle. Large ostium primum atrial septal defect is seen above AV valve leaflets. No interventricular communication is present beneath the leaflets. However, deficiency of basal (inlet) portion of ventricular septum is apparent. Left superior (LS) leaflet is attached firmly by fibrous tissue to crest of septum (dashed line) and does not bridge onto right ventricular side. There is thus a bare area on right side of superior aspect of ventricular septum (arrow) . Left inferior (LI) leaflet bridges on right ventricular side. Right superior (RS) leaflet is clearly visible, but right lateral and inferior leaflets are not in photograph. B, Left ventricular outflow view. LS and LI leaflets are firmly attached to crest of ventricular septum. Narrowing and elongation of left ventricular outflow tract are apparent. This figure makes clear why, in describing position of the two leaflets attached to the ventricular crest, the terms superior and inferior are preferable to anterior and posterior , terms that lead to confusion with normal mitral leaflets.")
Generally, there is little atrial septal tissue at the superior point of fusion of the atrial septum with the valve anulus adjacent to the aorta, but more tissue is usually present inferiorly adjacent to the coronary sinus ( Fig. 34-4 ). The distance between the crescentic atrial margin of the defect and the AV valves (and thus the size of the interatrial communication) is variable. In most cases, the fossa ovalis is normally formed and there is a patent foramen ovale or an associated fossa ovalis ASD. Usually the interatrial communication through the ostium primum defect is moderate in size. When the interatrial communication is small, the atrial septal deficiency is restricted to the area normally occupied by the AV septum. The communication may be still smaller due to fusion of the base of the LSL or LIL to the edge of the adjacent portion of the atrial septum. Rarely, there may be an accessory “parachute” of fibrous tissue that narrows or obstructs the defect. Under such circumstances, a pressure difference exists between the two atria.
 septal defect. Coronary sinus ostium (CoS) is seen inferior and posterior to ostium primum (P) defect in atrial septum. Approximate position of AV node and bundle of His is shown as a dashed line. Placement of inferior part of patch suture line is shown by the line of x's. Key: EV, Eustachian valve of inferior vena cava; FO, fossa ovalis; SVC, superior vena cava.")
Deficiencies in the anterior limbus or fossa ovalis may be associated with AV septal defects, resulting in a larger interatrial communication. Occasionally the entire limbus and fossa ovalis are absent, along with the AV septum. The condition is then termed common atrium (see Table 34-1 ).
Rarely, AV valve tissue is attached completely to the edge of the atrial septum, and no interatrial communication exists despite the deficiency in the septum (see Table 34-1 ). In this unusual variant, the characteristic deficiency of the inlet (basal) portion of the ventricular septum is also present and associated with a large interventricular communication beneath the leaflets. The functionally left AV valve, consisting only of those portions of the LSL and LIL on the left side of their attachment to the atrial septum, tends to be competent. As seen from a right atrial approach, part of the right AV valve may have chordal attachments across the ventricular defect to the left side of the septum—that is, it is straddling. When viewed from the ventricular side, the appearance is typical of a complete AV septal defect. It is distinct from an inlet type of perimembranous VSD that is sometimes called inlet septal, AV septal, or AV canal type of VSD, which is unrelated to deficiency of the AV septum (see “ Inlet Septal Ventricular Septal Defect ” under Morphology in Chapter 35 and “ Inlet Septal Type of Ventricular Septal Defect ” in text that follows).
Some degree of deficiency of the inlet portion of the ventricular septum immediately beneath the AV valves is a constant finding. Thus, the inlet portion of the ventricular septum is shortened. There is usually no interventricular communication when the LSL and LIL are connected and attached to the downwardly displaced crest of the septum throughout its length ( Fig. 34-5 ; see also Fig. 34-3 ), the situation described as a partial AV septal defect . Occasionally, one or several small interventricular communications are present beneath the attachment of the AV valve to the septum ( Fig. 34-5, B ).
 septal defects. A, Partial AV septal defect viewed from opened left ventricle. Left superior (LS) and left inferior (LI) leaflets are completely attached to crest of a deficient ventricular septum (VS) . Area of contact or closure between left superior and left inferior leaflets is indicated by arrow. In this specimen, only the anterior papillary muscle (APM) is present (“parachute” mitral valve). B, Intermediate type of AV septal defect from left ventricular view. Numerous small interventricular communications are present between thick, short chordae that tether both LS and LI leaflets to ventricular crest. Fibrous tissue extending from superior leaflet to below right coronary aortic cusp (RC) represents remnant of membranous septum. C, Complete AV septal defect viewed from left ventricular aspect. LS and LI bridging leaflets are free floating, and there is a large interventricular communication between them and the underlying crest of the ventricular septum. This specimen also has double outlet right ventricle. Key: AoV, Aortic valve; LL, left lateral leaflet; NC, noncoronary aortic cusp.")
With ventricular septal deficiency generally greater than that in a partial AV septal defect, a moderate or large interventricular communication may be present, and usually the LSL and LIL are separate. This anomaly is described as a complete AV septal defect ( Fig. 34-5, C ). Deficiency of the inlet portion of the ventricular septum (the “scoop”) is generally deeper in hearts with complete AV septal defects than in those with partial AV septal defects. Often the communication is particularly large beneath the LSL and smaller beneath the LIL (see Table 34-2 ), whereas in about 5% of cases there is a larger interventricular communication beneath the LSL and none beneath the LIL. Rarely, there is no VSD beneath the LSL and a large one beneath the LIL.
A remnant of the membranous ventricular septum may be present (see Fig. 34-5, B ). This was the case in 8 of 27 (30%) GLH autopsy specimens of AV septal defect with normally related great arteries; in 19 specimens the membranous septum could not be identified.
Attachments of the AV valves to the crest of the ventricular septum in partial AV septal defects, as well as their chordal attachments in complete AV septal defects, are displaced toward the apex of the heart because of deficiency of the inlet (basal) portion of the septum. This alters orientation of the AV orifices relative to the aortic orifice (i.e., the aortic valve is no longer wedged between the AV valves) and provides an important diagnostic imaging criterion of this malformation.
Typically when two AV valve orifices are present, as in partial AV septal defects, the LSL and LIL are joined together to a variable extent anteriorly by leaflet tissue near the crest of the ventricular septum (see Figs. 34-1 and 34-3 ). Together they resemble an anterior (septal) mitral leaflet with a cleft, but in fact the left AV valve is tricuspid and oriented differently from the normal valve (see Figs. 34-1 and 34-2 ). The connection between the LSL and LIL may be only a thin strand of tissue (complete cleft), but more commonly it is 2 to 4 mm or more deep (see Table 34-3 ). This connection, too, is usually fused to the crest of the ventricular septum in partial AV septal defects. Occasionally, chordae pass from opposing edges of the LSL and LIL to the muscular ventricular septum beneath. Yilmaz and colleagues identify a difference in this area of separation and distinguish between a commissure supported by chordal apparatus on either side of the gap and a cleft that is relatively unsupported and bereft of chordae at its edges. In addition, the chordae that originate from the central edges of the LSL and LIL attach to different papillary muscles, which can cause a distracting force on the leaflets during closure. This contrasts with the normal commissure in which the chordae from adjacent leaflet edges attach to a single papillary muscle, encouraging coaptation. Rarely, separation into LSL and LIL is represented only by a notch in the center of the free edge of a nearly normal “anterior mitral leaflet.” The left lateral leaflet (LLL) is usually smaller than the other two leaflets and is triangular.
In aggregate, these left AV valve leaflet anomalies may make the valve regurgitant to a variable degree, sometimes severely ( Table 34-8 ). When LSL and LIL are nearly completely separated (connection grades 1 and 2; see Table 34-3 ), an appreciable gap may occur during systole, producing regurgitation. When there is failure of valve coaptation at this site, leaflet tissue forming the margin usually becomes thickened and rolled. In other cases, regurgitation appears to be due to deficiency of leaflet tissue, particularly in the LIL. The mechanism of severe left AV valve regurgitation is, however, not evident in some cases. The jet of regurgitation is usually directed into the right atrium. Rarely, the left AV valve is stenotic, but this usually is associated with hypoplasia of the LV.
The right AV valve is also abnormal when there are two AV orifices, although less attention has been paid to it. It may consist of three leaflets—right superior leaflet (RSL), right lateral leaflet (RLL), and right inferior leaflet (RIL)—or of two or four leaflets (see Figs. 34-1 and 34-2 ). Leaflet tissue attached directly or by chordae to the crest or right side of the crest of the septum, and thus contributing to closure of the right AV valves, is considered to represent bridging of the LSL or LIL (see Fig. 34-1 ).
Usually in cases without an interventricular communication, the LSL does not bridge at all (previously, this finding was interpreted as absence or hypoplasia of the superior part of the tricuspid septal leaflet) and the LIL bridges moderately (see Fig. 34-2, A ). Even with abnormalities of the right AV valve, regurgitation is rare (unless right heart failure develops).
When the AV valve orifice is a common one and the interventricular communication is large (complete AV septal defect), the LSL and LIL are separate, and a bare area is exposed on the crest of the ventricular septum ( Fig. 34-6 ; see Figs. 34-1 and 34-5, C ). The LSL may be entirely on the LV side of the septum or may, to a variable degree, bridge the septum and extend onto the right ventricular side (see Fig. 34-2, B-C and Table 34-4 ). This variability formed the basis for the classification by Rastelli and colleagues into types A, B, and C. Chordal attachments of the right ventricular extremity of the LSL vary according to degree of bridging P8 ( Fig. 34-7 ). When there is no bridging, chordal attachments are to the ventricular crest ( Fig. 34-7, A ). With mild bridging, they are to the medial papillary muscle in the right ventricle; with moderate bridging, to an accessory (often large) apical papillary muscle ( Fig. 34-7, B ); and with marked bridging, to the normally positioned (although often bifid) anterolateral papillary muscle of the right ventricle ( Fig. 34-7, C ). When the LSL bridges the septum moderately or markedly and extends into the right ventricle, it is usually unattached to the underlying ventricular crest (free-floating), but it may occasionally be attached by chordae (tethered). Length of the chordal or fibrous attachments to the right side or crest of the ventricular septum varies according to size of the interventricular communication or the position of the leaflet.
 does not bridge, resulting in a bare area of crest of ventricular septum on right ventricular side, where in a normal heart, superior aspect of septal leaflet touches septum. A small fossa ovalis atrial septal defect is also present. Key: CoS, Coronary sinus; LI, left inferior leaflet.")
 leaflet. A, Nonbridging (bridging grade 0) LS leaflet (Rastelli type A). This surgical specimen (the patch having been removed) is viewed from right atrium. Arrow marks mildly bridging left inferior (LI) leaflet. B, Moderate (grade 2 or 3) bridging of LS leaflet. Chordae from its right ventricular extremity go to a papillary muscle in right ventricle. Arrow indicates bridging portion of LI leaflet. (Rastelli and colleagues termed this type B , but it is just part of the spectrum of bridging.) C, Marked (grade 5) bridging of LS leaflet (Rastelli type C). Arrow marks bridging part of LI leaflet. Key: RS, Right superior leaflet; S, ventricular septal crest.")
The LIL typically bridges moderately, but it too varies in this respect. It is not uncommon for a bridging LIL to be attached to the underlying ventricular crest either completely or by short, thick chordae with interchordal spaces.
Chordal attachments of the leftward components of the common AV valve in the LV are usually relatively normal, although the posterior papillary muscle is displaced more laterally than normal and a third papillary muscle may be present. There may be only one papillary muscle, producing a parachute-type valve that is difficult to repair. This was true in 7 of 53 (13%) cases in the GLH autopsy series, in 14% of the specimens described by David and colleagues, and in 4% of 155 surgical cases reported by Ilbawi and colleagues.
The right ventricular portion of the common AV valve has superior, lateral, and inferior leaflets, but as in partial AV septal defects, they vary considerably in number and size (see Fig. 34-2 ). When bridging of the LSL is absent or mild, the RSL is large, whereas with more extensive bridging, it is smaller. P8
When leaflets of the common AV valve close appropriately during ventricular systole, AV valve regurgitation is absent or mild. However, important left AV valve regurgitation may be present (see Table 34-8 ). The mechanism of the regurgitation is often not clearly understood.
Anatomic studies by Kanani and colleagues have emphasized the marked valvar abnormalities in this malformation, not only of the anular component but also of the subvalvar apparatus (with deficiency of chordal arrangement) and leaflet tissue (which is often deficient in coaptation surface and pliability following repair).
Other unusual combinations of size, connections, attachments, and degree of bridging of AV valve leaflets in the spectrum of AV septal defects prompted Wakai and Edwards, Bharati and colleagues, and others to use a transitional or intermediate category . Rarely in patients with two AV valve orifices with no interventricular communication beneath the LSL and LIL, these leaflets are connected only by a fibrous strand adherent to the ventricular septal crest (see Tables 34-3 and 34-5 ), forming what Bharati and colleagues have called a “pseudomitral leaflet,” rather than an “anterior mitral leaflet with a complete cleft.”
In such patients, deficiency of LIL tissue and severe left AV valve regurgitation are common. Occasionally when the LSL and LIL are connected (and thus two AV valve orifices are present), one or multiple small interchordal interventricular communications are present beneath the leaflets (see Tables 34-2 and 34-5 ), and occasionally one or two larger holes may be present ( Fig. 34-8 ; see Fig. 34-5, B ). In about 1% of cases, the connected LSL and LIL have large interventricular communications beneath them; in these patients, the connection is a thin strand of valve tissue beneath which there is also a large interventricular communication ( Fig. 34-9 ), but two AV valve orifices can be said to be present (see Table 34-5 ). Bharati and colleagues have referred to this as intermediate type C .
 septal defect viewed from left ventricular aspect. Left superior (LS) leaflet is connected to left inferior (LI) leaflet by leaflet tissue, resulting in two AV valve orifices; yet there are interventricular communications between short, thick chordae connecting leaflets and their connection to scooped-out underlying ventricular septum. LS and LI leaflets, particularly the latter, are deficient.")
 and left inferior (LI) leaflets are connected by leaflet tissue, and thus two AV valve orifices are present. However, the interventricular communication is large, and neither connection nor leaflets are attached to scooped-out underlying ventricular septum.")
An accessory orifice (double left AV valve orifice) is present in the commissure on one side, usually the inferior side, of the LLL in about 5% of cases ( Table 34-9 ). A ring of chordae surrounds the orifice, and a very small papillary muscle is usually beneath it. The accessory orifice may be conceptualized as an incomplete commissure, and the fibrous tissue “bridge” between the accessory orifice and main orifice consists of valvar tissue and chordae. This emphasizes the danger of producing regurgitation by cutting the bridge. The LLL is often underdeveloped when an accessory orifice is present. Accessory orifices predispose patients to stenosis after repair.
A single papillary muscle in the LV uncommonly (about 5% of cases) complicates AV septal defects, most commonly the complete type. All chordae of the left AV valve leaflets insert into this single papillary muscle, which is usually situated anteriorly in the LV. In complete AV septal defect with a free-floating and bridging LSL, no LV inflow obstruction results. Otherwise, or after repair, the situation is entirely analogous to a true “parachute mitral valve” (see “Papillary Muscle Anomalies” under Morphology in Chapter 50 ), and inflow obstruction can complicate intracardiac repair.
The LV outflow tract is characteristically elongated and narrowed ( Fig. 34-10 ) in all types of AV septal defect (see “ General Morphologic Characteristics ” under Morphology earlier in this chapter).
 leaflet and connection of leaflet to underlying ventricular septum by long chordae. Narrowness of left ventricular outflow tract is apparent.")
In AV septal defect with large interventricular communications, the LV may be abnormally large, but its size is variable, both absolutely and in relation to the right ventricle. In the severely right-dominant type of AV septal defect, the LV is severely hypoplastic ( Fig. 34-11 ). In such cases, the atrial septum may be displaced leftward in relation to the plane of the ventricular septum, in which case it overrides the left AV valve to a varying degree and may be associated with hypoplasia of the left atrium. This variant is therefore sometimes included in “hypoplastic left heart physiology” (see Chapter 49 ).
 septal defect with hypoplasia of left ventricle and a dominant right ventricle (RV) . Specimen is viewed from its right atrial aspect, and a probe (P) passes into left ventricular cavity. The common AV valves open almost entirely into right ventricle. Arrow indicates superior margin of the ostium primum atrial septal defect. Key: CoS, Coronary sinus.")
The right ventricle has no specific anomalies, but is usually enlarged secondary to the left-to-right shunt. Its size is also variable, and occasionally it is importantly hypoplastic.
The LV or right ventricle is severely hypoplastic in about 7% of patients born with complete AV septal defect. Prevalence of the two types is similar. Presence of severe ventricular hypoplasia can increase risk of surgical correction and may demand a Fontan-type repair, alone or with a technique for correcting the hypoplastic left heart physiology (see Special Situations and Controversies later in this chapter and Chapter 41 ).
Usually the two AV valves or common AV valve orifice lies in proper proportion over the two ventricles. When one ventricle is hypoplastic, the ventricular septum is malaligned and lies more to the side of the hypoplastic ventricle (see Fig. 34-11 ).
Less commonly, the atrial septal remnant is malaligned, and then usually leftward. When this is severe, both AV valves (or common AV valve orifice) are accessible only from the right atrium, and blood exists from the left atrium only through the ostium primum defect (so-called double outlet right atrium).
Important LV outflow tract obstruction occurs rarely in unoperated hearts (about 1% of cases) in all types of AV septal defect. It more often becomes apparent as a postoperative complication. It is surprising that it is not more frequent, in view of the elongation and narrowing of this area in affected hearts.
Part of the elongation and narrowing is due to the more extensive area of direct fibrous continuity between the aortic valve and the LSL than is present normally between the aortic and mitral valves. This is caused in part by the short, thick chordae that often anchor the LSL to the crest of the ventricular septum. Also, the anterolateral muscle bundle of the LV (muscle of Moulaert) bulges more into the LV outflow tract in hearts with AV septal defects than in normal hearts, contributing to the tendency to outflow obstruction after repair. In addition to these basic arrangements tending to narrow the LV outflow tract, LV obstruction may be contributed to by morphologically discrete subaortic stenosis or by excrescences of AV valve tissue heaped up in the LV outflow tract. It may also result from abnormally positioned papillary muscles. Occasionally, its presence is overlooked preoperatively, and it becomes apparent or develops only after operation.
Important LV inflow obstruction may occur rarely. This may be from simple narrowing of the AV valve entrance into the LV, usually associated with marked right ventricular dominance. It may be related to presence of an accessory AV valve orifice on the left side, or it may result from cor triatriatum (see Chapter 32 ) or a supravalvar fibrous ring. These associated cardiac anomalies appear to be more prevalent in patients without Down syndrome.
The defect in the AV septum often displaces the coronary sinus ostium inferiorly, which may appear to lie in the left atrium, especially when the ostium primum atrial defect is particularly large. The AV node is also displaced inferiorly (caudally) and lies in the posterior right atrial wall between the orifice of the coronary sinus and ventricular crest ( Fig. 34-12 ) in what has been termed the nodal triangle . The bundle of His passes forward and superiorly from the node to the ventricular crest, reaching it where the crest fuses posteriorly with the AV valve anulus. It then courses along the top of the ventricular septum beneath the bridging portion of the LIL, giving off the left bundle branches. As it reaches the midpoint of the crest of the ventricular septum, it becomes the right bundle branch, which continues along the crest a little farther before it descends toward the muscle of Lancisi and moderator band. These anatomic findings have been supported by electrophysiologic studies at operation. This morphology of the conduction system is a determinant of the electrocardiographic pattern usually seen in AV septal defects.

Table 34-6 presents the prevalence of the major cardiac anomalies associated with AV septal defects.
A patent ductus arteriosus is present in about 10% of patients with AV septal defects. It is particularly common in those with an interventricular communication.
Typical tetralogy of Fallot is present in about 5% of patients with complete AV septal defects, and about 1% of patients with tetralogy of Fallot have associated complete AV septal defects. The LSL bridges markedly and is free-floating over the crest of the ventricular septum, and the interventricular communication beneath it is large and juxtaaortic. An interventricular communication beneath the LIL is present in only about half of cases. Rarely the LSL and LIL are connected by a fibrous (or valvar) band, beneath which also is a large interventricular communication. The right ventricular outflow tract has typical tetralogy morphology (see Chapter 38 ) that may be so severe that pulmonary atresia is present. Localized narrowing occasionally occurring in that portion of the LV outflow tract just upstream from the recess formed by the subaortic deficiency of the ventricular septum further complicates the situation in rare cases.
Double outlet right ventricle (DORV) without pulmonary stenosis complicates complete AV septal defect in about 2% of cases. As in tetralogy of Fallot, usually deficiency of the ventricular septum is large and juxtaaortic beneath the extensively bridging and free-floating LSL. However, occasionally the interventricular communication is far from the aortic and pulmonary valves and is “noncommitted.” Rarely, Taussig-Bing type of DORV is present. DORV combined with severe pulmonary stenosis coexists with complete AV septal defects in about 1% of cases. These combinations of DORV and AV septal defect with large interventricular communication frequently also have atrial isomerism or situs inversus, common atrium, completely unroofed coronary sinus with left superior vena cava, azygos extension of the inferior vena cava, or total anomalous pulmonary venous connection.
Very rarely, transposition of the great arteries (discordant ventriculoarterial connection) is associated.
Completely unroofed coronary sinus with persistent left superior vena cava (see Chapter 33 ) attached to left atrium occurs in about 3% of patients with an interventricular communication and in about 3% without, and is more frequent when common atrium is present. A partially unroofed distal end of the coronary sinus resulting in drainage of the coronary sinus into the left atrium occasionally occurs, but is a minor and unimportant associated anomaly. When complete AV septal defect is associated with persistent left superior vena cava and unroofed coronary sinus, atrial isomerism is also frequent (see Chapter 58 ).
Table 34-7 lists minor cardiac anomalies associated with AV septal defects.
In partial AV septal defects, as in other types of ASDs, pulmonary vascular disease is uncommon, whereas in complete AV septal defects, as with large VSDs, pulmonary vascular disease usually appears early in life and progresses.
Morphologically, pulmonary vascular disease associated with complete AV septal defects is similar to that associated with large VSDs (see “Pulmonary Vascular Disease” under Morphology in Section I of Chapter 35 ). However, it tends to progress more rapidly in patients with complete AV septal defects. Correlation between histologic findings and pulmonary vascular resistance is similar in the two conditions. The pulmonary vascular changes probably are more frequent and occur at an earlier age in patients with Down syndrome with complete AV septal defects compared with patients without Down syndrome.
Down syndrome is rare in patients with partial AV septal defects but common (about 75%) in those with complete AV septal defects. Left-sided obstructive lesions are 10 times less common in Down syndrome patients ; other associated anomalies are probably also less common, whereas advanced pulmonary vascular disease may be more frequent.
It is important to note that an isolated inlet (AV septal) type of VSD (see Morphology in Section I of Chapter 35 ) occurs without any of the features of an AV septal defect as defined in this chapter, except that it involves the inflow portion of the ventricular septum beneath the septal tricuspid valve leaflet and usually also the area of the membranous ventricular septum. The AV septum, however, is intact, and the mitral and tricuspid anuli and aortic orifice lie in normal positions. This feature allows these VSDs to be readily differentiated echocardiographically and angiographically from AV septal defects. Interestingly, in isolated inlet VSD, the anterior mitral leaflet is occasionally cleft.
Left-to-right shunting is present in AV septal defects unless severe pulmonary vascular disease has developed or important right ventricular outflow tract obstruction or pulmonary valve stenosis coexists. When there is no interventricular communication, the shunt is at atrial level and usually large, but it may be small or moderate; in such cases, a pressure gradient can be demonstrated between left and right atria. When the shunt is large and left AV valve regurgitation is mild or absent, the hemodynamic state of the patient is identical to that in isolated ASD (see Clinical Features and Diagnostic Criteria in Chapter 30 ); only right ventricular stroke volume is increased. When important left AV valve regurgitation is present, the left-to-right shunt becomes much larger; in fact, the regurgitation jet usually goes directly from LV to right atrium. Left as well as right ventricular stroke volume is increased, and marked cardiomegaly and heart failure develop early in life.
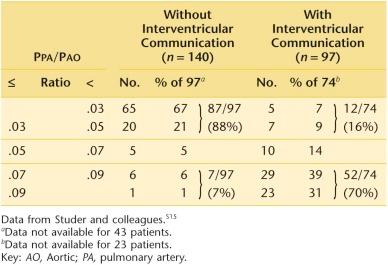
When a large interventricular communication is also present (complete AV septal defect), the left-to-right shunt is large, and right ventricular and pulmonary artery pressures approach or equal systemic pressures ( Table 34-10 ). Pulmonary vascular resistance rises rapidly and is usually importantly elevated after age 6 to 12 months and sometimes before. When present, AV valve regurgitation adds greatly to ventricular volume overload. For some reason, however, the overload usually seems to enlarge the right ventricle more than the left.
Prevalence of regurgitation at the left AV valve or common AV valve is considered to be less than before echocardiographic studies were available. Probably 10% to 15% of patients with partial AV septal defect have important regurgitation, not 40% as was estimated earlier (see Table 34-8 ). Moderate AV valve regurgitation is present in about 20% of infants with complete AV septal defects and severe regurgitation in only about 15%. AV valve regurgitation may be considerably more common in older patients with complete AV septal defects.
A not-uncommon site of regurgitation is through the gap between the LSL and LIL, particularly near the leaflet hinge or base; partly for this reason, regurgitant flow frequently goes directly into the right atrium. Under such circumstances, the left atrium remains small and the right becomes large; but when the interatrial communication is smaller or the regurgitation is sited elsewhere, regurgitation may enter the left atrium, which enlarges.
Although the precise mechanism of AV valve regurgitation is often unclear, it apparently varies considerably, as would be expected from variations in the number, size, and configuration of the leaflets and their chordal attachments. In patients with partial AV septal defects and important left AV valve regurgitation, the LIL is commonly severely hypoplastic.
Patients without an interventricular communication (partial AV septal defect) and with absent or mild left AV valve regurgitation often present in the first decade of life but may remain asymptomatic well beyond that age. Their clinical presentation is virtually identical to that of patients with the more common fossa ovalis ASD (see “Fossa Ovalis Defect” under Morphology in Chapter 30 ), except that they may have an apical systolic murmur when mild left AV valve regurgitation is present, and left axis deviation and a counterclockwise frontal plane loop.
Moderate or severe (grade 3, 4, or 5) left AV valve regurgitation in patients with partial AV septal defects may produce symptoms earlier, and progressive severe heart failure may require treatment in infancy. In addition to the usual signs of ASD, the heart is more active in association with a loud apical pansystolic murmur, and the apex of the LV may be palpable. Tachypnea and hepatomegaly are often evident.
In patients with complete AV septal defect, presentation is usually in the first year of life, frequently during the first months, as a result of progressive severe heart failure, which may not be controllable medically. There is associated tachypnea, poor peripheral perfusion, and failure to thrive. Occasionally, heart failure is minimal early in life, and presentation may be delayed until some years later, by which time there is almost always severe hypertensive pulmonary vascular disease and Eisenmenger complex (see “Clinical Findings” under Clinical Features and Diagnostic Criteria in Section I of Chapter 35 ). On physical examination, cardiomegaly with increased ventricular activity is apparent. The second heart sound at the base is split and usually fixed, with accentuation of the second component caused by elevated pulmonary artery pressure. A systolic murmur is audible over the left precordium from the shunt at ventricular level and is increased in intensity and nearer the apex when there is important AV valve regurgitation. A mid-diastolic flow murmur is characteristically widely heard both over the lower left precordium and at the apex secondary to the large diastolic flow across the malformed AV valve leaflets (depending on both the left-to-right shunt and any AV valve regurgitation).
In those patients with morphology intermediate between the partial and complete AV septal defects, clinical features depend on size of the interventricular communication and severity of left AV valve regurgitation.
In patients without an interventricular communication or important left AV valve regurgitation, the chest radiograph is the same as in other large ASDs. When moderate or severe left AV valve regurgitation is present, the radiograph usually shows marked cardiomegaly with evidence of LV, right ventricular, and right atrial enlargement and marked pulmonary plethora. Left atrial enlargement is not apparent unless the ostium primum defect is restrictive.
In complete AV septal defect, cardiomegaly and pulmonary plethora are evident in infants and young children presenting with heart failure. In patients who survive beyond this age, severely increased pulmonary vascular resistance usually dominates, and the heart is less enlarged, central pulmonary arteries are large, and lung fields are clear.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here