Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Access video content for this chapter online at Elsevier eBooks+ 
Hands are an essential part of human interaction, communication, and social integration, and apart from the face, they are the most consistently visible part of the body. Generally, the primary concern for hand surgeons is the restoration of function. However, many patients desire not only a functional extremity, but an aesthetically pleasing one, supporting the notion that fowrm and function are inextricably linked. Aesthetic discomfort has been associated with depression, anxiety, and poor health-related quality of life in patients with hand conditions and has been found to be a strong motivator even for patients seeking functional surgery. Beauty is strongly correlated with youth, and most interventions have focused on restoring a youthful appearance to the hands. As a person’s age may be estimated solely by viewing their hands, it is therefore unsurprising that the popularity of hand rejuvenation procedures has increased by over 60% in the past decade.
The ideal, youthful hand is characterized by soft-tissue fullness and inability to see underlying structures, while the aging process is marked by a combination of dermatoheliosis, motion effects, and volume loss, characterized in the hands as muscular atrophy, thinned skin, visible tendons, dorsal veins and wrinkles, and bony deformities (e.g., osteoarthritic joint deformities). Skin aging manifests as irregular pigmentation, dermal thinning, and progressive loss of skin elasticity in the form of collagen depletion. This process is influenced by genetics, but environmental factors, predominantly ultraviolet light exposure and cigarette smoking, as well as occupational exposures, can accelerate these effects Decreased skin elasticity is combined with a progressive volume loss of both the intrinsic muscles and subcutaneous fat, making the soft-tissue envelope too large for its contents and increasing the appearance of dorsal wrinkling. The loss of soft-tissue volume accentuates the prominence of the underlying tendons and metacarpal bones. Common osteoarthritic hand deformities including Heberden’s nodes, Bouchard’s nodes, and squaring of the hand at the carpometacarpal joint contribute to bony prominence and further accentuate the appearance of soft-issue deficits. In addition to increased visibility of dorsal veins due to dermal and subcutaneous atrophy, venous tortuousity also increases, in part due to incomplete venous emptying during finger flexion.
The challenge for the surgeon in treating the effects of aging involves addressing its multifocal etiology and manifestations in the skin, vasculature, soft tissue and bones. Patient tolerance for scars and complications is poor in those who seek purely aesthetic treatment, and it is essential that function be preserved in any intervention that is undertaken. Often, multiple therapies must be combined over several treatment sessions for optimal outcomes. Hand surgeons should understand both the surgical and non-surgical approaches available for rejuvenation in order to optimize outcomes.
Certain anatomic features of the hand impact both the aging process as well as influence rejuvenation. Palmar and dorsal skin are aesthetically distinct, based on their histological differences and mechanical demands, and as a result are differentially impacted by the aging process. Palmar skin has a thick dermis, ranging from 2 to 3 mm, and heavily cornified epithelium with papillary ridges that protect against shearing forces. An abundance of vertical fibers tether the thick, fibrous palmar fascia to the dermis, making this skin highly durable and less susceptible to age-related changes. The palm is characterized by multiple deep creases, which are genetically determined and independent of motion, and remain constant throughout a patient’s life. In contrast, dorsal skin is thin and soft, and the lack of tethering fibers contributes to its pliability, which is required for unrestricted motion. Even at a young age, transverse skin wrinkles can be seen over the wrist and most prominently over the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints. This thinner, more pliable skin, however, is also more susceptible to age-related changes and becomes attenuated, thinning from 1.2 mm at the age of 25 years to only 0.75 mm by the age of 70 years. As a result, wrinkles increase and progress to include non-joint surfaces in a predictable pattern over the patient’s lifespan. Fig. 42.1 demonstrates the characteristic appearance of the aged hand, highlighting dermatoheliosis and volume loss of the dorsal hand with the relative sparing of the palmar aspect.
 and volar aspect (B) .")
The subcutaneous tissue of the dorsal hand is also more complex, made up of several distinct fascial layers with intersecting fatty lamina. First investigated by Knavel et al . in 1939 in reference to the spread of infection through the hand, the anatomy of the dorsal hand was further refined in 1945 by Anson et al . and again in 2010 by Bidic et al ., with reference to implications for volume restoration. The dorsal lamina are now defined as three distinct layers, each with an associated fascial divider. Below the dermis lies the dorsal superficial lamina (DSL), which contains no structures apart from fat. The dorsal superficial fascia (DSF) separates the DSL from the dorsal intermediate lamina (DIL) which contains the dorsal veins and sensory nerves. The dorsal intermediate fascia (DIF), an extension of the antebrachial fascia of the forearm, separates the DIL from the dorsal deep lamina (DDL), which contains the dorsal extensor tendons. Lastly, the dorsal deep fascia (DDF) is the deep muscular fascia continuous with the periosteum overlying the dorsal aspect of the metacarpals. Fig. 42.2 demonstrates these distinct layers as demonstrated on histology.
 Histologic slide demonstrating dorsal superficial lamina, dorsal superficial fascia, and dorsal intermediate lamina. (B) Duplex ultrasound image demonstrating sagittal section of hand, showing the veins in the dorsal intermediate lamina. DSL, Dorsal superficial lamina; DSF, dorsal superficial fascia; DIF, dorsal intermediate fascia; DDF, dorsal deep fascia; DDL, dorsal deep lamina.")
In order to restore a youthful appearance to the hand, the basic aesthetics of the hand must first be defined. The appearance of the hand is impacted both by patient sex as well as overall body habitus. In general, males have a more square and muscular hand while female hands are typically more slender, with 25% less volume of the hand even after correction for height. Male hands generally have less subcutaneous fat, allowing visualization of the intrinsic hand muscles and tendons even in a relaxed position. In females, greater subcutaneous fat to obscure the tendons and dorsal vasculature at rest is felt to be more attractive. Hands can be categorized according to the Kretschmer’s body habitus classification, with the predominant difference in body type for both sexes manifest in finger length. Leptosome–asthenic types demonstrate a slender form and long fingers, athletic types a wide hand and balanced fingers, and pyknic types a short, wide dorsum and conically formed fingers ( Fig. 42.3 ).
 athletic, leptosome–aesthenic, and pyknic.")
Hand length has been found to be approximately 11% of total body length with the average male hand measuring 190 mm from the proximal wrist crease to the tip of the middle finger, and the average female hand 175 mm. The width of the hand is approximately 45% of the length, a similar proportion in both sexes. However, the masculine wrist is slightly wider than the feminine wrist, with a ratio of 70% in males and 67% in females. In both sexes, the middle finger is the longest finger and the only one that is straight. The ring finger reaches the middle of the nail bed of the middle finger and usually is angulated in the middle and distal phalanx toward the middle finger. The index finger is shorter, extending to the nail base of the middle finger, and also angulates toward the middle finger. Fig. 42.4 demonstrates these consistent proportions of the hand.

An aesthetically superior finger-to-hand length does not exist, but the golden proportion has been suggested as a model. The golden proportion, a mathematical ratio of two parts represented by “( a + b )/ a equals a / b equals 1.618,” approximates the Fibonacci sequence and has been referred to as a proportion of beauty. This ratio is felt to resemble balance and “dynamic” symmetry, which, contrary to static symmetry, portrays motion and rhythm. Littler was the first to apply this ratio to the hand, demonstrating that the proportion of each phalanx to the adjacent one is in perfect conformity with the golden proportion ( Fig. 42.5 ).

Although influenced by both genetics and environmental factors, the aging process in the hand in terms of dorsal wrinkling, volume loss, visibility of subcutaneous structures, and trophic changes progresses in a predictable fashion. In a study of 143 individuals, Jakubietz et al . defined the expected characteristics of age at each decade of life ( Fig. 42.6 ).
 4th decade; (B) 5th decade; (C) 6th decade; (D) 7th decade; (E) 8th decade; (F) 9th decade.")
In the second decade, the final shape and proportion of the adult hand is established. Adequate soft tissue obscures underlying structures although tendons can be visualized during finger flexion over central metacarpal heads. Dorsal veins empty completely with flexion. Multiple transverse flexion creases are seen over the PIP as well as a single crease over the DIP joint. MP joints I and III show a circular crease pattern, whereas MP joints II, IV and V show transverse creases.
In the third decade, the bones and subcutaneous structures are still obscured by a supple soft-tissue envelope. Wrinkles are few and dynamic in nature, similar to those described in the second decade.
In the fourth decade, the first signs of aging appear. Among the obliquely oriented creases of the fourth webspace, one dominant wrinkle develops and is paralleled by smaller wrinkles. This wrinkle does not yet extend over the extensor apparatus. A longitudinal wrinkle can also be seen in the first dorsal webspace. The MP III joint shows a circular wrinkle pattern, whereas MP joints I, II, IV and V show oblique wrinkles. Dorsal veins become more prominent with incomplete emptying during finger flexion.
In the fifth decade, the ulnar, dorsal wrist begins to show parallel transverse wrinkles in a neutral wrist position. An oblique wrinkle can now also be seen in webspace III, whereas the oblique wrinkle in webspace IV deepens and elongates to cross the extensor tendon. Webspace II shows an oblique wrinkle and the circular wrinkling pattern over MP III changes to a transverse pattern. The first signs of dermatoheliosis appear with solitary age spots.
In the sixth decade, the skin thins significantly. Multiple radial and ulnar oblique creases converge towards the third metacarpal head and static wrinkles emerge at the wrist. The dorsal PIP wrinkles become more prominent and take on a “sucked-out” appearance. In the midaxial line of the digits longitudinal folds appear. Both the thenar and hypothenar eminence show a loss of volume and become flat with skin redundancy. Veins do not empty during flexion and appear increasingly tortuous. The central extensor tendons III and II as well as the extensor pollicis longus (EPL) tendon become visible from the metacarpal head to the extensor retinaculum.
In the seventh decade, dermatoheliosis increases with most people demonstrating 10 or more confluent age spots. Previously obliquely oriented wrinkles have now straightened. The distal dorsum is completely covered with transverse wrinkles, while the first webspace shows longitudinal wrinkles. Due to thenar volume loss, hooding of the major wrinkle occurs. The DIP joints show multiple parallel wrinkles. Due to hypothenar atrophy, the MP V joint now forms the ulnar border of the hand. Nails begin also to demonstrate signs of aging with the development of streaks.
By the eighth decade, most people show osteoarthritic changes of the PIP and DIP joints. The extensor tendons become increasingly prominent with single fibers now visible at rest. The skin takes on a paper-thin quality. Due to muscular atrophy, the outline of the fifth metacarpal is seen as a stair-step deformity formed by the bone and the underlying hypothenar musculature.
In the ninth decade, progressive muscular atrophy results in static wrinkles across the complete dorsum. Even in flexion wrinkles can be seen over the distal dorsum. Patchy areas of hypopigmentation can now be found next to age spots.
While the progression of aging has been defined, measurement systems for the relative grading of severity are still lacking. Hand aesthetics are influenced not only by age and pathology, but by individual perception, which may be dynamic and responsive to biopsychosocial factors. In hand surgery, several outcome instruments exist that accurately measure functional outcomes, but aesthetic impressions can be more challenging to quantify, which makes comparison of disease burden and effectiveness of therapies difficult.
Developed in 2008 by Carruthers et al ., the Merz Grading Scale, a 5-point photonumeric rating scale, attempts to objectively quantify the severity of aging of the hand by the degree of fatty tissue loss and the visibility of veins and tendons ( Fig. 42.7 ). This scale has demonstrated good inter- and intra-rater variability and has been validated for both photographic and live assessments. In 2016, Jones et al . reported the Allergan Hand Volume Deficit Scale, which sought to minimize subjective expressions of tendon and vein visibility, substituting the words “protruding” or “prominent,” rather than “mild” or “moderate”. More recently, in 2019, Lee et al . developed the Hand Volume Rating Scale to evaluate the outcomes of hand rejuvenation procedures by incorporating changes in skin texture due to hand volume changes. Though not specific to the hands, the Global Aesthetic Improvement Scale (GAIS) is also often used in the literature as an outcome measure. The 5-point scale reflects patients’ or providers’ subjective impressions, rather specific physical parameters, and rates improvement with categories of: “worse”, “no change”, “improved”, “much improved”, and “very much improved”.

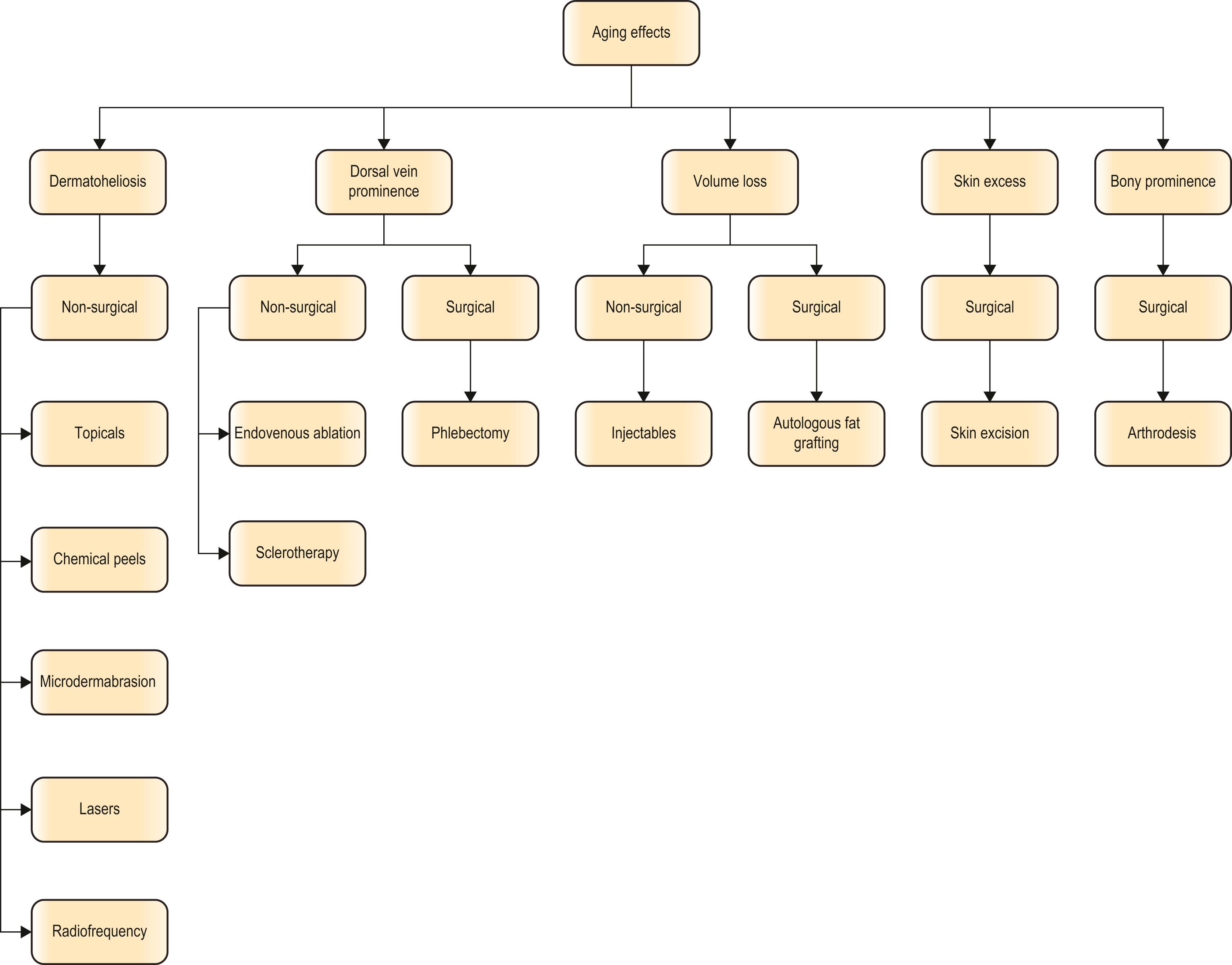
As aging is a multifactorial, three-dimensional process, a combination of both surgical and non-surgical techniques may be required for successful rejuvenation. Algorithm 42.1 demonstrates a decision algorithm for addressing the different characteristic signs of aging based on the desire for either a surgical or non-surgical approach.
The superficial appearance of the skin is one of the most noticeable signs of aging, and non-surgical management for rejuvenation of the skin can be highly effective. The majority of therapies, which include topical medications, chemical peels, microdermabrasion, lasers and radiofrequency ablation, induce superficial damage to the skin which in turn promotes neo-collagenesis. However, given the thinness of the skin and relative paucity of adnexal structures compared to other commonly resurfaced areas such as the face, the regenerative capacity of the skin is lessened. Treatments should be used cautiously as the dorsal hand skin is more prone to dyschromia and scarring.
Popular topical agents that can address the signs of photoaging include tretinoin, alpha-hydroxy acid, hydroquinone, vitamin C, alpha-lipoic acid, penta-peptide, and cutaneous growth factors. These serve to reduce the rate of melanin transfer in order to correct pigmentary abnormalities and simultaneously stimulate the production of collagen in the dermis. Although several multicenter, double-blind, placebo-controlled studies have demonstrated the effectiveness and safety of topicals for moderate to severe photodamage, none has specifically evaluated the effects on the aging hand. Nevertheless, they are a common first-line treatment.
Chemical peels are an economical approach for skin rejuvenation, primarily to address mild pigmentary changes, and can be classified as superficial, medium, or deep based on their depth of penetration into the epidermis and dermis. Superficial chemical peels penetrate to the level of the epidermis and include 70% glycolic acid, salicylic acid, 50% resorcinol, Jessner’s solution, and 10% to 25% tri-chloroacetic acid (TCA). Medium-depth peels penetrate to the level of the papillary dermis and include TCA peels at concentrations greater than 30%. Finally, phenol peels, classified as deep peels, penetrate to the level of the midreticular dermis, but should be avoided on the skin of the hand. Protocols for “light” medium-depth peels to be used in non-facial sites have been developed and can offer more effective results than their superficial counterparts.
Depending on the depth of the peel, various degrees of flaking and desquamation are to be expected in the 2 to weeks following the peel. Deeper peels carry more risk of scarring, dyschromia and prolonged erythema. Salicylism is rare with chemical peeling but can occur if large areas are treated with salicylic acid. In general, peels must be performed conservatively and serially over time until results are satisfactory, and outcomes are heavily dependent on concentration, contact time with the skin, and pre-peel preparation.
Microdermabrasion is another minimally invasive rejuvenation technique for skin resurfacing. It provides superficial exfoliation with mild to complete abrasion of the stratum corneum following treatment. Studies have shown epidermal thickening, decreased melanization and increased elastin deposition after treatments. The main advantage of microdermabrasion is that there is little to no downtime. However, multiple microdermabrasion procedures on the hands are recommended and the end result is often minimal improvement in skin smoothness, texture, and color.
Laser therapy is another noninvasive, cost-effective modality for skin resurfacing and multiple modalities have been reported for rejuvenation of the hand: Q-switched lasers, intermittent pulsed light (IPL), photodynamic therapy (PDT), 1320 nm neodymium-doped yttrium aluminum garnet (Nd: YAG) laser, fractionated 1550 nm erbium-doped laser, fractionated 1927 nm thulium laser, 2940 nm erbium-doped YAG (Er:YAG) laser, and fractionated 10,600 nm CO 2 laser. Given that recovery times after laser and light therapies are often longer than with facial skin and the risk of scarring is greater, treatment parameters including fluence, density, and number of passes should all be lowered to decrease the risk of adverse events. Table 42.1 compares different lasers with advantages and disadvantages of each.
| Laser | Advantages | Disadvantages | Number of sessions (4–6 week intervals) |
|---|---|---|---|
|
Most effective for pigmented lesions | Erythema, edema, dyschromia, scarring, PIH (particularly in darker skin types) | 1–2 |
|
Minimal recovery time, can treat both vascular lesions and solar lentigines, stimulates collagen production | Requires more sessions for improvement | 3–5 |
| Photodynamic therapy (using IPL) | Minimal recovery time | Erythema, edema, scaling | 2–3 |
| Non-ablative non-fractionatedNd:YAG (1320 nm) | Preserves epidermis so shorter recovery than ablative | Requires more sessions, mild improvement | 4–6 |
|
Preserves epidermis so shorter recovery than ablative | Mild improvement, erythema, edema and PIH | 1–3 |
|
Greatest degree of dermal remodeling | Longest recovery, highest risk of PIH, dyschromia, scarring | 1–3 |
As one of the most common complaints of the superficial appearance of the hand is pigmentary changes, lasers that target melanin can be particularly effective. The most common devices used are the Q-switched ruby laser (694 nm), Q-switched alexandrite laser (755 nm), and the Q-switched Nd:YAG laser (1064 nm) that deliver pulse durations in the nanosecond range, corresponding to the short thermal relaxation time of melanosomes. A single pass is typically performed with these lasers, but pulses may be stacked over macular seborrheic keratosis. The majority of epidermal pigmented lesions can be removed in one to two treatment sessions.
The Q-switched ruby laser has been demonstrated to be the most effective laser in removing epidermal pigmentation, although its use is not recommended in darker skin types. Darker skin types can be more safely treated, although not as effectively, using the 1064 nm Q-switched Nd:YAG laser. Adverse events for all skin types can include erythema, crusting, bleeding, and bullae formation, while the incidence of post-inflammatory hyperpigmentation (PIH) and post-inflammatory hypopigmentation is greater in darker skin types.
Strict sun protection and a broad-spectrum sunscreen is advised in all patients to minimize the incidence of complications, including PIH.
Intermittent pulsed light (IPL) therapy is a non-ablative photo-rejuvenating device that utilizes a high-intensity, noncoherent filtered flash-lamp light source, to emit light between 515 and 1200 nm. This broad spectrum facilitates the selective treatment of targets of varying absorption spectrum, and cut-off filters can be used to remove all wavelengths below a specified wavelength, allowing preferential selection of different targets and depths of penetration. Optimal correction of erythema and vascular lesions, with oxygenated hemoglobin as the target, can be achieved using 515 to 590 nm cut-off filters. Purpuric patches are better targeted with filters of 590 nm or higher. IPL systems should be less effective targeting melanosomes as they have pulse durations in the millisecond range, which is longer than the melanosome thermal relaxation time, but successful reports have been published demonstrating 50%–100% improvement in solar lentigines and ephelides after three to five treatment sessions. Fig. 42.8 demonstrates an example of improvement in pigmentation following IPL treatment. In addition to improvement in pigmentation, dermal heating from IPL therapy, which spares the epidermis, has been demonstrated histologically to induce collagen production in the papillary and reticular dermis.
 and 6 weeks following treatment with IPL (B) .")
Patients with lighter skin can be safely treated with a 560 nm filter, although darker skin types should be treated with a 590, 695 or 755 nm filters. In addition to variations in filter type, darker skin types should also be treated with lower energies and longer pulse durations to decrease the risk of dyschromia or scarring. Otherwise complications are rare and downtime after treatment is minimal.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here