Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124


 Access video and video lecture content for this chapter online at Elsevier eBooks+
Access video and video lecture content for this chapter online at Elsevier eBooks+
The abdominal wall is an important “organ”. It serves to protect the viscera and provides an important functional role with maintaining a pressurized core under which the lower extremities achieve locomotion and over which the thorax, upper extremities, and head are supported. Loss of continuity of the abdominal wall is an important issue, with hernia repair affecting hundreds of thousands of individuals and costing billions of dollars in direct and indirect costs. Despite the great interest and numerous conferences dedicated to abdominal wall closures, between 11% and 23% of laparotomy closures develop an incisional hernia and up to 40% hernia rates are documented in “high-risk” individuals such as the morbidly obese or abdominal aortic aneurysm patients. The rate of incisional hernia is greatly influenced by whether the hernia is detected radiographically (ultrasound, computed tomography) or clinically with a need for repeat surgery. Clinical rates of operative incisional hernia repair within 5 years after laparotomy are in the 3.8% range using large databases. As this remains an unsolved problem and the need is great, it behooves plastic surgeons to contribute to the knowledge and care of these patients.
Successful mastery of the field requires an understanding and working knowledge of:
Abdominal wall anatomy and physiology
Abdominal wall blood supply
Nerve supply and innervation of muscles
Muscle function
Abdominal wall tissue apposition
Midline laparotomy closure
Sutures, suture pull-through, meshes
Optimal midline closure
Abdominal wall defect repair
Umbilical and epigastric hernia
Incisional hernia
Need for mesh
Types of mesh
Mesh coatings, mesh placement, and fibrovascular ingrowth
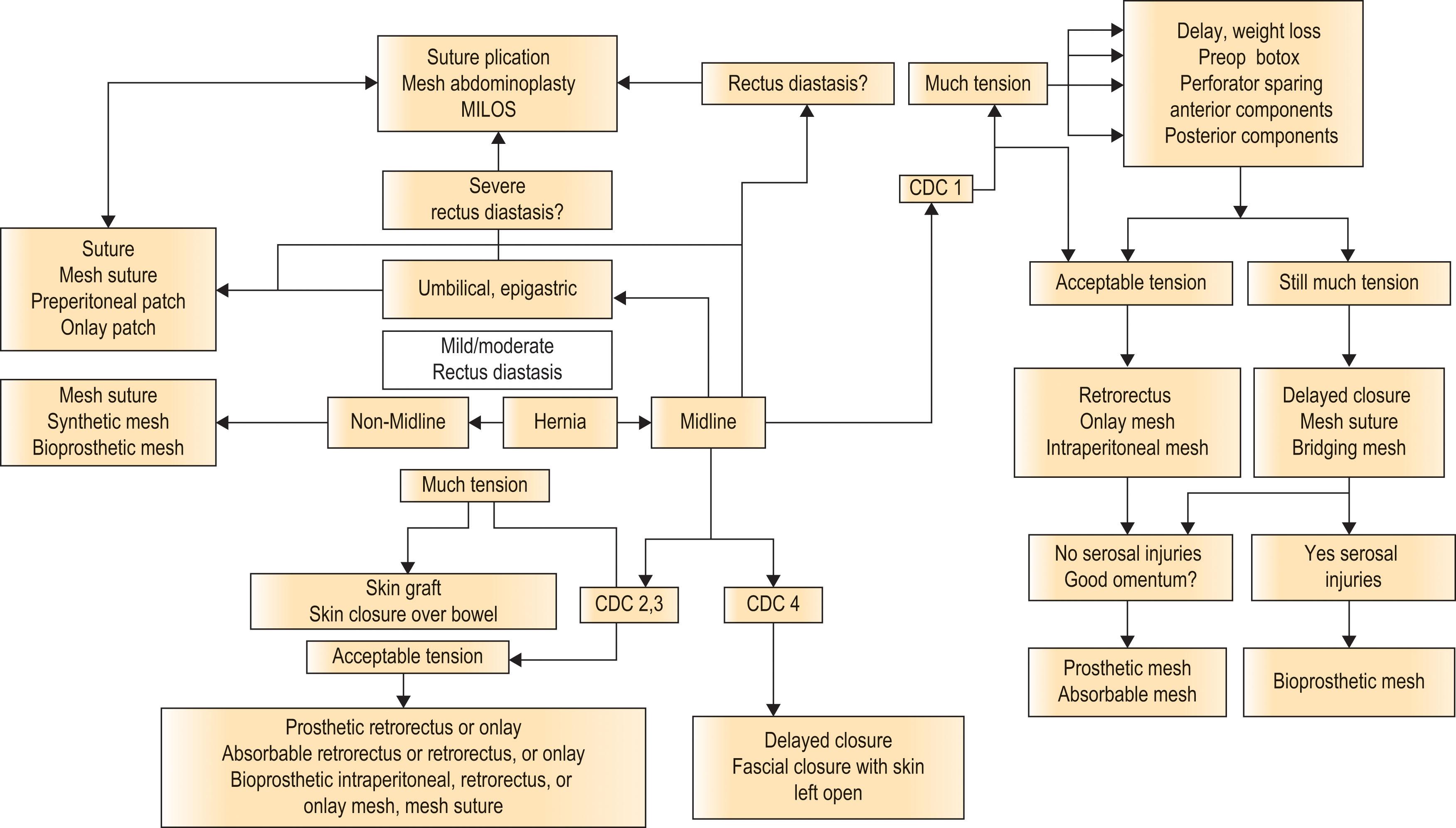
Optimal hernia closure (see Algorithm 13.1 )
Surgical technique for clean open midline incisional hernia repair
Surgical technique for clean midline incisional hernia repair under tension
Surgical technique for clean-contaminated, contaminated, and dirty midline hernias
Flank (non-midline) hernias
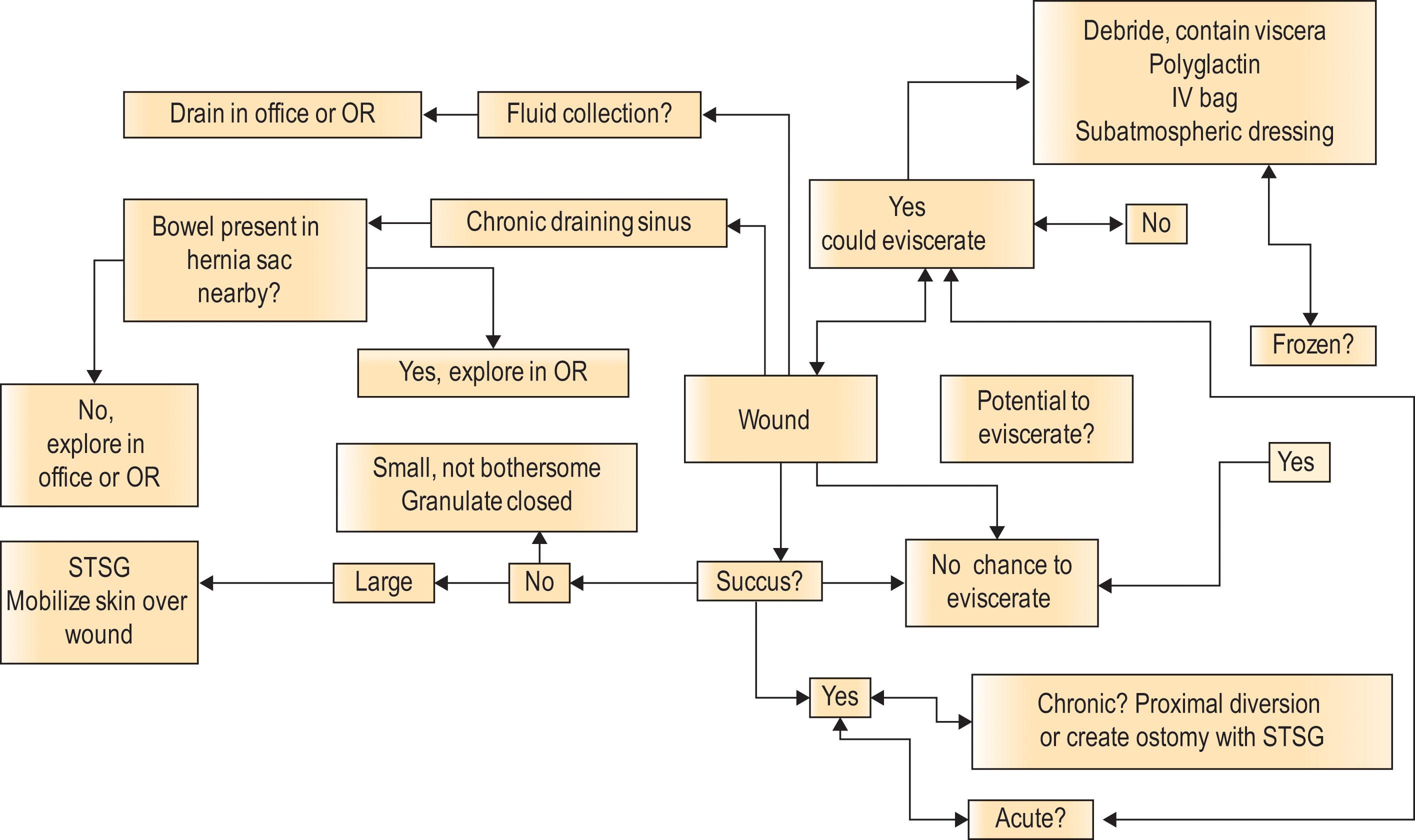
Abdominal wall soft-tissue management, wounds (see Algorithm 13.2 )
Plastic surgeons are uniquely situated to contribute to the care of these patients, based on our knowledge of anatomy, implants, and soft-tissue manipulation. In this chapter, we will present practical management strategies for the treatment of common abdominal wall conditions. In the course of learning about these individual conditions, we hope to provide an understanding and working knowledge of the necessary elements for successful abdominal wall reconstruction (AWR).
The abdominal wall anteriorly comprises eight muscles that envelop and protect the abdominal wall viscera. The paired rectus muscles originate at the symphysis pubis and insert onto the xyphoid. While the embryology of the lateral three muscles from somites is developmentally clear, the rectus muscles develop as condensations of somites. The embryology of the rectus muscle is complex and leads to the pediatric conditions of gastroschisis, omphalocele, and prune belly syndrome. There are three tendinous inscriptions per rectus muscle, and these fibrous bands exist at the level of the umbilicus, at the level of the xyphoid process, and one inscription midway between the two. The term “abdominal wall six-pack” should be an eight-pack, as the rectus muscles are noted to be each divided into four segments in muscular thin patients. These inscriptions are thought to prevent bowstringing of the muscle with contraction (much like the pulleys of the finger flexor tendon sheath), as well as aiding in forward flexion of the vertebral column.
Between the rectus muscles is the linea alba. This “white line” is a midline fibrous structure formed by the median fusion of the layers of the rectus sheath. Regarded as the “central tendon” of the abdominal wall, it joins the left and right hemi-abdomens to maintain appropriate sarcomere length for the eight abdominal wall muscles thereby optimizing function. In nulliparous women, the linea alba is approximately 1.1 cm wide at the level of the third vertebral body and increases to over 2 cm wide after childbirth ( Fig. 13.1 ). In men, the rectus muscles are separated by the linea alba from the xyphoid down to approximately 2–3 cm below the umbilicus where the muscles join. Significant rectus diastasis can occur with linea alba width of 8–10 cm in both men and women.

The semilunar lines exist between the lateral three abdominal wall muscles and the rectus muscles. These fascial condensations extend from the ninth rib cartilage towards the pubic tubercle. The location and prominence of the semilunar lines are interpreted as a sign of female abdominal wall beauty, as along with the linea alba these lines outline the rectus muscles.
The lateral three abdominal wall muscles allow twisting and forward flexion of the torso. The fibers of the external oblique and internal oblique muscles are oriented at almost 90 degrees to each other – conceptually akin to the bias-ply tire on automobiles. Bilateral external oblique contraction along with the rectus abdominis achieves flexion of the trunk, while ipsilateral external oblique and contralateral internal oblique contracture causes the trunk to twist. The transversus abdominis has a broad origin including the lower six costal cartilages, the thoracolumbar fascia, the iliac crest, and the lateral third of the inguinal ligament. With its insertion via a broad aponeurosis to the linea alba, it serves to increase abdominal pressure and support the abdominal viscera. Releases or incisions of either the external oblique muscle or the transversus abdominis muscle are common for complex AWR and will be discussed later in this chapter.
The abdomen is best thought of as a closed cylinder exposed to repeated bouts of elevated pressure. The bony pelvis is the bottom of the cylinder, and the retroperitoneum represents a firm and unyielding back wall of the cylinder. The diaphragm is a piston causing repeated bouts of elevated pressure within the abdomen. With each cough, Valsalva maneuver, and increase in core pressure, the viscera are compressed. As the bowel, omentum, and pre-peritoneal fat are mobile, these tissues naturally are pushed centrifugally toward areas of lower pressure. The lateral and anterior abdominal wall provide static and active centripetal force to contain the tissues. The static force is provided by unyielding fascia, while the active force is provided by muscle contraction that acts to stiffen the abdominal wall. Hernias develop when the static and active centripetal forces of the abdominal wall are no longer sufficient to contain the viscera. As the counterpressure outside the abdominal wall is low, hernias tend to enlarge over time. In the worst cases, there develops a loss-of-domain, as the intra-abdominal cavity loses its compliance and is no longer able to accept back the hernia contents. The importance of the pressurized cylinder concept of the abdominal wall can be illustrated with the closure of the abdomen after free flap breast reconstruction. Tightening of the lower abdomen raises intra-abdominal pressure that results in an epigastric bulging with decreased aesthetics.
Laplace’s law is important to understand when thinking about AWR. The pressure inside an inflated elastic container with a curved surface is inversely proportional to the radius. Continuing with the concept that the abdomen is a pressurized cylinder, the radius of the cylinder decreases from the epigastrium to the hypogastrium. By Laplace’s law, there is less tension on the abdominal wall near the symphysis pubis than adjacent to the xyphoid. This may in part explain the near 0% hernia risk for Pfannenstiel incisions after Cesarean section, as opposed to the difficulties seen with suture repairs of epigastric defects associated with rectus diastasis. Another example of the importance of Laplace’s law for the abdomen is at the time of extubation after laparotomy. The junior surgery resident “holds down” the incision so that forceful coughing will not increase the radius of the abdominal wall closure. By Laplace’s law, the increased radius raises the tension on the abdominal wall closure leading potentially to an abrupt dehiscence.
The blood supply to the abdominal wall comes from the deep inferior epigastric artery and the superior epigastric artery. The rectus muscles receive contributions from a third set of vessels that accompany the intercostal nerves. The lateral three abdominal muscles have a dual arterial system, being fed via segmental intercostal and lumbar perforators as well as the ascending branch of the deep circumflex iliac artery.
The abdominal skin blood supply has been intensely studied as this tissue is used for breast reconstruction. The lower abdominal skin is supplied via perforators of the deep inferior epigastric artery and the superficial epigastric artery that branch off the external iliac and common femoral arteries, respectively. A third supply to the lower abdominal skin is from the intercostal artery system and from a perforator from the deep circumflex iliac artery that emerges through the external oblique just posterolateral to the anterior superior iliac spine. The redundant blood supply allows for wide skin undermining common with AWR. In the upper abdomen, the skin is supplied by the superficial epigastric artery and segmental intercostals. Relative occlusion of the deep inferior epigastric artery from pressure created by the uterus in pregnancy serves to “delay” the lower abdominal skin and open communicating choke vessels. This episodic flap delay with pregnancy will later facilitate successful wide skin undermining for abdominoplasty.
A working knowledge of the abdominal blood flow is critical to successful AWR. As will be described, surgical procedures that utilize either an anterior or posterior component release require maintenance of skin perforators to avoid tissue necrosis. The anterior component release was regarded as an operation with high surgical site occurrence (SSO) rates due to the wide undermining required to release the external oblique muscle and fascia from the midline. As will be discussed, perforator preservation techniques maintain skin blood flow while still permitting the surgeon to perform the necessary releases.
Maintenance of the deep inferior epigastric artery branch that supplies the umbilical stalk and posterior sheath may encourage the rapid incorporation of a retrorectus mesh and preserve umbilical stalk viability. A prior surgical procedure (such as a large mesh overlay) may have interrupted the primary perforators supplying the skin, and so any subsequent operation with a new incision could jeopardize the secondary blood flow. A Cesarian section, an ostomy, or even an inguinal hernia repair may interrupt the deep inferior epigastric artery blood flow, and its patency needs to be confirmed before performance of a vertical rectus abdominis flap using a CT angiogram (CTA). Successful AWR requires the solution of two related but independent problems – how to manage the abdominal wall, and how to manage the skin. The latter requires a knowledge of past procedures, and occasionally a CTA or indocyanine green intraoperative angiography to ensure adequate skin healing.
The nerve supply to the abdominal wall and skin should be rather straightforward but instead has been shrouded in mystery in part due to difficult-to-remember nomenclature. Segmental nerves that emerge from T7 to L1 to supply the abdominal wall and skin are the thoracoabdominal nerves T7 to T11, the subcostal nerve (T12), and the three sensory branches that arise from L1 (iliohypogastric, ilioinguinal, and genitofemoral). The branches from T7 to T12 are mixed motor and sensory, while the L1 branches are pure sensory. The sensory component of the thoracoabdominal nerves travel through the rectus muscle and rectus fascia to innervate the anterior skin. “ACNES syndrome” is a compression neuropathy of the anterior sensory nerve branches as they emerge through the abdominal wall. Segmental sensory branches arise from the thoracoabdominal and subcostal nerves at the mid-axillary line to innervate the posterolateral and anterolateral abdominal wall.
Incisions that parallel the dermatomes spare the majority of the thoracoabdominal nerves, while abdominal incisions that are either transverse or even perpendicular to the dermatomes (such as a Kocher incision) will cut multiple thoracoabdominal nerves and cause a zone of denervation medial and inferior to the incision. The hallmark of abdominal wall denervation is a loss of thickness of the rectus abdominis muscle when compared to the contralateral rectus muscle by CT scan. True abdominal wall denervation can occur after full-thickness abdominal wall excisions for tumors. Spine pathology and “front/back” spine surgery can cause damage to the intercostal nerves. These true denervations can be compared to so-called “denervation bulges”, where a flank incision parallel to the dermatome line can result in a hernia of the internal oblique and transverse abdominis muscle, but with an intact external oblique. This condition is discussed in the section on non-midline hernias.
Abdominal incisional hernias occur after a sutured laparotomy closure where the tissues do not remain apposed. With the muscle no longer held out at length from failure at the linea alba closure site, all eight abdominal muscles are shortened and no longer at their physiologic appropriate length where sarcomere function is optimal. The Starling curve is critical in understanding abdominal wall muscle physiology at this point. A shortening of abdominal muscle length from an incisional hernia causes a weakening of the muscle due to sarcomere overlap and an inability to generate a maximal force. A loss of muscle function and strength from sarcomere overlap is one reason for a loss of abdominal core pressure with incisional hernia formation. In animal models, the internal oblique is noted to become shortened, stiff, and atrophic. Not only is muscle function not optimized, but there is also a change in energy consumption with large hernias. With abdominal wall contraction, rather than an isometric contraction where force is generated but the muscle does not change length, a large hernia allows isotonic contraction whereby the muscle shortens but tone is not increased due to the viscera emerging into the hernia sac. The energy consumption for isotonic contraction is much greater than that for isometric contraction due to the visible movement of the viscera and work being performed.
There are two types of hernia repairs, and they lead to different outcomes for long-term muscle function. Primary repairs of defects theoretically restore abdominal muscle length back to baseline, thereby optimizing the Starling curve and muscle function. The patching of defects with spanning (or bridging) mesh is termed a “tension-free repair”, and while this technique converts isometric contraction to isotonic contraction with a successful repair, it does not restore muscle length, thereby leaving the muscle permanently weakened from its pre-hernia state. Perhaps leaving the muscle a bit weak helps spanning meshes to remain intact by not pulling on the repair site as strongly. While animal data has supported the use of spanning meshes over primary repairs, human outcomes of decreased hernia recurrence rates with direct tissue repairs that are supported by a mesh have decreased the frequency of “tension-free” closure procedures.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here