Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

A 46-year-old woman, never smoker, with excellent performance status and otherwise healthy, with a new diagnosis of squamous cell carcinoma (SCC) from unknown primary stage T0N1 (as per the American Joint Commission on Cancer [AJCC] Staging Manual, 8th ed. ), p16 positive. She presented with a right cervical mass.
Computed tomography (CT) scan of the neck showed a 2-cm right cervical level IIA lymph node and no suspicious primary lesion. The patient underwent excisional biopsy revealing a 2-cm right level II node with no extracapsular extension. She then underwent a fluorodeoxyglucose-positron emission tomography/CT (FDG-PET/CT) followed by examination under anesthesia, diagnostic direct laryngoscopy, rigid esophagostomy, and random biopsies of the oropharynx, which failed to reveal a primary tumor site.
Her case was discussed at the multidisciplinary tumor board, and radical radiotherapy was the recommended treatment.
The patient was dispositioned to proton beam therapy (PBT) delivered as multifield optimization intensity-modulated proton therapy (IMPT) to a dose of 64 cobalt-Gray equivalent (CGE).
At the time of simulation, the patient was placed in the supine-neck extended position and aligned using external room lasers and a scout film. A mouth-opening/tongue-depressing stent was placed in the patient’s mouth for positioning and immobilization. A custom thermoplastic mask and headrest were created, and shoulder pulls were used to ensure reproducibility of setup for radiation treatments. A planning CT scan extending from the vertex to carina was obtained.
The case and contours were reviewed at the head and neck quality assurance meeting.
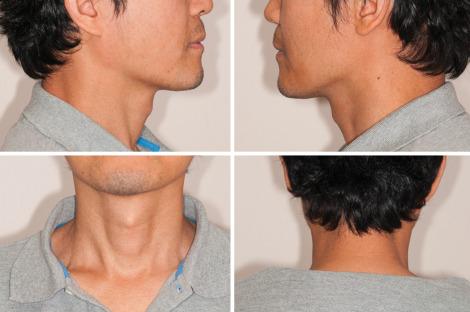
Baseline images of patient’s neck, oral cavity, and oropharynx
Treatment contours
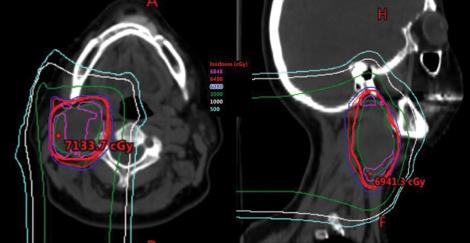
Treatment plan
Week 3 of treatment
End of treatment
The patient had the following toxic effects: fatigue grade 1, dermatitis grade 3, dry mouth grade 1, dysphagia grade 1, fatigue grade 1, and oral mucositis grade 1. The patient required narcotic pain medications.
Figure 8. Neck × 4 (ant/post/lat).
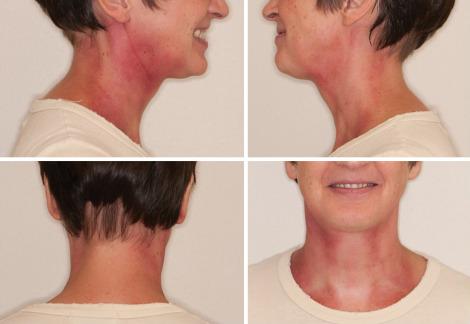
Figure 9. Oral cavity × 3 (lat tongue × 2/oropharynx).

2 months after treatment (first visit)
Grade 2 xerostomia. No dysphagia or dysgeusia. Thyroid function was normal.
FDG-PET/CT showed nonspecific findings for a level II lymph node. Fine-needle aspiration of this lymph node was negative.
Figure 10. Axial slice from fluorodeoxyglucose-positron emission tomography/computed tomography (FDG-PET/CT) showing nonspecific level II lymph node on PET.
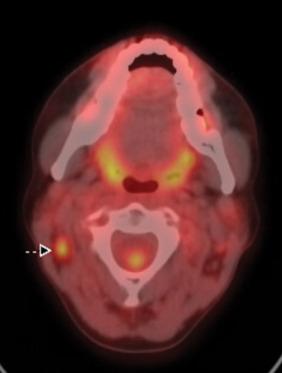
Figure 11. Neck × 4 (ant/post/lat)

Figure 12. Oral cavity × 4 (lat tongue × 2/oropharynx).

6 months after treatment
Patient is eating a regular solid diet without difficulty. Dry mouth is rated moderate with an XQ score of 69/80. Thyroid function tests are within normal limits.
Patient has no evidence of disease on physical examination or on imaging.
Figure 13. Neck × 4 (ant/post/lat)

Figure 14. Oral cavity × 4 (lat tongue × 2/oropharynx)

2 years after treatment
Patient is eating a regular solid diet without difficulty. Dry mouth is rated moderate with an XQ score of 30/80. Thyroid function tests are within normal limits.
Patient continues to have no evidence of disease on physical examination or on imaging.
Figure 15. Neck × 4 (ant/post/lat).

Figure 16. Oral cavity × 4 (lat tongue × 2/oropharynx).

A 38-year-old man with a history of stage T2N1 nasopharynx carcinoma treated 4 years ago with concurrent chemoradiation therapy to 70 Gy using intensity-modulated radiotherapy (IMRT). The patient presented with new-onset neck pain.
Computed tomography (CT) scan and magnetic resonance imaging (MRI) of the head and neck showed recurrence at the skull base in the region C1 cervical spine. Fluorodeoxyglucose-positron emission tomography/CT (FDG-PET/CT) showed no site recurrence, regionally or distantly.
The case was presented at the multidisciplinary tumor board, where induction chemotherapy followed by consolidation (chemo)-radiotherapy was recommended. The patient underwent four cycles of induction chemotherapy, with good response.
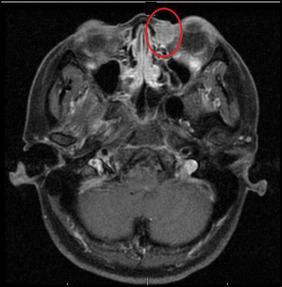
Figure 1. Axial slice from preinduction contrast-enhanced magnetic resonance imaging showing recurrent lesion at the left skull base.

Considering the proximity of the recurrent lesion to the brainstem and previously irradiated nasopharynx mucosa, the patient was considered a good candidate for proton beam radiotherapy to minimize the risks of severe toxicity. The patient was treated to a dose of 66 cobalt-Gray equivalent (CGE) with concurrent chemotherapy using three-field intensity-modulated proton therapy (IMPT).
At time of simulation, the patient was placed in the supine position. A wedge pillow was placed under his knees for comfort. His shoulders were retracted. A bite block was inserted. A CT scout image was obtained to verify alignment. Once alignment had been verified, a custom mask was placed over the head and shoulders. The isocenter was placed at the level of C1 in the midline. A planning CT scan extending from the vertex to carina was obtained.
The patient was examined, and the case and contours were reviewed at the head and neck quality assurance meeting.
Baseline images of patient’s neck, oral cavity, and oropharynx
Treatment contours
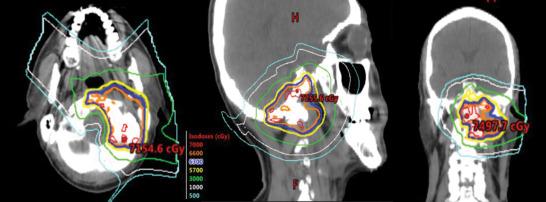
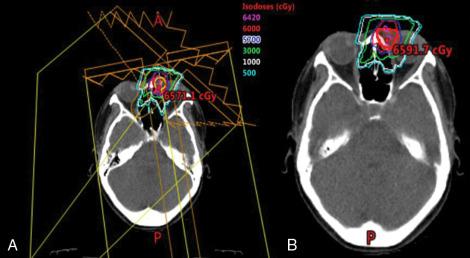
Treatment plan
Week 3 of treatment
End of treatment
2 months after treatment (first visit)
6 months after treatment
1 year after treatment
No fatigue. Resolution of “ear stuffiness.” No dysphagia, no pain, no xerostomia.
2 years after treatment
New hypoglossal, vocal fold, and hemipharyngeal paresis associated with dysphagia, but airway protection maintained. Magnetic resonance imaging findings showed no evidence of local-regional recurrent disease; new deficits attributed to radiation-induced neuropathy. Plan for swallowing study and rehabilitation for cranial neuropathy.
A 57-year-old woman with paraganglioma of the right neck found incidentally and followed by imaging over a 4-year period. Follow-up imaging revealed slow progression of the lesion. The patient reported occasional throbbing sensation in the neck and tongue but had no vasomotor symptoms, dysphagia, or dysphonia.
Treatment options including further observation, surgery, or radiotherapy were discussed. The case was presented at the multidisciplinary tumor board. Given the significant risks of vagal and hypoglossal nerve injury associated with surgery, radiotherapy was the recommended treatment option.
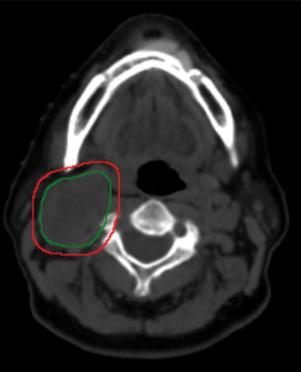
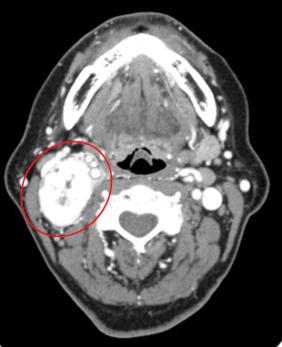
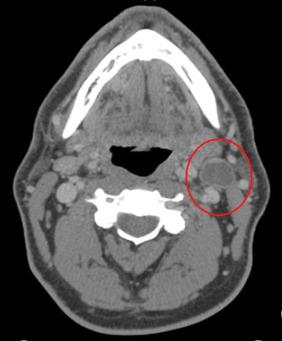
Figure 1. Axial slice from diagnostic computed tomography (CT) scan of the neck showing a right neck paraganglioma.
The patient was dispositioned to proton beam therapy (PBT) delivered as three-dimensional conformal proton beam therapy to a dose of 64 cobalt-Gray equivalent (CGE) in 32 fractions.
At time of simulation, the patient was placed in the supine-neck extended position and aligned using external room lasers and a scout film. A bite block was placed in the patient’s mouth for positioning and immobilization. A custom thermoplastic mask and headrest were created, and shoulder pulls were used to ensure reproducibility of setup for radiation treatments. The isocenter was placed at above the arytenoid level. A planning CT scan extending from the top of the orbits to the carina was obtained.
The case and contours were reviewed at the head and neck quality assurance meeting.
Baseline images of patient’s neck, oral cavity, and oropharynx
Treatment contours
Treatment plan
Week 3 of treatment
The patient developed the following toxic effects: fatigue grade 1, oral mucositis grade 0, dysphagia grade 1, nausea grade 0, dermatitis grade 1. No pain medication.
End of treatment
The patient had the following toxic effects: fatigue grade 2, dysphagia grade 1, nausea grade 0, dermatitis grade 3. No pain medication.
2 months after treatment (first visit)
6 months after treatment
Patient reports occasional neck stiffness. Sharp pain resolved. Alopecia in posterior occipital region.
No nausea or vomiting, eating regular diet. No cranial nerve deficits. No vasomotor symptoms. No dysphonia or dysarthria. No xerostomia. Thyroid function normal.
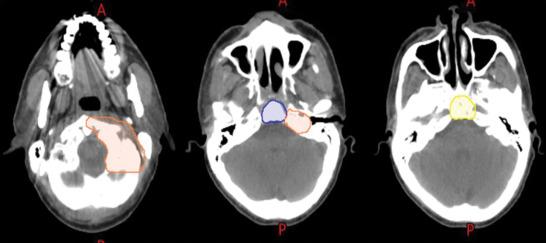
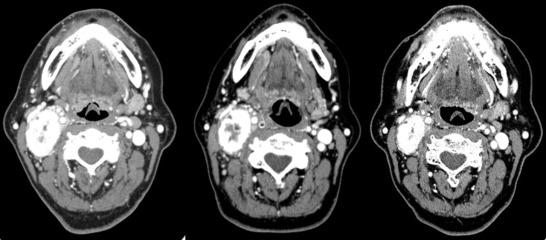
Figure 6. Axial computed tomography scans show reduction in size of paraganglioma from before treatment (left) to 6 months after treatment (middle) to 5 years after treatment (right).

18 months after treatment
2 years after treatment
3 years after treatment
5 years after treatment
A 46-year-old woman with left-lacrimal-sac squamous cell carcinoma (SCC). The patient had noted a lesion at the medial aspect of the left eye as well as excessive tearing from the left eye at 3 months before presentation..
Magnetic resonance imaging (MRI) of the orbit revealed an enhancing soft tissue mass in the left nasal lacrimal duct of 1.6 × 1.4 cm. There was no evidence of cervical adenopathy on head and neck scan. Dacryocystectomy (resection of tumor mass and left larcimal sac with frozon section control of margins) was performed along with excision of the medial aspect of the upper and lower eyelid. Pathology confirmed SCC of the lacrimal sac with involvement of the bone and the lacrimal gland.
After discussion at the multidisciplinary tumor board, postoperative radiotherapy to the operative bed and nasal duct was recommended.
Figure 1. Axial slice from preoperative magnetic resonance imaging showing the lesion at the left lacrimal sac region.
The patient was dispositioned to receive radical proton therapy with a three-dimensional (3D) conformal technique to a dose of 60 cobalt-Gray equivalent (CGE) in 30 fractions.
At the time of simulation, the patient was placed in the supine-neck extended position and aligned using external room lasers and a scout film. A bite block was placed in the patient’s mouth for positioning and immobilization. A custom thermoplastic mask and headrest were created, and shoulder pulls were used to ensure reproducibility of setup for radiation treatments. The surgical scar was wired. Isocenter was placed at the level of the tumor bed. A planning computed tomography (CT) scan extending from the top of the orbits to the carina was obtained.
The case and contours were reviewed at the head and neck quality assurance meeting.
Baseline images of patient’s face
Treatment contours
Treatment plan
Week 3 of treatment
End of treatment
2 months after treatment (first visit)
6 months after treatment
12 months after treatment
’
2 years after treatment
The patient developed epiphora of the left eye. No recurrence.
3 years after treatment
Resolution of left eye epiphora. Vision unchanged. No recurrence.
A 47-year-old man with T2N1 left tonsil squamous cell carcinoma (SCC), p16 positive, never smoker presented with a 1-year history of sore throat and a growing mass in the left tonsil.
He underwent a diagnostic tonsillectomy at outside institution which revealed p16-positive SCC, 2 cm with negative margins. A computed tomography (CT) scan revealed a level IIA cystic lymph node measuring 3 cm.
The case was discussed at the multidisciplinary tumor board, and unilateral radical radiotherapy was the recommended treatment.
Figure 1. Axial slice from computed tomography scan of the neck after left tonsillectomy showing no residual gross disease at the left tonsil and left level IIA lymph node.
The patient was dispositioned to receive radical proton therapy delivered as three-field intensity-modulated proton therapy (IMPT) to a dose of 66 cobalt-Gray equivalent (CGE) in 30 fractions to the left tonsil and ipsilateral neck.
At the time of simulation, the patient was placed in the supine-neck extended position and aligned using external room lasers and a scout film. A bite block was placed in the patient’s mouth for positioning and immobilization. A custom thermoplastic mask and headrest were created, and shoulder pulls were used to ensure reproducibility of setup for radiation treatments. The surgical scar was wired. Isocenter was placed at the level of the tumor bed. A planning CT scan extending from the top of the orbits to the carina was obtained.
The case and contours were reviewed at the head and neck quality assurance meeting.
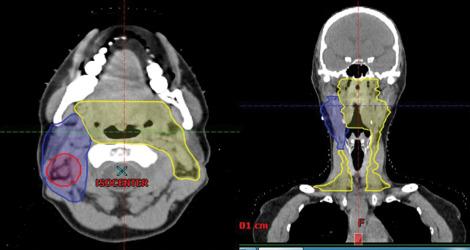
Treatment contours
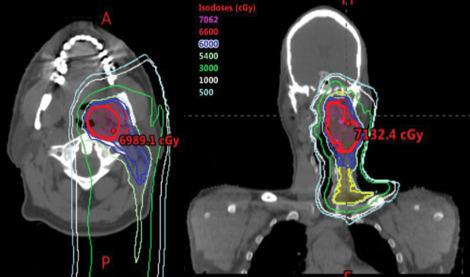
Figure 2. Axial and coronal slices showing clinical target volumes (CTVs). High-dose CTV treated to 66 cobalt-Gray equivalent (CGE) in 30 fractions to the tonsillar bed and involved lymph node (red), intermediate-dose CTV treated to 60 CGE in 30 fractions (retropharyngeal and ipsilateral level III; blue ), and elective CTV treated to 54 CGE in 30 fractions ( yellow ).

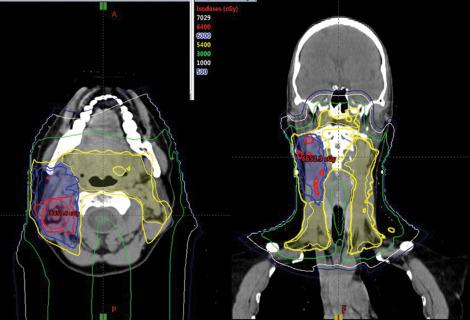
Treatment plan
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here