Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Central nervous system (CNS) tumors are the second most common pediatric cancer diagnosed each year, accounting for approximately 25% of childhood cancers. They are responsible for the second most common cause of cancer deaths in children.
Survival has slowly improved over the years, and overall survival is now approximately 75%.
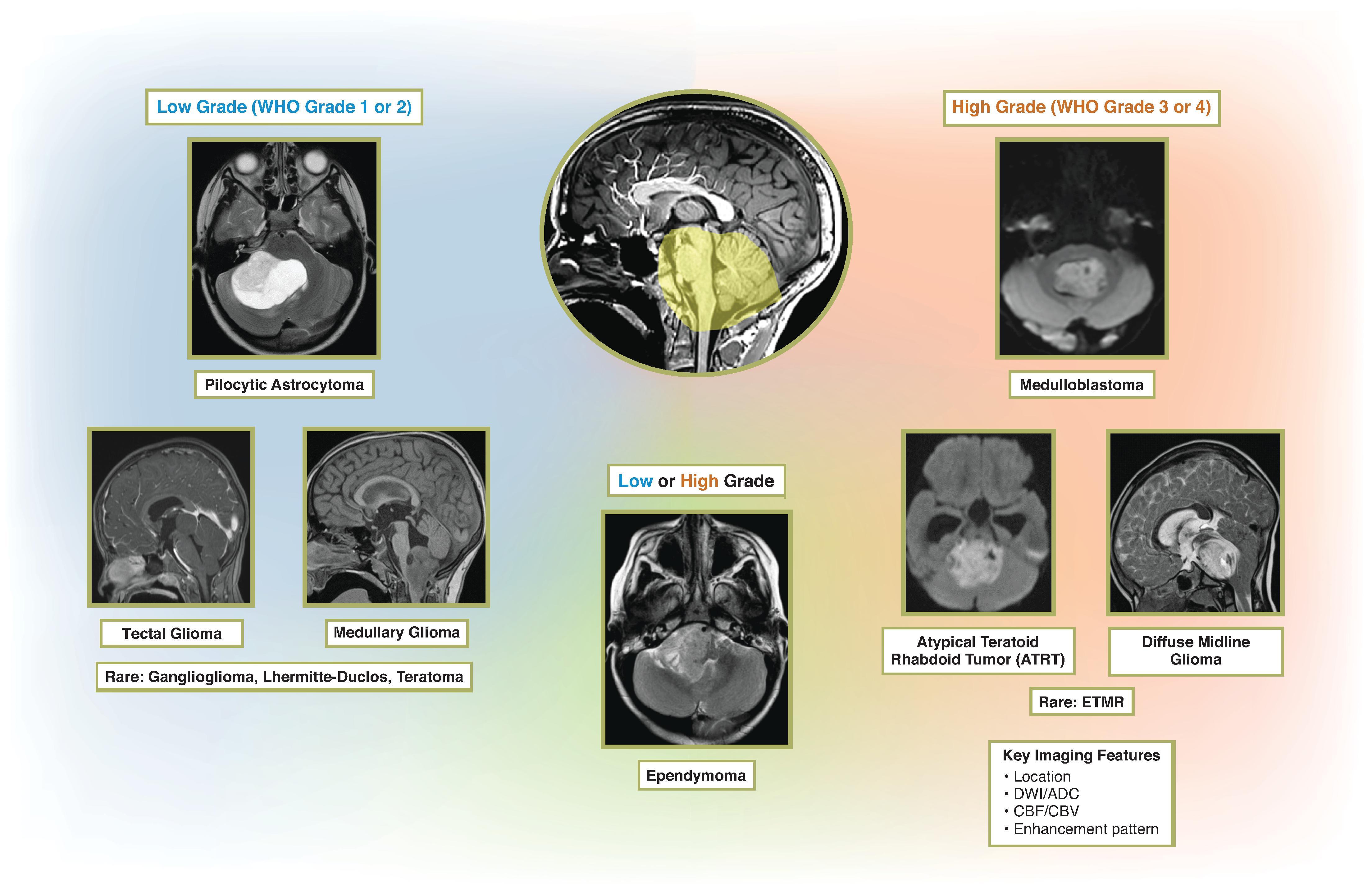
Supratentorial tumors predominate during the first 2 years of life and late adolescence, while infratentorial tumors are more common in the remainder of the first decade.
Presenting signs and symptoms are wide ranging, but common features include headache (especially morning headache), vomiting, lethargy, papilledema, seizure, and neurologic deficit. Some signs and symptoms are more specific to a location of tumor and are emphasized in this chapter.
Treatment varies, depending on the tumor pathology and location, and is briefly discussed in each section.
Imaging is performed for obtaining a diagnosis or differential diagnosis, determination of tumor extent, and effect on the normal brain. Follow-up imaging is used to assess for recurrence/progression and complications of treatment.
A general approach for a new pediatric brain tumor for determining the diagnosis or narrow differential diagnosis includes the following:
Location and extent of the tumor: This chapter emphasizes a location-based approach
Conventional MRI appearance with emphasis on DWI appearance
Advanced imaging: MR Spectroscopy (MRS), Arterial Spin Label (ASL) perfusion, Dynamic Contrast Enhanced (DCE) perfusion, and Dynamic Susceptibility Contrast (DSC) perfusion
Determination of leptomeningeal disease in the remainder of the brain and spine
DWI is helpful for determining low grade (WHO grade 1–2) from high grade (WHO grade 3–4). High-grade tumors typically demonstrate DWI hyperintense and ADC hypointense signal relative to normal parenchyma, which is considered a reflection of tumor cellularity (low ADC = high cellularity).
MR perfusion imaging is helpful for tumors in which the conventional imaging patterns remain inconclusive. Generally, high cerebral blood flow (CBF) and cerebral blood volume (CBV) occur in high-grade tumors and are reflective of tumor microvascular density. An ASL CBF > 50 mL/min/100 g was shown to have sensitivity/specificity for differentiation of low-grade and high-grade pediatric brain tumors at the following locations: cerebral hemisphere (90%/93%), thalamic tumors (100%/80%), and posterior fossa tumors (65%/94%). Determination of specific histopathology remains challenging.
MRS can be useful when the convention pattern is indeterminate. However, the authors believe the conventional imaging patterns combined with MR perfusion have rendered MRS less favorable in the initial imaging of pediatric brain tumors. Utility may remain in situations of determining radiation necrosis from recurrent tumor.
WHO grade 4
Account for 30% to 40% of pediatric posterior fossa tumors
Five histologic subtypes:
Classic: Most common (>70%)
Desmoplastic/nodular
Large cell
Anaplastic
Medulloblastoma with extensive nodularity
Molecular subgroups better correlate with demographics, clinical features, and prognostication and may aid development of future molecular targeted therapies
Four molecular subgroups—prevalence:
Wingless (Wnt): 10%
Sonic Hedgehog (SHH): 30%
Group 3: 25%
Group 4: 35%
Gorlin syndrome (basal cell nevus syndrome) is associated with increased risk of medulloblastoma and discussed in Chapter 9 .
Midline (most common) or cerebellar hemispheric hyperdense tumor; commonly cysts or necrotic regions (50% to 90%); calcifications (10% to 40%); significant hemorrhage is uncommon
Most commonly arising from the inferior vermis, although location may be variable depending on molecular subtype
Well-circumscribed; T1W hypointense; T2W isointense to hypointense
Variable enhancement with majority demonstrating enhancement. Minority may show no enhancement
Restricted diffusion with ADC values <0.9 × 10 3 mm 2 /s
Metastatic disease at initial diagnosis in 11% to 43%
Posterior fossa, intraventricular, subfrontal, and spinal are most common locations for metastases
MR Perfusion: ↑ CBF and CBV
MRS: ↑ Elevated taurine , choline, and lactate; ↓ NAA and creatine

")
 |
 |
 |
 |
|
| Wnt | Sonic Hedgehog | Group 3 | Group 4 |
Prevalence: 10% (rarest subgroup)
Histology: Classic
Prognosis: 5-year survival 95% (best prognosis)
Demographics: Older children and teens ; M:F ratio 1:1
Location: Lateral location (foramen of Luschka, cerebellopontine angle [CPA]) ; is most common fourth ventricle, or cisterna magna are less common
Rarely presents with metastasis
Prevalence: 30%
Histology: Desmoplastic/nodular and classic are most common; large cell/anaplastic possible
Prognosis: 5-year survival 75% (intermediate prognosis)
Demographics: Infants and teenagers/adults; M:F ratio 1:1
Location: Vermis (infants), or cerebellar hemisphere (teenagers/adults)
Rarely presents with metastasis
Prevalence: 25%
Histology: Classic, large cell/anaplastic
Prognosis: 5-year survival 50% (poor prognosis)
Demographics: Infants and children; M:F ratio 2:1
Location: Midline (vermis, fourth ventricle)
Enhancement in majority of tumors
Higher risk of presentation with metastasis
Prevalence: 35% (most common)
Histology: Classic, large cell/anaplastic
Prognosis: 5-year survival 75% (intermediate prognosis)
Demographics: Infants, children, and adults; M:F ratio 3:1
Location: Midline (vermis, fourth ventricle)
Less enhancement
Higher risk of presentation with metastasis
WHO grade 1
Accounts for 25% to 35% of pediatric posterior fossa tumors
Most tumors are sporadic in origin. Most tumors have the BRAF gene mutation leading to activation of the RAS/ERK/MAPK pathway
Neurofibromatosis type I associated with increased risk of pilocytic astrocytoma (typically optic gliomas; rarely posterior fossa)
95% 5-year survival; prognosis dependent on extent of resection
Location: Cerebellar hemispheric (most common) or posterior fossa midline, optic pathway/hypothalamus, thalamus and cerebral hemisphere
Fluid density cysts and isodense or hypodense solid portion; dominant cyst with small iso- to hypodense solid component (most common); may have a small cystic component or entirely solid.
Calcifications; hemorrhage is uncommon at presentation.
Solid and cystic (commonly a cyst and nodule pattern ); well-circumscribed; fluid signal intensity or complex fluid signal intensity cystic component; T1W-hypointense, T2W-hyperintense solid component with intense enhancement; cyst wall may enhance but can be reactive rather than indicate tumor presence
Usually ADC hyperintense compared to normal brain; ADC values >1.4 × 10 3 mm 2 /s
Uncommonly metastasize, but possible
MR perfusion: Variable CBF and CBV; often leaky blood-brain barrier which can lead to a T1 leakage pattern on DSC perfusion images characterized by the signal intensity rising above baseline after the contrast bolus has arrived
MRS: Aggressive metabolite pattern with ↑ choline and lactate, ↓ NAA and creatine. Can be misleading to diagnosis of a high-grade glioma
WHO grade 2–3
Accounts for approximately 20% of pediatric posterior fossa tumors
Molecular subgroups
EPN_PFA (80%): Infants and young children; poor prognosis ; reduced trimethylation of H3K27
EPN_PFB: Older children and adolescents; better prognosis; increased levels of trimethylation of H3K27
Subependymoma
Neurofibromatosis type 2 (NF-2)–associated with increased risk of ependymoma
7-year survival is 65%; prognosis dependent on extent of resection, tumor grade, and molecular subtype
Location: Floor of the fourth ventricle with projections of tumor and through the foramen Magendie and foramina of Luschka
Isodense-hyperdense; well-defined; calcifications more common than any other posterior fossa tumors; small cysts and hemorrhage may occur
Well-circumscribed; T1W hypointense, T2W iso- to hyperintense; variable enhancement
Intermediate ADC signal (usually isointense compared to normal brain ) between medulloblastoma and pilocytic astrocytomas with ADC values ∼1.0-1.3 × 10 3 mm 2 /s
Metastasis uncommon, but increased risk with higher grade, and younger age
MRS: ↑ Myoinositol , choline, and lactate; ↓ NAA
MR perfusion: ↑ CBF and CBV
WHO grade 4
SMARCB1 mutations
Rhabdoid tumor predisposition syndrome (RTPS) associated with increased risk of ATRT
Dismal prognosis in patients <3 years of age (most common age group is <3 years)
Location: Cerebellar, vermian/fourth ventricular , supratentorial (older patients)
Hyperdense heterogeneous mass, small cysts, necrosis, hemorrhage, and calcification may occur
Well-circumscribed heterogeneous mass, T1W isointense, T2W isointense, variable enhancement, small cysts, necrosis, hemorrhage and calcification
Restricted diffusion similar to other embryonal tumors
Metastasis common at presentation (>20%)
MR perfusion: ↑ CBF and CBV
MRS: Aggressive metabolite pattern with ↑ choline, lipid and lactate; ↓ NAA
Embryonal tumor with multilayered rosettes (ETMR) is a WHO grade 4 tumor recently classified in 2016 as tumors with amplification or gain of the C19MC region on chromosome 19 (19q13.42). This now includes tumors previously known as embryonal tumor with abundant neuropil and true rosettes (ETANTR), ependymoblastoma, and in some cases medulloepithelioma
Median age at presentation <3 years
Poor prognosis; median survival is 8 months
Location: Both supratentorial (cerebral hemisphere) and infratentorial locations (along the tentorium, cerebellar vermis, fourth ventricle, and brainstem)
Variable density with 50% hyperdense; hemorrhage and calcification (67%)
Large, well-circumscribed, homogeneous, T2W hyperintense, minimal enhancement, and minimal to no surrounding edema
Restricted diffusion similar to other embryonal tumors (median ADC 728 mm 2 /s)
Leptomeningeal disease uncommon
MR perfusion:
↓ CBF (median 30 mL/min/100g; unusual for high-grade tumors and different than what is seen typically with ATRT and medulloblastoma)
↑ CBV (maximal rCBV 3.5–5.8; mean rCBV 1.7–2.7)
MRS: Limited data indicate ↑ choline and taurine
Also known as Lhermitte-Duclos. WHO grade 1
May be associated with hemimegalencephaly or hemihypertrophy syndromes
Cowden syndrome associated with increased risk of dysplastic cerebellar gangliocytoma
Location: Cerebellar hemisphere; may extend into vermis
Ill-defined hypodense mass; hemorrhage and calcification may occur
Well-circumscribed heterogeneous striated mass “enlarging the regional cerebellum,” also known as “corduroy appearance” with significant mass effect. Bands of alternating T2W hyper- and hypointense signal; areas of cystic change; most do not enhance but may have regions of enhancement; hemorrhage and calcification may occur.
Lack of restricted diffusion.
MR perfusion: Regions of ↑ rCBV
MRS: ↑ Lactate; ↓ NAA and myoI
Low-grade : WHO grade 1 (dorsally exophytic), WHO grade 2 (diffuse)
Three subtypes:
Dorsally exophytic (pilocytic astrocytoma, ganglioglioma)
Diffuse infiltrating (fibrillary astrocytoma)
NF -1–associated focal gliomas (pilocytic astrocytoma)
Prognosis better in dorsally exophytic and NF-1–associated gliomas compared to diffuse infiltrating
Location: Medulla or cervicomedullary
Hypodense mass
Dorsally exophytic
Well -circumscribed, multilobulated T1W hypointense, T2W hyperintense, variable enhancement, and small cysts
Lack of restricted diffusion
Dorsally exophytic with involvement of the medulla
Diffuse infiltrating (fibrillary astrocytoma)
Less well -defined T1W hypointense, T2W hyperintense, and variable enhancement
Lack of restricted diffusion
Infiltrative expansion of the medulla
NF-1–associated focal gliomas (pilocytic astrocytoma)
Focal , and usually small; well-defined; T1W hypointense, T2W hyperintense, and variable enhancement
MR Perfusion: decreased CBV and CBF
MRS: varies based on histology
High-grade: WHO grade 3–4
H3K27M mutation (histone H3 lysine27-to-methionine mutation) is present in 70%
Term DIPG (diffuse intrinsic pontine glioma) no longer officially is used
The pons is the most common location of brainstem tumors
Signs and symptoms include hyperreflexia, ataxia, and cranial neuropathies (particularly abducens palsy). Behavior and cognitive changes also may occur
Poor prognosis. Median survival is 9 to 11 months
Location: Midline pons but may extend into the cranial and caudal brainstem and even into the cerebellum and supratentorial brain at end stage
Hypodense expansile mass of the pons
Poorly circumscribed T1W hypointense, and T2W hyperintense infiltrative expansile mass; mostly nonenhancing . May have regions of focal or cystic necrotic peripheral enhancement. Commonly effaces the prepontine cistern and encases or partially encases the basilar artery
Lack of restricted diffusion, although higher-grade components, which commonly enhance, may have restricted diffusion
End stage may metastasize or rarely at presentation
MR perfusion: Typically, low CBF and CBV at presentation with exception of enhancing areas; postradiotherapy demonstrates increased CBF
MRS: ↑ Elevated choline, lactate & lipid; ↓ low NAA
WHO grade 1 (most commonly pilocytic astrocytoma)
Obstruction of cerebral aqueduct leads to hydrocephalus and presentation
Most managed with third ventriculostomy
Excellent prognosis
Location: Tectal plate; may extend into the adjacent tegmentum and thalami
Hypodense expansile mass of the tectum
Well-defined T1W hypointense, and T2W hyperintense expansile tectal mass; often nonenhancing, but may enhance. Effaces the cerebral aqueduct
Lack of restricted diffusion
MR Perfusion: decreased CBV and CBF
MRS: not routinely performed
WHO grade 1
Peak incidence in the second decade of life; affects more M>F
Presentation with intractable seizures
Mixed glioneuronal tumor that may be associated with focal cortical dysplasia (type IIIB)
5-year survival >95%
Location
Hemispheric tumor in the cortex and subcortical white matter, especially the temporal lobe, but they can occur anywhere. Rarely arise in the brainstem, cerebellum, and basal ganglia.
Nearly always solitary; rarely multifocal
Well-defined hypodense mass without hemorrhage. Calcifications may occur. Small lesions may be entirely missed. Scalloping of the overlying calvarium can occur and suggests slow growing and lengthy presence of the mass.
T1W hypointense, T2W hyperintense “bubbly” lesion due to cystic or microcystic appearance of the tumor. Nodular or diffuse appearance may also be seen. Peripheral rim of T2 FLAIR signal may be present. Some have a triangular configuration, especially larger mass lesions.
Most commonly nonenhancing but up to one-third will have small areas of nodular, ring-like, or heterogeneous enhancement. Absent peritumoral edema and little to no mass effect.
Facilitated diffusion.
MR perfusion: ↓ rCBV
MRS: normal or ↑ myoI
WHO grade 1 (low grade), grade 2 (atypical), and grade 3 (anaplastic). May progress to grade 4.
Median age of 12 years; male predominance
Neoplastic neuronal elements and astrocytes
Similar imaging appearance to gangliocytomas, pilocytic astrocytomas, oligodendrogliomas, and DNETs
85% associated with seizures ; reported to be the most common cause of chronic temporal lobe epilepsy
Survival 98% at 7.5 years
Location
Temporal , especially mesial temporal followed by frontal. May rarely occur intraventricular or in brainstem, cerebellum, or spinal cord. Cerebellar gangliogliomas are reported to have unusual associated atrophy of the ipsilateral cerebellar hemisphere.
Small lesions will be easily missed by CT. Hypodense mass; calcification is common; hemorrhage is uncommon
Variable appearance
Typically, T1W hypointense and T2W hyperintense variably enhancing solid mass with or without cysts. Lesions within the mesial temporal lobe; however, may be primarily solid, poorly delineated with little enhancement.
Increased ADC ; higher-grade lesions may have lower ADC
MR perfusion: ↓ CBV and CBF
MRS: ↓ NAA, ↑ myoI
WHO grade 2 (low grade) and grade 3 (anaplastic)
1% to 3% of pediatric CNS neoplasms
Rare entity in children compared to adults ; peak incidence is fifth to sixth decade
Uncommon to have 1p19q deletion or IDH1 mutation which is different from adult patients; MGMT promoter methylation is similar to adult patients
Excellent prognosis; 5-year survival 95%
Location
Typically, hemispheric, cortical and subcortical tumor. Frontal lobe is most common followed by parietal and temporal lobe. Rarer locations include brainstem, cerebellopontine angle, optic nerve, and spinal cord.
Small lesions will be easily missed by CT. Hypodense peripheral mass; calcification may be seen but less common than in adults; hemorrhage is uncommon
Well-defined T1W hypointense and T2W hyperintense; nonenhancing to minimally enhancing solid mass with or without cysts; can also be poorly delineated with little enhancement.
Increased ADC, even in high-grade lesions
MR perfusion: Variable but potential for ↑ CBV/CBF
MRS: ↑ Choline, lactate, and lipid in higher-grade lesions and thus may be more helpful than dynamic susceptibility perfusion imaging
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here
