Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Talus : talar dome osteochondral lesion; neck of talus fracture; medial or lateral process fractures. Calcaneum : acute fracture; stress fracture.
Syndesmotic widening (tear of tibiofibular membrane).
Base of 5th metatarsal fracture.
Ankle : AP mortice (20° internal rotation) and Lateral . Sometimes a Straight AP .
Calcaneal injury : an additional Axial .
AP, anterior-posterior; AVN, avascular necrosis; CT, computed tomography; MT, metatarsal; RTA, road traffic accident.
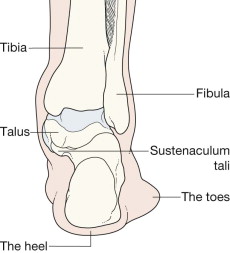
The lateral and medial malleoli can be identified. Helpful hints to aid identification:
The lateral malleolus extends more inferiorly than the medial malleolus.
The medial malleolus has a notch inferiorly.
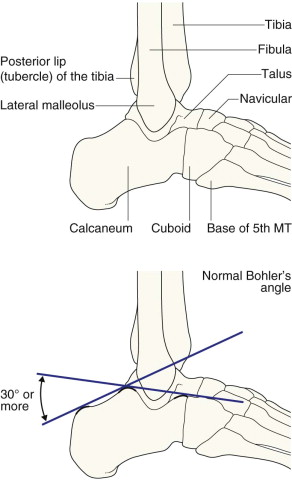
The posterior lip (or tubercle) of the tibia, conventionally and inaccurately referred to as the posterior malleolus, is well shown.
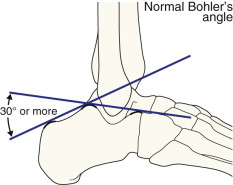
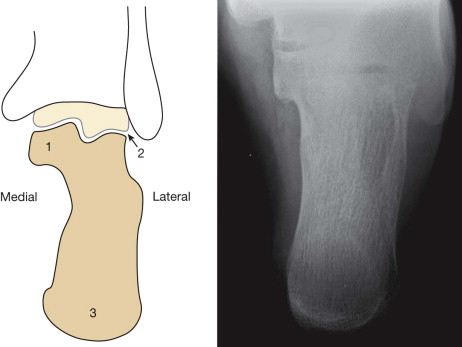
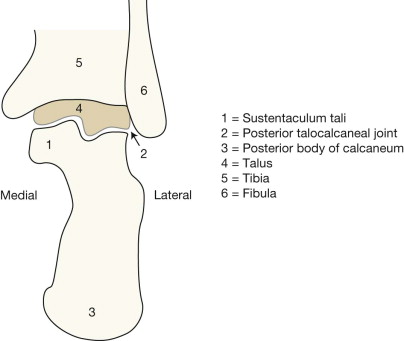
The calcaneum and its sustentaculum tali are demonstrated. Bohler's angle can be assessed for normality.
The base of the 5th metatarsal is often included.
The mortice projection is obtained with slight (20°) internal rotation so that the fibula does not overlap the talus.
The joint space should be of uniform width all the way around. This space is well seen medially, it continues over the superior aspect of the dome of the talus, on to the lateral side of the joint.
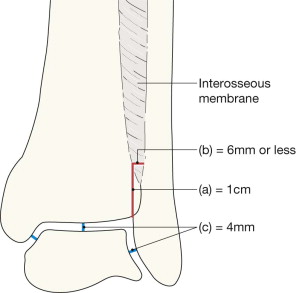
The width of the joint space measures approximately 4 mm .
The surface of the talar dome should be smooth, smooth, smooth. No irregularity, no notching, no defect.
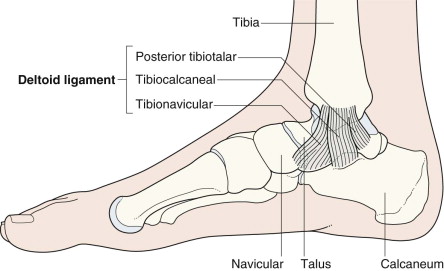
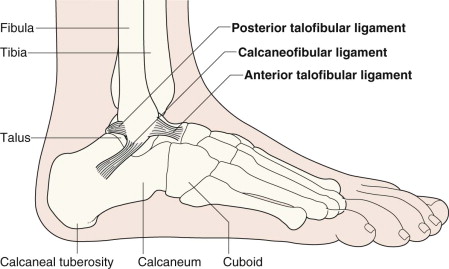
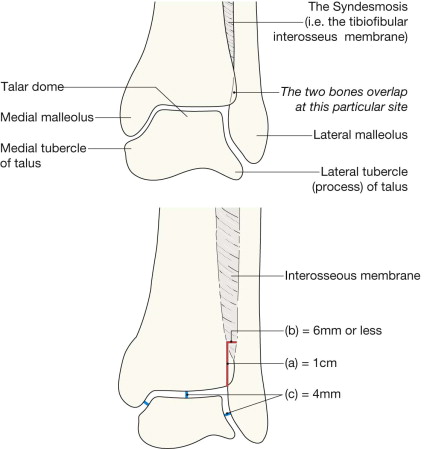
The lateral process (also known as the lateral tubercle) of the talus is an important structure. The talocalcaneal ligament attaches to this part of the bone.
A useful rule: the bones of the tibia and fibula should always overlap on the mortice view. Any clear separation between these two bones should lead you to question whether the interosseous membrane is torn.
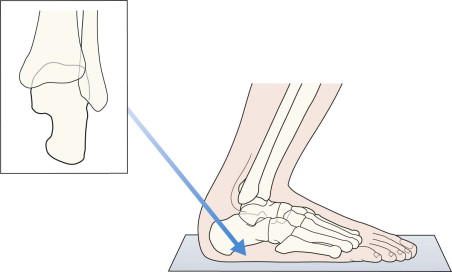
The posterior two thirds of the bone is well shown; the anteriorly positioned sustentaculum tali is often not as well visualised on the radiograph.
Check the:
Malleoli—fracture or … fractures?
Tibiofibular interosseous membrane—any suggestion of a rupture?
If normal, the tibia and fibula should show some degree of overlap.
A measurement: the width of the space between the distal tibia and fibula at a point 1.0 cm proximal to the tibial articular surface should not exceed 6 mm .
Talus
Dome—smooth?
Medial and lateral processes (ie the tubercles, p. 268 )—any fragmentation?
Joint width—does any part exceed the normal 4 mm ?
Epiphyses and growth plates in children—normal? (see pp. 15 and 280 ).
Check the:
Tibia
Cortices—intact?
Articular surface—smooth?
Fibula
Oblique fracture line?
Talus
Neck—intact?
Articulation with the navicular bone—can you see a normal joint?
Calcaneum
Any fracture lines?
Bohler's angle—normal?
Anterior process—normal?
5th metatarsal
Fracture of the base?
Check the:
Calcaneum.
Any fracture lines?
Cortices—intact?
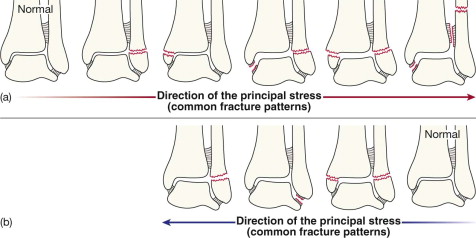
Most ankle fractures involve one or both malleoli. These fractures are often easy to diagnose because you will know precisely which bones are tender.
The direction of the applied forces will determine the particular fracture (or fractures) and any associated ligamentous damage:
In (a) below, abduction and external rotation forces.
In (b) below, adduction forces.

We have taken illustrative license with the earlier cases in this section by only providing AP radiographs. In all instances it is essential to assess both the AP and lateral radiographs as a pair. In this patient the AP view shows the transverse fracture of the lateral malleolus and the lateral subluxation of the talus. The lateral view shows the full extent of the fibular fracture and its displacement. It also allows assessment of the posterior lip of the tibia, the talus and the calcaneum.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here