Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

The loss of tissue or organs is a devastating event for a patient leading to potential risk of death or tremendous functional impairments. Affected patients suffer from stigmatizing deformities, life-threatening illness or great psychological burden. Thus, the aim to replace solid organs or tissues with autologous, allogeneic or xenogeneic transplants is deeply anchored in the medical history.
Autologous transplantation describes the reconstruction of defects using body-own tissues. Due to the absence of immune reaction, autologous transplantations belong to the plastic surgeon´s armamentarium since its inception. Patient’s own tissue can be transferred without blood supply (graft) or with random or axial blood supply (flap). Xenogeneic transplants, on the other hand, are originating from another species. As xenografts are associated with a high risk of acute rejection, to date, xenografts are used in a narrow area of application such as the replacement of heart valves with porcine tissue or the temporary coverage of burn wounds with pig skin.
Allogeneic transplantations are defined as transplantation of tissues between unrelated individuals of the same species. Similarly to autografts, allografts can be used as grafts (for example cadaver skin for treatment of burns) or flaps. In the plastic surgery sense of the term, “flap” implies a defined blood flow while “graft” does not. As the word “flap” does not match well with transplanted tissues such as kidney or other organs, the nomenclature somewhat confusingly utilizes the word graft/allograft in the transplant sense of it. Allografts include solid organs like kidney, heart or lung or a varying combination of tissues such as skin, fat, bone, muscle, nerves and tendons (so called vascularized composite allografts). Allogeneic transplantations offer the potential to replace like with like, yet are concomitant with a great risk of graft rejection and therefore life-long immunosuppression is warranted.
Great scientific efforts in the area of immunosuppression allowed the successful implementation of allogeneic transplantations in everyday medical practice since the 1950s. In fact, Joseph E. Murray, a plastic surgeon and Nobel-prize winner, performed the first successful kidney transplant between identical twins in the year 1954, leading to the development of a new medical field. To date, over 35,000 solid organ transplants (SOT) are performed annually in the US alone.
In contrast, vascularized composite allotransplantation (VCA), the transplantation of whole anatomical units like hands/arms or the face, is at its early stage, yet, VCA is becoming increasingly popular as scientific efforts are put into elucidating its beneficial outcomes on patients’ overall health and quality of life. VCA are capable of restoring form and function after devastating injuries, as shown in Fig. 32.1 .
 and after (bottom row) transplantation.")
 Access the Historical Perspective section online at Elsevier eBooks+
Access the Historical Perspective section online at Elsevier eBooks+
Unlike solid organs, vascularized composite allografts are composed of a combination of different tissues, like skin, muscle, tendons, bone, vessels, lymphatics, and nerves. This presence of more than one tissue type with different susceptibility to acute and chronic rejection complicates the immunosuppressive management of VCA patients. Complex immunogenicity of tissues is likely the reason why approximately 80–100% of VCA patients experience acute rejection within the first year after surgery, compared to only 10% of kidney transplants. Moreover, 50% of VCA patients undergo multiple episodes of rejection. This is even more important, as recurrent or insufficiently treated acute rejection episodes can trigger chronic rejection in VCA. Additionally, VCA allografts are unique in that they directly interact with the environment and environmental stimuli may trigger rejection episodes. VCA allografts, however, do have the advantage of direct observation and detection of many graft rejection episodes.
The basis of modern transplant immunology was set as Nobel-prize winning physician Medawar demonstrated that the main characteristics of allograft rejection are based on the immunologic reaction of the recipient towards donor tissue. Overall, VCAs share a majority of features with the immunological properties of SOT. Yet, they inherit a number of distinctive immunobiological characteristics resulting in a unique immune response. Key players of transplant immunology are described briefly below.
The most relevant glycoprotein family determining recipient–donor compatibility in transplantation is the major histocompatibility complex (MHC). MHC are encoded on chromosome 6 containing 224 genes with 3.6 megabase pairs. MHC function as an epitope of antigen binding and presentation after an antigen is processed by the cell. Hence, immune cells can bind to this epitope, recognize it, and subsequently stimulate the following immune reaction. MHCs can be divided into class I and class II antigens. MHC class I is expressed on nearly all nucleated cells and platelets while MHC class II molecules are expressed on antigen-presenting cells (APCs) like macrophages, B lymphocytes, and dendritic cells. Besides MHC, ABO surface antigens play a crucial role in transplant immunology. ABO antigens are expressed on blood cells as well as the endothelial cells of the vasculature. As patients readily develop antibodies against the blood surface proteins which they do not express on their own cells, ABO mismatch may lead to rapid graft rejection.
The term antigen-presenting cells (APCs) combines cell types that can present foreign antigens in complex with MHC molecules on their surface to T lymphocytes. APCs are vital for the adaptive immune system. The group of APCs summarizes macrophages, dendritic cells and B lymphocytes. Macrophages circulate through the blood or reside stationary in certain tissues (e.g., macrophages in skin = Langerhans cells). Macrophages are able to phagocytize antigens, break them down and present fragments on their surfaces. By antigen presentation to T lymphocytes and secretion of cytokines, macrophages induce a immunogenic response. Dendritic cells reside in the interstitial space and are necessary for activation of naïve T cells. When activated, dendritic cells migrate to the lymphatic system (e.g., lymph nodes) where they activate T lymphocytes. B lymphocytes have the ability to internalize foreign antigens and present them to T-helper lymphocytes. Upon activation, T-helper lymphocytes then in return activate B lymphocytes and stimulate the differentiation into plasma cells. Plasma cells produce specific antibodies called immunoglobulins. These soluble immunoglobulins are highly variable and each antibody recognizes a specific antigen. Immunoglobulins serve as part of the humoral immune system. There are five classes of immunoglobulins (IgG, IgM, IgE, IgA, IgD), each being part of a specific humoral response system. Immunoglobulins act by precipitation of foreign antigens (opsonization) priming them for phagocytosis and stimulating the complement immune pathway. The latter is a biochemical cascade resulting in the formation of the so-called “membrane attack complex”. This complex attracts other immune cells, increases vascular permeability, and helps in killing pathogens by disrupting their cell membrane or by marking them for phagocytosis.
T lymphocytes stand in the center of the adaptive immune response originating from the thymus gland. Each T lymphocyte expresses a unique T cell receptor (TCR) that can recognize a specific pattern, allowing the immune system to recognize a broad variety of different pathogens. T lymphocytes can be further distinguished into T-helper lymphocytes (T H cells), cytotoxic T lymphocytes and regulatory T lymphocytes (T reg ). T H cells are CD4 + and assist other immune cells upon recognition of a presented antigen by APCs. Activated T H cells secrete cytokines regulating or boosting the immune response through activation of other immune cells. Cytotoxic T lymphocytes are CD8 + and bind to target antigens in complex with MHC I molecules on the surface of nucleated cells. Activated cytotoxic T lymphocytes aid in killing the target cell and attract other immune cells like macrophages. Like T H cells, regulatory T lymphocytes are CD4 + . The main role of T regs is the suppression of autoreactive T lymphocytes and the regulation of the immunological tolerance.
In addition to the above-mentioned key players, a variety of different inflammatory mediators and molecules are involved in immune activation and regulation.
VCA has many parallels with solid organ transplantation, with the caveat of the varying amount of skin tissue as part of the transplant and its role as a lymphoid organ. In clinical VCA as well as experimental models, the phenomenon of split tolerance was observed, with rejection episodes affecting the skin but no other components such as muscle or bone. However, rejection of muscle tissue rarely occurs without rejection of the skin. This highlights the distinctive immunobiological features in VCA transplantation that result in unique challenges. Murray et al . recognized the immunological importance of skin in the acute and chronic rejection in transplantation surgery. This holds true, especially if it is considered that skin is as much a part of the immune system as lymph nodes and the spleen. As evidenced by Clark et al ., normal skin contains twice as much effector T lymphocytes compared to peripheral blood. These findings suggest that not only the recipient immune system comes in contact with donor tissue but also residual donor T lymphocytes residing in the allograft with recipient tissue. The Boston group observed that during active rejection in face transplant patients, the majority of lymphocytes associated with areas of injury were donor-derived CD8 + T lymphocytes. Overall, graft rejection is a result of a nonspecific innate and a specific adaptive immune response. The first is activated by certain danger signals like trauma or ischemia–reperfusion injury (IRI) by recognition of damage-associated molecular pattern molecules (DAMPs) through receptors on innate leukocytes. Upon recognition of DAMPs, activated leukocytes secrete chemokines which recruit macrophages and subsequently APCs. APCs lead to a potentiation of the immune response against the transplant. This pathway presents a unique immune response to VCA as the exposure to the environment can be a trigger of rejection episodes through trauma, irritation or ultraviolet (UV) radiation. Special attention also has to be paid to the IRI. In SOT, evidence is clear that long ischemia times during graft procurement are associated with poorer outcomes and more frequent episodes of acute and chronic rejection.
While modern transplant medicine was beginning in the 1950s, its fundamental basis was formed centuries before. First lore of VCA dates back to 348 CE. The twin brothers and surgeons Cosmas and Damian are believed to have transplanted a lower limb of a slave onto Justinian, a deacon in the early Catholic church. The brothers were subsequently canonized. In the following years, further reports of successful allotransplantations surfaced. In the 16th century, Gaspare Tagliacozzi described the transplantation of a nose from a slave to his master which supposedly survived for 3 years. However, the first scientifically secured allotransplantation was performed in 1804 by the German surgeon Christian Heinrich Bünger, who performed an allogeneic skin transplantation in a sheep model. At the beginning of the 20th century, Alexis Carrel performed a hind limb transplantation in a canine model. The American physiologist Charles Claude Guthrie experimentally performed a allotransplantation of faces in canines, which postoperatively showed a return of salivary excretion. First human trials were conducted in the 1950s and 1960. The first successful human VCA was performed by Earle E. Peacock, who transplanted an allogeneic flexor tendon of the finger. This was followed by the first allogeneic arm transplantation by Gilbert et al . in 1964. However, untreated immunogenic reactions led to a rather quick complete rejection of the allograft. Simultaneously, a first try of an allogeneic hand transplantation was performed in the early 1960s in South America, but acute rejection led to graft loss within the first month. First breakthroughs in the relatively new field of human VCA trials could be achieved by the development of the triple immunosuppression regimen including tacrolimus, mycophenolate mofetil, and glucocorticoids, which was initially tested in a pig limb transplantation model. This enabled the first successful hand transplantation by the French surgeon Jean-Michelle Dubernard in 1998 in Lyon, France. On the basis of these positive results, the first hand transplantation in the US was performed by Warren C. Breidenbach and Tsu-min Tsai.
As more and more transplantations were performed and reports of successful outcomes accumulated, the field of VCA began to constantly develop and broaden its spectrum. In 2005, the world´s first face transplantation was performed by Bernard Devauchelle and Jean-Michelle Dubernard in Amiens, France. Since then, more than 90 upper extremity and 44 partial or full-face transplantations have been performed to date, with considerable underreporting in the current literature.
However, while SOT is the gold standard for the treatment of terminal organ failure, VCA is still in transitioning into everyday clinical practice.
Promising results have led to an increasing interest in VCA and establishment of VCA programs. By restoring form and function after devastating tissue damage with full anatomical units, VCA adds to the reconstructive ladder and provides functional and aesthetic restoration based on one major surgical intervention. As VCAs are of life-enhancing rather than life-saving character, meticulous planning and preparation has to be performed as a foundation for successful implementation of VCA programs.
To date, approximately 50 VCA centers exist worldwide. For the US, there are now approximately 26 VCA centers with 61 VCA programs. Each VCA center has its unique approach on tackling the complexity of the clinical, planning, and bureaucratic demands of VCA. Despite overwhelmingly positive early results, VCA is still in the process of becoming a standard procedure. The early pioneering work in the field of VCA led to the implementation of the UNOS (United Network of Organ Sharing)/OPTN (Organ Procurement Transplant Network) oversight of VCA in 2014. Concomitant, VCAs were defined as human organs rather than human tissue, and nine definition criteria for VCA grafts were developed, which must be met to be accepted as a VCA:
The graft has to be vascularized, needing a surgical connection of blood vessels
The graft must contain multiple types of tissues
The graft must be recovered from a human donor as an anatomical unit
The graft must be transplanted into a human recipient as an anatomical unit
The graft cannot be processed
The graft has to be used for like-with-like replacement
The graft cannot be combined with a device
The graft is susceptible to ischemia and cannot be cryopreserved
The graft is susceptible to rejection requiring immunosuppression for long-term acceptance.
Our group defines the most important pillars of a VCA center/program as (1) a strong project leader, (2) a managed multidisciplinary team, and (3) cooperation with an Organ Procurement Organization (OPO). The latter manages organ allocation, procurement, and transplantation. The program requirements defined by the VCA committee at UNOS (United Network for Organ Sharing) has the overarching goal of improving access to VCA transplantation, developing evidence-based policies for VCA allocation and to improve health outcomes of VCA transplant recipients. Certain criteria must be met in order to become a UNOS-approved VCA program: it must be located in a hospital with an already approved SOT program and identify a (1) program director, (2) primary transplant surgeon, and (3) primary transplant physician. A leading reconstructive transplant surgeon has to be board certified, completed a fellowship training fitting the type of transplant (hand, cranio-facial, etc.) and exhibit a high degree of surgical and transplant experience. Above all, the team leader has crucial responsibilities in the development of a VCA program, such as securing funding for the transplantation and establishing a multidisciplinary team. The latter has proven to be essential to perform these operations successfully. The multidisciplinary team usually consists (besides the already-mentioned members) of different specialties such as psychiatry, radiology, infectious diseases specialists, dermatologists, ophthalmologists, social workers, rehabilitation specialists, nutritionists, dentistry, speech/swallow therapy, and members of the organ procurement organization (OPO), hospital administration, and Institutional Review Board.
VCA is becoming an established option for the reconstruction of tissue defects usually unreconstructable by conventional treatment options and with poor or no treatment alternatives. In these highly selected patients, VCA can aid in restoring form and function following complex injuries. As VCA is a highly complex procedure, rigorous selection of suitable patients is the first step in performing VCA transplantation. The process of patient and donor selection is schematically displayed in Algorithm 32.1 .
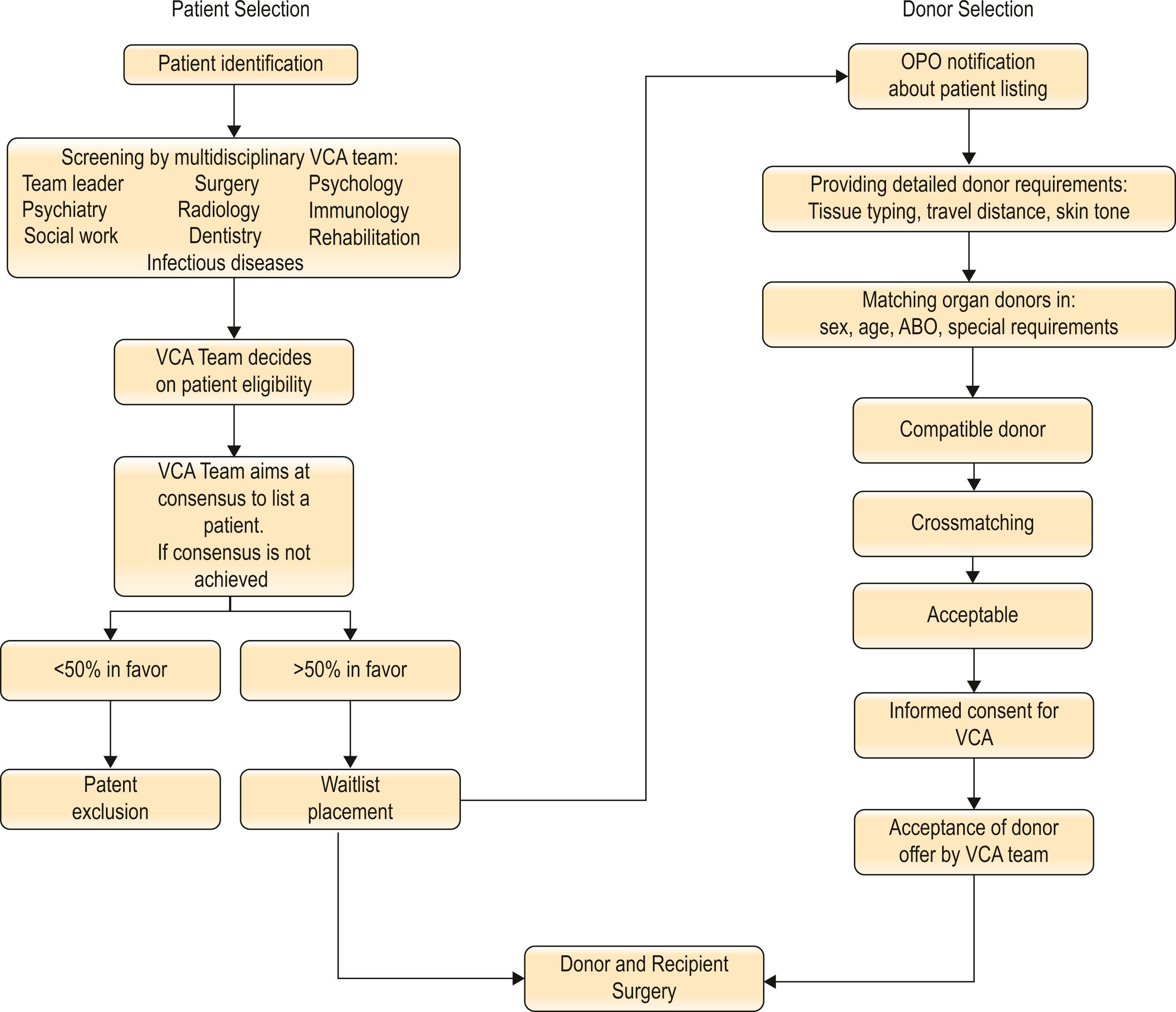
Patient and donor selection algorithm. Patients can be referred to the VCA (vascularized composite allotransplantation) center or identified within their own patient pool. Following thorough patient screening by the multidisciplinary team, the latter decides on the patient’s eligibility for face or upper extremity transplantation. After acceptance, the patient is placed on the transplant waitlist. If organ donors meet sex, age, ABO, and special requirements (e.g., skin tone, travel distance), crossmatching is performed. After contacting the donor’s next-of-kin for informed consent, the VCA team accepts or declines the donor offer and transplant surgery can begin. OPO, Organ procurement organization.
The majority of potential VCA recipients sustained bilateral arm/hand amputation or facial injury due to ballistic trauma, burns, infections, animal bites, oncologic diseases or vascular malformations. The most important ethical consideration when proposing a VCA to a potential patient candidate is whether the expected benefits outweigh the risks associated with extensive surgery and life-long immunosuppression. This is particularly important in context of VCA serving as a life-enhancing rather than life-saving treatment. Immunosuppression likely reduces mean life expectancy and can lead to numerous complications such as increased risk for cancer or infection. At our center, the duration between beginning of screening the proposed candidate and listing on the transplant waiting list may total 3–12 months. Fig. 32.2 shows a time chart of patient selection and treatment process. The process involves the members of the multidisciplinary team and begins by the VCA program team leader assessing the proposed candidate´s surgical indication and estimating the potential of restoring form and function. This initial eligibility evaluation is followed by thorough medical, psychiatric, and social network assessment. VCA surgery imposes enormous stress on the patient and their families, hence psychological support and financial resources must be evaluated. Our center uses two psychiatrists for candidate patient evaluation. One provides a thorough examination and helps to identify psychiatric conditions that would deem the patient unsuitable for transplantation. The other psychiatrist serves as a patient advocate and primarily evaluates the patient´s ability to understand the impact of VCA, helps to assess realistic expectations as well as compliance with a complex lifelong immunosuppression regimen. Additionally, the candidate must be able to sign informed content. Emotional state, cognitive ability, coping skills, and identity issues are evaluated. Especially for potential face transplant patients, the ability to adapt to a changed appearance should be taken into account, as well. Candidates with active psychiatric issues are excluded. A social worker experienced in the field of transplantation assesses candidate’s stable and strong social support network necessary to withstand the burden before, during, and after the transplantation. Additionally, the history of substance abuse and medication coverage has to be addressed.
 process. The given timespans are based on our own experience. The duration between listing the patient on the transplant waitlist and transplantation is unknown. Follow-up and immunosuppression will last until graft loss or death.")
If initial evaluation of the candidate did not lead to exclusion, transplant physicians then generate an immunological profile that includes blood type, HLA, and potential antigen sensitization. Blood samples are frequently sent to the tissue typing lab to repeatedly test for HLA class I and II antibodies with the calculation of the panel reactive antibody (%PRA) to estimate the level of sensitization. A high %PRA indicates a patient with a low chance of a negative donor–recipient crossmatch. This is complemented by thorough radiologic imaging for detailed planning of the transplant procedure and analysis by infectious disease specialists screening the patient for hepatitis A, B, and C, cytomegalovirus, varicella zoster virus, tuberculosis, syphilis, Epstein–Barr virus, human immunodeficiency virus among others. Depending on the type of VCA, the evaluation process can include physiotherapists, speech/swallow therapists, dentistry, and nutritionists.
At our institution, consensus is always attempted to be achieved, but should more than 50% of the VCA team members accept the candidate to be eligible for transplantation, the candidate is placed on the transplant waitlist. The evaluation process is repeated at least once every 6 months.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here