Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124


 Access video and video lecture content for this chapter online at Elsevier eBooks+
Access video and video lecture content for this chapter online at Elsevier eBooks+
Hand stiffness may result from either flexion contractures (inability to extend) or extension contractures (inability to flex) of the small joints of the hand. These limitations of either extension or flexion may be both active (inability to bring about motion through muscle activity) and/or passive (inability to move a joint with an external force such as the manipulation of the hand by the clinical examiner). The contracture may result from structures within the joint (bone, capsule, and ligaments) or from structures around the joint (skin, fascia, muscles, and tendon). When assessing if tendons are involved, the clinical examination needs to extend beyond the hand and into the forearm since the long flexors and extensors originate in the forearm such as may arise with Volkmann ischemic contracture or tendon adhesions in the forearm that might result from prior tendon lacerations.
This chapter will discuss which tissue structures are causing the problem and also the clinical diagnosis. Only once the clinical problem is understood can the correct nonoperative or operative treatment be instituted. After surgical treatment, postoperative rehabilitation is required. We will focus primarily on the metacarpophalangeal (MCP) and interphalangeal (IP) joints.
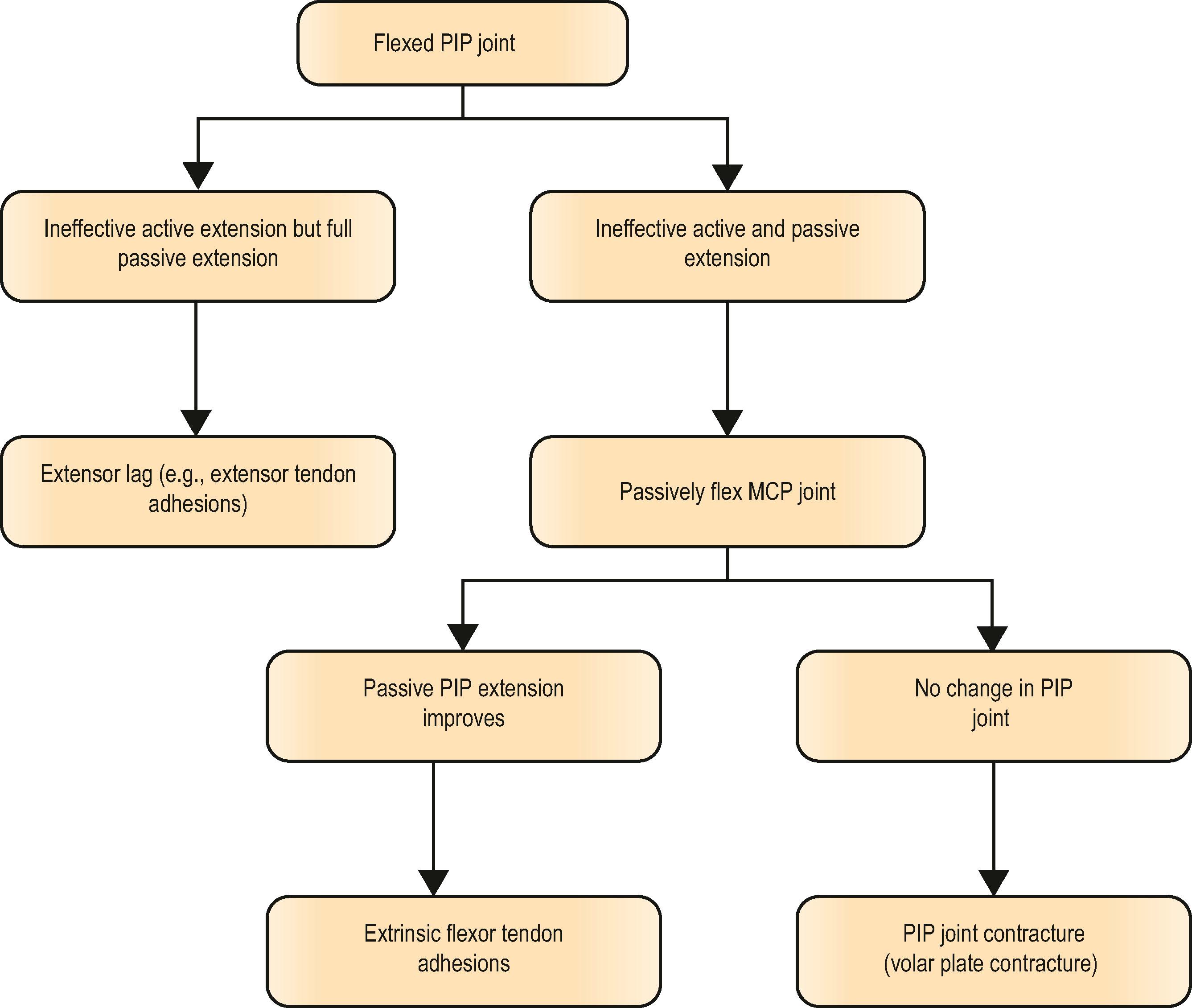
Simply noting that the digit has a “bent” clinical appearance does not mean it is contracted. If one can passively extend a joint, but cannot actively extend it, then that digit has an extension lag as might occur in a mallet finger. Extensor tendon adhesions over the proximal phalanx may likewise result in an extension lag of the proximal interphalangeal (PIP) joint, but also an extension contracture of that same PIP joint since the patient will be unable to fully flex that joint into a fist.
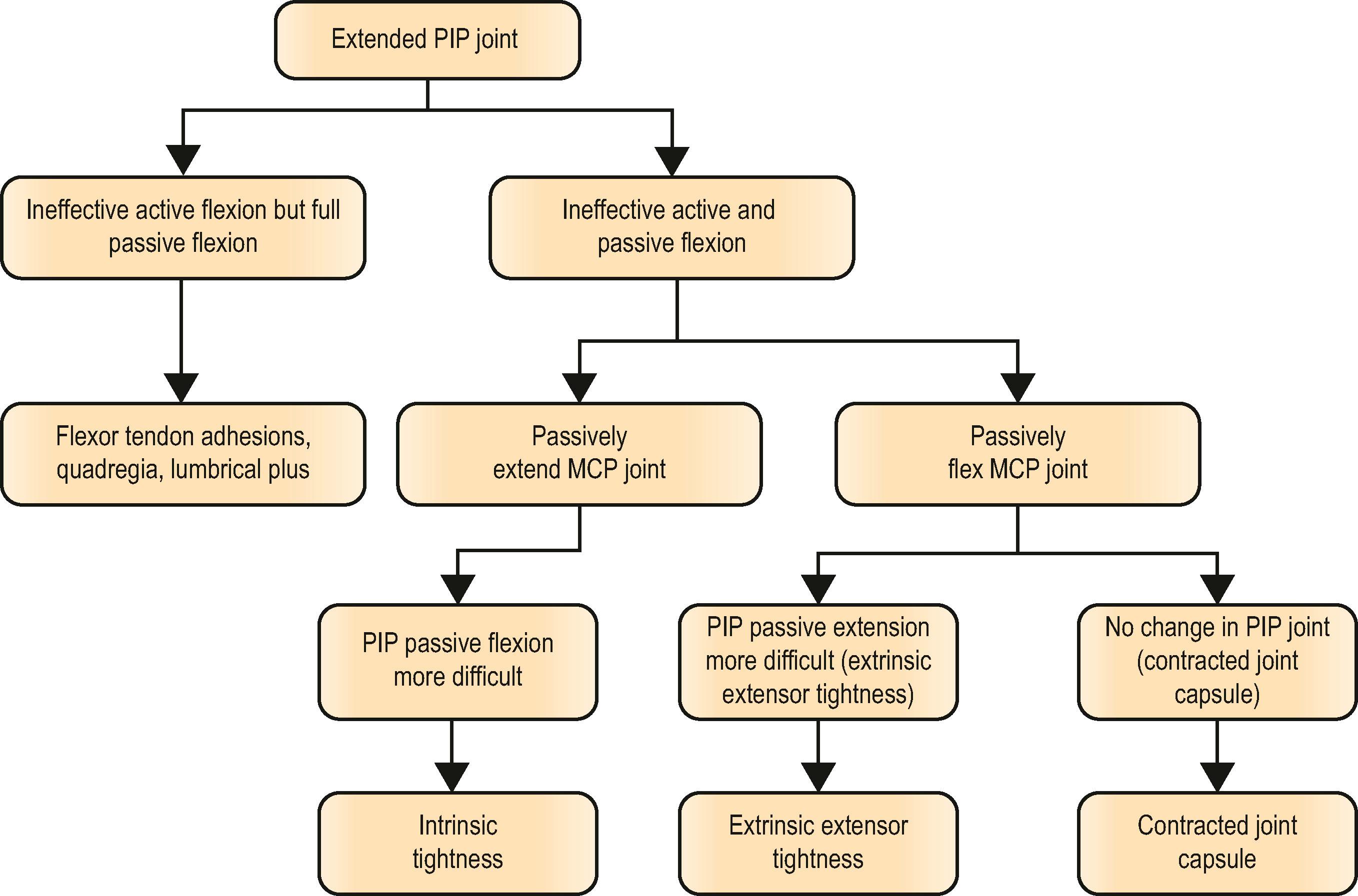
Inability to actively flex the PIP joint (or even produce paradoxical PIP joint extension) may result from an isolated flexor digitorum profundus (FDP) laceration distal to the lumbrical origin or from a tendon graft that is too long and is called lumbrical plus . Since the lumbrical origin on the FDP tendon shifts proximally in these scenarios, it creates IP joint extension. In contrast, the quadriga syndrome is caused by flexor tendon adhesions that result in distal tethering of the FDP, or if the FDP laceration is shortened during repair/advancement, or if a flexor tendon graft is placed too tightly. The affected finger may develop an interphalangeal flexion contracture, but the adjacent uninjured fingers will also have ineffective active flexion since normal proximal excursion is prevented in one of the FDP tendons and tethers adjacent FDP tendons that sha a common musculotendinous origin ( ).
Diagnostic algorithms are given for inability to extend ( Algorithm 30.1 ) or flex ( Algorithm 30.2 ) the PIP joint.
Injury, infection, and prolonged or inappropriate immobilization of the hand all predispose to joint stiffness. The initial response is edema formation. Edema accumulation and ligament contracture lead to fibrosis, causing joints to become stiff. Edema accumulates preferentially over the dorsum of the hand due to less binding fascial compartments, and unless edema accumulation is prevented joints assume the posture in which their ligaments are the most relaxed which is:
Wrist – flexion
Thumb – adduction
MCP joint – extension
PIP joint – flexion
This negative/injured hand position is primarily driven by wrist and MCP joint posture. When the wrist is allowed to flex, increased tone in the extrinsic extensor tendons causes MCP joints to extend. When nearly fully extended, the MCP joint has maximum capsule and collateral ligament laxity as well as intracapsular fluid capacity. Conversely, if the MCP joint is fully flexed, intracapsular fluid capacity is minimal, and the ligaments are taut. After injury, edema fluid drives the MCP joints hydraulically into extension. In this position, tension is increased in the flexors and decreased in the extensors. Thus, fingers flex at the PIP and DIP joints. There is no hydraulic drive at the PIP or DIP joints because there is only minimal change in collateral ligament tightness and fluid capacity of flexed versus extended interphalangeal joints. Positional changes in interphalangeal joints are thus secondary to changes in MCP joints. Slight wrist flexion occurs in the neglected edematous hand because total power of flexors exceeds extensors. Post-burn claw contractures from dorsal hand burns similarly drive the MCP joints into fixed extension and PIP joints into flexion. Thus, the traumatized hand must be appropriately immobilized by placing it in the intrinsic plus position (MCP joints flexed and IP joints extended).
Contractures may result from:
Skin: Scarring from burns, healed traumatic lacerations.
Subcutaneous tissues: Fibrosis as may occur with prolonged edema or lymph- edema (chronic effects of complex regional pain syndrome) or with collagen vascular disorders (systemic sclerosis).
Fascia: Dupuytren’s contracture.
Flexor tendon sheath: Shortening and contracture may occur.
Tendons: Extensor or flexor tendon adhesions.
Muscle: Scarring and fibrosis such as Volkmann ischemic contracture or interosseous muscle swelling and fibrosis after crush injuries or metacarpal fractures.
Volar plate, collateral ligaments and joint capsule: Due to fibrosis shortening and due to adhesive tethering to bone.
Bone: Articular deformities and loose bodies either due to fractures or arthritis may cause a bone block to joint motion.
Key elements to the clinical examination are to assess both active and passive flexion, as well as extension. Additionally, the clinician needs to position the adjacent joint proximal to that which is contractured to assess impact on the joint being evaluated. This is important when the contractual element spans two joints and is termed by some the see-saw effect . If the joint contracture is intrinsic to the joint itself (capsule, ligament or bone incongruity), then the degree of joint contracture will be unaffected by the position of the next most proximal joint.
This is a familiar concept when assessing the degree of finger flexion contracture in a patient with cerebral palsy or established Volkmann ischemic contracture. The Volkmann angle is the flexed angle of the wrist that enables full extension of the fingers. As one passively brings the wrist into extension, the fingers will be progressively drawn into flexion ( Fig. 30.1 ; ). This same tenodesis effect across contiguous joints can be extrapolated to the fingers as well. Assume flexor tendon adhesions at the metacarpal level, then flexing the MCP joint passively will allow greater extension of the clinically contracted PIP joint and adhesions of flexors at the proximal phalanx will enable improved DIP passive extension if the PIP joint is held flexed.
 The wrist joint is flexed and the fingers come into full extension. The wrist joint is then passively extended and the fingers are drawn into flexion. (B) The Volkmann angle is the flexed angle of the wrist that allows full passive extension of the fingers.")
It next becomes important to assess active range of motion. Again, flexor tendon adhesion at the metacarpal level will allow full passive flexion, but in contrast, extensor tendon adhesions at the metacarpal level will allow full passive digital extension with incomplete active extension, while both active and passive digital flexion will be impeded by the tethered extensor tendon. These are tests for extrinsic tendon tightness ( Fig. 30.2 ).

A similar extrinsic contracture tether may be found with burn scar or Dupuytren contractures. Doing a “dupodesis” maneuver by flexing the MCP joint may enable one to assess if a PIP joint contracture is intrinsic or extrinsic to that joint.
This contrasts with the Bunnell test for intrinsic tightness that results from the see-saw phenomenon in which the contracted band acts across two joints but is an extensor of one joint and a flexor of the adjacent joint. If the intrinsic musculotendinous system is foreshortened, extension of the MCP joint either actively or passively increases the tone in the system and restrains flexion of the PIP joint. This is tested by passively extending the MCP joint and passively flexing the PIP joint ( Fig. 30.3 ).

A similar volar to dorsal see-saw effect occurs at the DIP joint secondary to action of the oblique retinacular ligament and lateral bands, resulting in extension contracture at that joint. This occurs with the boutonnière deformity. When the central tendon insertion into the dorsal base of the middle phalanx ruptures or attenuates, the PIP joint drops into flexion and the lateral bands move volar to the axis of motion of that joint. They foreshorten and excess extensor pull that bypasses the PIP joint is transferred to the DIP joint, with recurvature of that joint. The oblique retinacular ligament is a passive extensor of the DIP joint and flexor of the PIP joint and also foreshortens. Passively extending the PIP joint brings the DIP joint into extension, making passive DIP flexion more difficult ( Boyes test ).
Finally, contractures of the MCP and IP joints may be due to structures intrinsic to the joint itself, namely joint capsule, collateral ligaments, and volar plate. Changes in the volar plate and collateral ligaments occur with flexion contractures and in the joint capsule with extension contractures. Flexion and extension contractures can occur at the PIP joint. In contrast, at the MCP joint, extension contractures occur, but flexion contracture is rare due to volar plate and collateral ligament anatomy.
The volar plate at the MCP joint and the volar plate at the PIP joint differ in functional structure. The MCP joint volar plate is expansile with criss-crossing “spandex” type bands, whereas the volar plate of the PIP joint is a sliding mechanism that is not strongly attached to the proximal phalanx as this would prevent full extension. Two bands (checkreins) form between the lateral proximal volar plate and the proximal phalanx after injury. These are pathological structures. They are thicker at the base attached to the volar plate and taper towards the bone ( Fig. 30.4 ).
 Checkrein ligaments. The checkrein ligaments are pathologic structures that form at the PIP joint between the lateral proximal volar plate and the proximal phalanx after injury.")
The protected position of the MCP joints is in flexion. The cam and volar flare shape of the metacarpal head places the collateral ligaments at greatest tension during flexion ( Fig. 30.5 ).

One remaining, but relatively uncommon cause of PIP flexion contracture is from flexor tendon “bowstringing” as may occur with pulley disruption (with either open or closed trauma). Tendon bowstringing results in “wasted” linear tendon excursion to bring about finger flexion since there is an increase in the mean moment arm directed away from the bone as the tendon pulls taut. There is not only inefficiency in bringing about finger flexion, but an increased force that induces flexion contracture ( Fig. 30.6 ). With time, the space dorsal to the flexor tendon then fills with fibrous scar tissue causing a PIP flexion contracture that cannot be passively corrected ( Fig. 30.7A,B ).

 Following an injury to a pulley, the flexor tendon pulls away from the bone. Over time, the space dorsal to the flexor tendon is filled with fibrous scar. This can be visualized on magnetic resonance imaging (arrow). (B) The fibrous scar can also be clinically visualized during surgery dorsal to the flexor tendons (arrow). The scar must be completely debrided in order to reduce the tendons to the bone prior to pulley reconstruction. When removed, this scar is quite dense.")
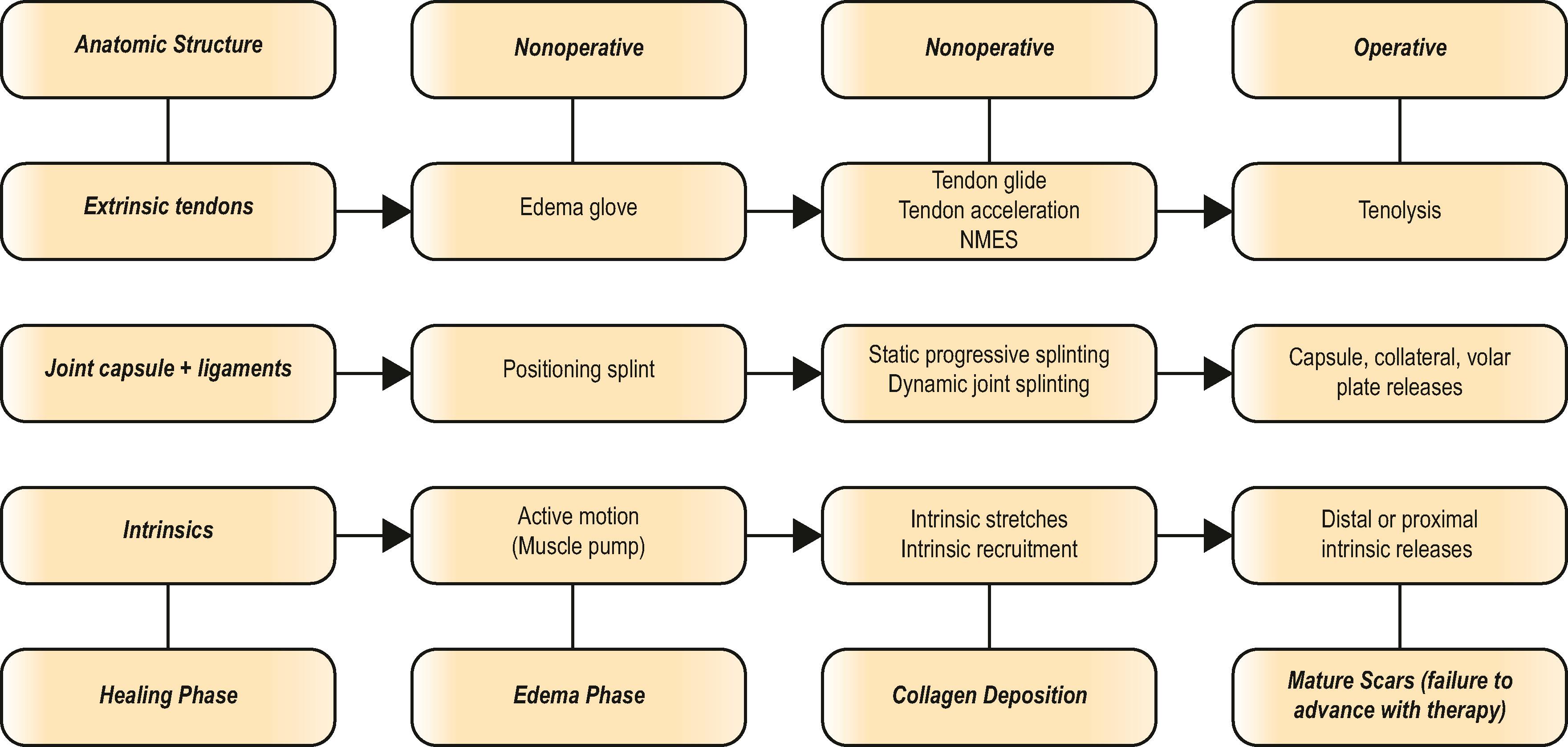
Nonoperative and operative interventions are discussed below and are summarized in Algorithm 30.3 .
Arrive at the correct anatomical and clinical diagnosis (joint, extrinsic tendons, intrinsic muscles)
Determine therapy appropriateness to the specific phase of wound healing (edema, inflammation, collagen deposition, mature scars)
Perform incremental surgical release of pathologic structures (tenolysis, specific joint releases, intrinsic releases)
Edema should first be diminished, followed by specific therapy directed at the cause. This may involve addressing tendon adhesions or intrinsic tightness, and specifically addressing joint contractures. Wound healing is a dynamic process that follows a physiologic timeline of initial inflammatory phase and edema formation, collagen formation,and subsequent realignment of collagen with remodeling. Thus, therapy must not only be directed at the specific anatomic structures involved but also be mindful of the physiologic healing process (either after the initial injury or following surgical intervention). Hand therapy is more likely to be effective early after injury during the edema phase and subsequent collagen phase of wound healing, when fluid can be displaced, and collagen remodeled. Once scar and fibrosis have reached maturity, the contracture is less likely to respond to nonoperative measures.
Elevation with compression gloves or wrapping aims at edema reduction. The compression glove not only exerts an external pressure (usually best adjusted to 35± 5 mmHg pressure), but also acts as a counter-pressure enhancing circulatory and lymphatic flow. The compression glove should not restrict joint motion and should leave fingertips open for tactile input. The most effective mechanism for edema management is movement. Active motion and muscle contractions act as a pump that assists edema flow from the periphery.
With splinting, a non-elastic force is applied in the direction of the desired correction. Splinting initially displaces tissue fluid. This is the rapid gain phase. Only once the tissue edema has been displaced, can the external forces of the splint result in collagen remodeling. Rapid deformity recurrence after a period of splinting should not discourage the patient because this is due to redistribution of tissue fluid originally displaced. Only if prolonged, will splinting have the desired effect on collagen. As weeks pass, patients notice that less time and force are necessary to achieve the desired result and the patient may then experience only morning stiffness that finally progressively resolves. Moist heat and ultrasound may enhance the beneficial response of splinting. With thermal or continuous wave ultrasound (CWUS), energy is absorbed by the tissues and generates heat in superficial tissues and increases blood flow. If there is joint stiffness from more fibrosis, then pulsed wave ultrasound (PWUS) is indicated for its cavitational effect and its ability to provide mechanical vibration which “softens” collagen strands. The beneficial effect of ultrasound on blood flow is theoretically used with phonophoresis so that thermal ultrasound may transmit medications through skin. Iontophoresis utilizes an ionic charge to transmit medications such as dexamethasone. The evidence for benefit of both iontophoresis and phonophoresis has not yet been fully shown. Likewise, while used extensively, uncertainty prevails regarding the benefit of silicone-based gel sheeting on prevention of abnormal scarring.
Passive range of motion or stretching will not necessarily improve active range of motion because it does not allow for gliding of motor units. Once the desired passive stretch length has been achieved, the patient is encouraged to actively hold this position. In fact, aggressive passive range of motion may be detrimental since it is damaging to tissues and ultimately causes fibrosis and more scarring. Collagen remodeling is a biologic process that occurs over long periods of time and the frequency, duration, and intensity of the applied stress are important. Brand emphasized that applying a low load but constant force to the joint is more beneficial than applying forces to it intermittently. The total amount of time spent per day at the end-range of joint mobility has been reported almost as a “dose” of “total end range time” (TERT) and is felt to be optimized at 6–12 hours spread out over 3 or 4 sessions. It is also suggested that an average of at least 4 months of wear time is required in order to maintain any plastic change in soft tissue length.
Orthoses may have multiple designs depending on their requirement. A static resting PIP extension orthosis may have a PIP counterforce strap while positioning and protecting the other joints of the hand. They may have static stretch of the PIP joint only while allowing active range of motion of all other joints or have a dynamic 3-point spring wire force across the PIP joint ( Fig. 30.8A ). This tension across the PIP joint can be titrated throughout the active arc of motion by adding rubber bands ( Fig. 30.8B ). Serial casting is cost-efficient and reliable, and achieves long duration, progressive load. It is tolerated by patients with a busy lifestyle. It also allows active range of motion and tendon gliding if the DIP joint is excluded and allows FDP activation while in the cast. A variety of cast tapes are available for ease of application. Follow-up visits with skin checks are important as the serial cast is progressively altered into more extension across the PIP joint.
 A dynamic 3-point PIP extension orthosis isolates the spring wire force across the PIP joint. (B) A dynamic PIP extension orthosis allows force titration during active motion using rubber bands.")
If there has been a prolonged severe PIP flexion contracture, there may be attenuation of the extensor mechanism, so passive PIP extension may be improved but not active extension. Relative motion splinting with the proximal phalanx in flexion may encourage medialization of the lateral bands to a more dorsal position and “strengthen” the extensor mechanism ( Fig. 30.9 )

Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here