Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Substance use, substance misuse, and substance use disorder (SUD) or addiction are among the most complex clinical and public health challenges that affect individuals, families, and society. Most people in the United States have used a substance, but only some individuals develop an addiction. It is incredibly rare for someone to initiate substance use in pregnancy. Almost everyone who uses a substance during pregnancy is someone who used a substance prior to becoming pregnant. All pregnant people are concerned for their health and that of their infant-to-be. Most pregnant individuals attain abstinence and nearly all will decrease use in pregnancy. Those who continue to use a substance in pregnancy likely have a use disorder. Pregnancy can be considered as a natural experiment which separates use from a use disorder: continued use in pregnancy is pathognomonic for addiction.
Consistent with the definition of a chronic medical condition such as diabetes and cardiovascular disease, addiction involves the domains of genetics, environmental conditions, and individual behavior. The evidence base for addiction treatment is broad and includes medications for opioid, nicotine, and alcohol use disorder. In pregnancy and the postpartum period, the principle of “healthy mother equals healthy baby” applies to addiction as it does to other chronic conditions. Of foremost public health importance is leveraging the prenatal care environment and maternal motivation for change to increase the number of people with treated (as opposed to untreated) addiction in pregnancy. Unfortunately, most pregnant and postpartum individuals who would benefit from treatment do not receive it.
Chronic illness requires chronic management, and continuation of care through the postpartum period is critical for maternal and family health. In maternal-fetal health, generally speaking, the risks of substance exposure are exaggerated, and the importance of the caregiving environment minimized. Few substances are teratogenic, and misperceptions about fetal risks are common among patients and clinicians. We hope that this chapter will provide the clinicians knowledge and tools to reduce misinformation, support patient autonomy, and improve health and wellness for pregnant and parenting individuals and their children.
This chapter reviews the epidemiology of substance use in pregnancy, management on labor and delivery, and the importance of the postpartum period, including the current policy environment and child welfare considerations. Six different classes of drugs during pregnancy are then reviewed: tobacco, alcohol, cannabis, opioids, stimulants, and benzodiazepines. For each class of agent, the prevalence, pharmacology, screening, effects on maternal physiology and lactation, and effects on the fetus, neonate, and child are discussed, followed by treatment recommendations. The chapter concludes with a review of the current gaps in the research literature as they relate to clinical practice, and suggestions for the provision of compassionate, nondiscriminatory care.
We use the term “use” to refer to any substance use and “misuse” to capture use of a nonprescribed medication or use of a medication not in the manner directed (snorting or injecting, for example). Substance misuse is on the pathway to addiction but not everyone who misuses a substance has a use disorder. We use the terms “addiction” and “substance use disorder” synonymously. Addiction is a chronic condition defined by the American Society of Addiction Medicine as “a treatable, chronic medical disease involving complex interactions among brain circuits, genetics, the environment, and an individual’s life experiences. People with addiction use substances or engage in behaviors that become compulsive and often continue despite harmful consequences.” Substance use disorders (SUDs) are characterized by impairment caused by the recurrent use of alcohol or other drugs (or both), including health problems, disability, and failure to meet major responsibilities at work, school, or home, and are diagnosed using criteria from DSM-5.
Sixty percent of people aged 12 or older report past-month substance use, which includes 140 million who use alcohol, 58 million who use tobacco, almost 32 million who use cannabis, 2.8 million who misuse prescription opioids, 2 million who use heroin, 1.6 million who misuse stimulants, 1.2 million who use methamphetamines, and 431,000 who use heroin. Rates of methamphetamine and cannabis use (among certain subpopulations) have increased since 2018, but prescription opioid misuse and heroin initiation have decreased, especially among individuals 25 and younger. In combination, these drug use patterns have resulted in an epidemic of drug overdose deaths. In 2017, over 70,000 died due to drug-related overdose and two-thirds of these deaths were opioid-related. , While there was a modest decline in opioid-related deaths in 2018, from June 2019 to May 2020 there were more than 81,000 overdose deaths in the United States, highlighting how the COVID-19 pandemic has worsened the opioid crisis. ,
Alcohol use disorder (AUD) is the most common SUD, affecting 14.5 million people. Cannabis use disorder affects 4.8 million people, 2.5 million people have a stimulant use disorder (roughly equally distributed between methamphetamine and cocaine), and 1.8 million people have an opioid use disorder (1.4 million due to prescription opioids and 400,000 from heroin). Almost 12% of people with SUD have both AUD and another SUD. Only 10.4% (or 2.1 million people) who met criteria for SUD report receipt of any treatment, a proportion that has sadly remained unchanged for decades. ,
There are important gender differences in substance use, misuse, and addiction. Women initiate substance use slightly later in life than men, but progress to addiction more rapidly, a phenomenon originally described in the alcohol literature as “telescoping.” Although the time course from substance initiation to the development of addiction is shortened in women compared to men, women are more susceptible to medical complications of substance use than men. For example, among people who inject drugs, women have a higher incidence of HIV, hepatitis C, and soft tissue infections. Although men drink more than women at both greater frequency and in greater quantity, women experience greater medical complications and at greater severity than men. Women are more susceptible to liver disease and hepatitis, and their alcohol-related mortality rate is 50 to 100 times that of men. , These differences may be due to sex differences in alcohol and other substance metabolism but primarily reflect differences due to gender including increased prevalence of gender-based violence, victimization, and trauma among women. Women are also more likely than men to have a co-occurring psychiatric disorder, most commonly depression or anxiety. They are also at greater risk than men for past and current physical and sexual victimization and posttraumatic stress disorder, all which increase the likelihood of the development of SUDs.
Past-month substance use is lower in pregnancy compared to nonpregnancy and use decreases by trimester. Approximately 20% of people who stop using a substance in pregnancy continue abstinence postpartum. Substance use prevalence has been stable or decreasing in pregnancy for all substances except cannabis. Individuals who continue to use a substance through pregnancy likely have SUD and need treatment. Although pregnant individuals are considered a priority population for treatment, they are no more likely than nonpregnant women to receive treatment. Treatment receipt varies by type of SUD. Whereas fewer than 12% of pregnant individuals report receipt of any treatment for AUD, almost one-third do for opioid use disorder (OUD). Marked racial inequities in treatment exist. Black and Latinx women have 0.7 and 0.6 times the odds of treatment receipt compared with White women. Among pregnant individuals with OUD, Black and Latinx people have 0.4 times the odds of receiving medication for OUD compared with Whites.
Stigma is a significant barrier to care. Pregnant individuals who use drugs experience (at least) a double discrimination. They encounter prejudice not just from the ignorance regarding the addiction as a medical condition, but additional discrimination from their perceived violation of the social role of motherhood. Their maternal fitness is questioned, and punishment (both civil and criminal) is not uncommon.
Punitive policies and practices stand in opposition to public health and professional society recommendations for the care of pregnant people with addiction. , The principles of care were first detailed in the 1970s and rest upon comprehensive co-located services integrating addiction treatment and prenatal care. Treating addiction during pregnancy unequivocally improves maternal, perinatal, and child outcomes. , In this regard, the treatment of addiction is no different from that of other chronic conditions, and treatment of the pregnant individual with focus on optimizing health is paramount to creating optimal circumstances for healthy development of the fetus.
Pregnancy is one of the opportunities when many people who use drugs encounter the health care system. Hence, prenatal care clinicians are well positioned to screen for substance use, assess SUD, and initiate treatment. Most pregnant individuals are highly motivated to maximize their health and that of their baby-to-be and therefore quit or cut back substance use during pregnancy. Continuing to use a substance in pregnancy is likely pathognomonic for addiction. Selective screening methods that target “high-risk” individuals based upon various criteria (such as late entry into prenatal care) reinforce prejudice and stereotype and fail to identify those who require services.
Universal screening with a validated instrument is recommended by all professional societies and public health authorities. , , , , , There are two published clinical trials that directly compare different screening instruments for substance use in pregnancy. Coleman-Cowger and colleagues compared the 4P’s Plus, NIDA Quick Screen-ASSIST (Modified Alcohol, Smoking and Substance Involvement Screening Test) and the SURP-P (Substance Use Risk Profile-Pregnancy) among 500 pregnant women. SURP-P and 4P’s Plus had greater sensitivity and negative predictive values than the NIDA Quick Screen-ASSIST. Ondersma and associates compared five instruments among 1220 pregnant women: the SURP-P, NIDA Quick Screen-ASSIST, CRAFFT, 5Ps, and WIDUS (Wayne Indirect Drug Use Screener). Accuracy measured by sensitivity, specificity, and area under the curve was low for nearly all measures. There is not a single instrument that appears to be clearly superior across these two trials. Therefore, clinicians should use a validated instrument that is easily integrated into their existing electronic health record ( Box 68.1 ).
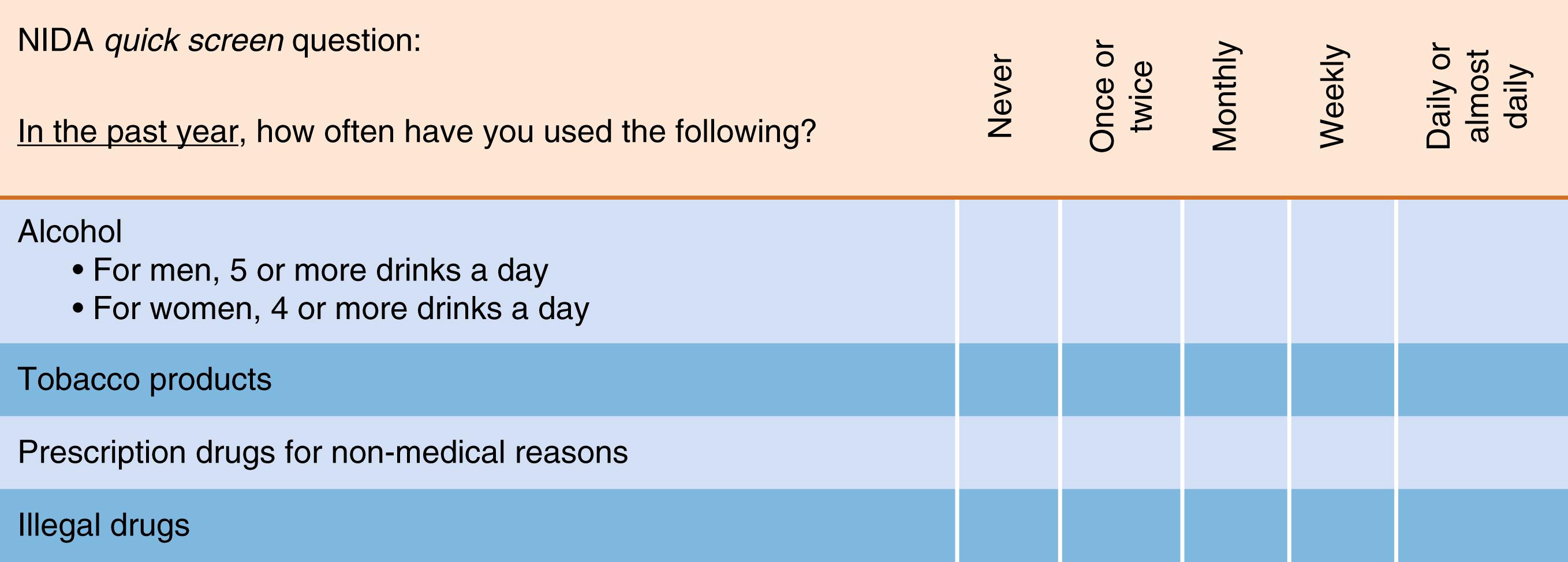
If the patient says “NO” for all drugs in the Quick Screen, reinforce abstinence. Screening is complete.
If the patient says “Yes” to one or more days of heavy drinking , patient is an at-risk drinker. Please see NIAAA website “How to Help Patients Who Drink Too Much: A Clinical Approach” http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/clinicians_guide.htm , for information to Assess, Advise, Assist, and Arrange help for at-risk drinkers or patients with alcohol use disorders.
If patient says “Yes” to use of tobacco : Any current tobacco use places a patient at risk. Advise all tobacco users to quit. For more information on smoking cessation, please see “Helping Smokers Quit: A Guide for Clinicians” http://www.ahrq.gov/clinic/tobacco/clinhlpsmksqt.htm .
If the patient says “Yes” to use of illegal drugs or prescription drugs for nonmedical reasons , proceed to Question 1 of the NIDA-Modified ASSIST.
(From National Institute on Drug Abuse. NIDA Quick Screen V1.0. https://nida.nih.gov/sites/default/files/pdf/nmassist.pdf ).
a Data from Chasnoff IJ, McGourty RF, Bailey GW, et al. The 4P’s Plus screen for substance use in pregnancy: clinical application and outcomes. J Perinatol . 2005;25:368–74; McLellan AT, Kushner H, Metzger D. The Fifth Edition of the Addiction Severity Index. J Subst Abuse Treat . 1992;9:199–213; and TWEAK (Tolerance, Worried, Eye-openers, Amnesia, K[C] Cut Down).
b From Yonkers KA, Gotman N, Kershaw T, et al. Screening for prenatal substance use: development of the Substance Use Risk Profile-Pregnancy scale. Obstet Gynecol. 2010;116(4):827.
a. Ever smoked nicotine cigarettes?
Number of cigarettes smoked in month before knowing about pregnancy
a. Ever drunk alcohol?
Number of alcoholic drinks consumed in month before knowing about pregnancy
Ever smoked marijuana?
Ever used cocaine?
Ever used sedatives, tranquilizers, sleeping pills, or other?
Ever used heroin?
Do you currently live with anyone who uses:
Alcohol
Nicotine cigarettes
Marijuana
Cocaine
Heroin
Have parents ever had problem with drugs or alcohol?
Does partner have problem with drugs or alcohol?
Number of drinks or hits or lines needed to feel effect?
In the past year, did friends or family worry or complain about drinking or drug use?
Do you drink or use drugs in the morning?
Ever been told about things you said or did while drinking or using drugs that you could not remember?
Ever felt the need to cut down on alcohol or drug use?
Hurt by someone in the home?
Feel safe at home?
Have you ever smoked marijuana?
In the month before you knew you were pregnant, how many beers, how much wine, or how much liquor did you drink?
Have you ever felt that you needed to cut down on your drug or alcohol use?
Classify the number of alcoholic drinks before pregnancy as none compared with any. Count the number of affirmative items.
0 = low risk
1 = moderate risk
2–3 = high risk
In low-risk populations, one or more affirmative items indicate a positive screen, whereas in high-risk populations, two or more affirmative items indicate a positive screen.
Most pregnant individuals report being asked about substance use during prenatal care. , In one survey, 79% of obstetrician-gynecologists reported that they “frequently” screened for substance use; however only 11% used a validated instrument. Provider gender may influence screening behavior as women obstetrician-gynecologists are more likely to “believe” in screening and use a validated instrument. Overall, integration of a validated instrument into the electronic health record, provider support through easily available resources, and skills-building to improve competence are needed to better include behavioral health assessments into prenatal care.
Screening instruments are all based upon self-report, and pregnant individuals who use drugs may have legitimate reasons for initial nondisclosure at the prenatal care visit. Reasons for initial nondisclosure include a fear of child welfare notification and prior experience of discrimination from clinicians. , Clinicians should consider asking permission prior to screening and respecting the patient’s response if screening is declined. Prenatal care unfolds over multiple visits, and the establishment of a strong therapeutic alliance, essential for all person-centered care, takes time.
Urine or other biological matrixes such as meconium or umbilical cord are not a substitute for screening for substance use, misuse, or addiction. , , Biological drug testing captures metabolites of substances present in the biological compartment at a specific moment in time. Addiction is a brain-centered condition whose symptoms are behaviors, and there is nothing in a drug test result that illuminates patient behaviors. Although urine drug screening and testing are frequently used as a component of addiction treatment, their use as a primary screening method in prenatal care is inappropriate and is not recommended. , These tests, particularly point-of-care or “presumptive” tests, have false-positive and false negative rates that differ by substance, and best practices rest upon definitive testing (via gas chromatography-mass spectrometry analysis) for clinical care decision-making. Clinicians need to be able to accurately interpret drug test results, yet physician knowledge of urine drug test interpretation is poor. Reisfield and colleagues surveyed clinicians using a 7-item scale. None answered more than 5 items correctly. , Starrels and associates used the same instrument among residents. The average score was 3, and there was no relationship between resident confidence in interpretation and actual knowledge. Given the current laws mandating child welfare notification for substance use in pregnancy and their potentially catastrophic consequence to the family, a more thoughtful and judicious use of urine drug testing is warranted, if it is to be used at all. Finally, when drug testing is deemed clinically necessary, it should only be performed following explicit maternal consent. , ,
With respect to testing the neonate, meconium (stool produced by the fetus during gestation), and umbilical cord have been used to detect substance exposure. Meconium and umbilical cord testing have relatively long windows of detection (weeks to months depending on substance); however the results between meconium and cord testing may be discordant. Clinicians should be aware of the positive and negative predictive values of testing and its substrate. Often hospital policies allow for the testing of the neonate in the event of “withdrawal” symptoms without maternal consent or even knowledge. As with maternal drug testing, clinicians should be aware of legal and ethical implications of drug testing and local reporting laws and are encouraged to openly and transparently discuss the rationale and medical use of neonatal testing. Otherwise, neonatal testing can cause lasting damage to children and their families.
Pregnant people with SUD often experience discrimination from clinicians. , It is therefore essential to use nonjudgmental, nonstigmatizing language (see Table 68.1 ) and remain centered on the pregnant person during labor, delivery, and postpartum. Concern about untreated or undertreated pain is common for people with SUD, especially those with OUD. Medications for opioid use disorder (MOUD) do not provide analgesia, and people with addiction may need more pain medication during labor. , MOUD should be continued at the same dose throughout the delivery hospitalization, and pain management should be multimodal, utilizing nonopioid medications, regional anesthesia, and opioid agonists if needed. , Hospitals should implement opioid prescribing guidelines that minimize routine prescribing, especially following vaginal delivery. Undertreated pain is likely a greater risk factor for return to substance use or SUD recurrence than judicious use of opioid agonist for postoperative pain. Pre- and postoperative MOUD discontinuation is associated with overdose and should be avoided. For people with untreated addiction, the delivery hospitalization is an important opportunity to connect them to continuing care postpartum, and everyone with SUD should receive naloxone and training in its use prior to hospital discharge.
| Stigmatizing Language | Proposed Terminology | Comments |
|---|---|---|
| Abuser; addict; street addict; former or reformed addict; alcoholic, boozer; crackhead, cokehead; pothead, weed user; dope addict; narco; junkie; druggy; tweaker; dope fiend; alkie; lush | Person with substance use disorder or addiction Person in remission from a substance use disorder |
Some of these terms can refer to a person with or without a substance use or behavior disorder. A disorder is diagnosed if the DSM-5 criteria for use or behavior disorder are met. |
| Having a drug habit or bad habit; having a drug of choice, drug of abuse | Having a [substance use or behavior] disorder or addiction involving [substance use or behavior] | Addiction is a chronic disease, not a habit; the term “habit” or “choice” implies that it is merely a problematic behavior and something that a person can “fix” by simply desiring a change. “Cigarette habit” and “heroin habit” are examples of such problematic terms. |
| Smoker | Person with cannabis and/or tobacco or nicotine use disorder, or addiction involving cannabis/tobacco/nicotine use | With the increasing use of vaping and e-cigarettes, it is suggested to use the term “nicotine” rather than “tobacco” as it encompasses both tobacco chewing and smoking, and the use of noncombustible nicotine delivery systems. |
| Addicted baby; crack baby; meth baby | Neonate (or newborn, child) with [substance] withdrawal; or with neonatal withdrawal syndrome; or with in utero exposure to [named substance] | Children can be exposed in utero to substances. They can develop a physical or physiological dependence with prolonged in utero exposure to certain substances that can lead to a withdrawal syndrome postbirth. They are not born with addiction—they do not meet the diagnostic criteria for SUD. |
| Being clean or sober | Being substance-free. Being abstinent. Being in remission. Toxicology testing “negative” for a [substance] | Remission occurs when the symptoms of a disease subside. Recovery extends beyond the remission phase. |
| Being dirty | Using [substances]; Toxicology testing “positive” or “unexpected” result | “Dirty urine” implies that the person is a “dirty” person. |
| Getting/being high; stoned; wasted | Being intoxicated; being under the influence of [substance] | |
| Shooting up; jacking up; slamming; banging; pinning | Intravenous drug use; injection drug use | Intravenous drug use refers to substance use and does not automatically mean that the individual has addiction. |
| Kicking the habit | Initiate abstinence; receive/ start treatment; enter remission, etc. | The commonly used phrase “kick the habit” implies that it is a habit not a disease, and that the “treatment” occurs simply based on sufficient willpower to stop the behaviors. |
| Being in detox | Undergoing a detoxification treatment; withdrawal management/treatment; tapering off medications | |
| Being in rehab | Undergoing intensive addiction treatment or management; intensive pain rehabilitation or restoration program | |
| Replacement or substitution treatment for OUD; Medication-Assisted Treatment (MAT) | Medication treatment; pharmacotherapy | Misconceptions about agonist medications buprenorphine and methadone (such as “they replace one addiction for another”), imply that this evidence-based treatment for OUD is a continuation of drug use; statements that people treated with agonist medications are not in remission because they are not “drug free” convey a similar message. Using the term “medication-assisted treatment” can imply that medication per se is not a treatment. Because the acronym MAT has now deep cultural roots, the change to “medications for addiction treatment” could preserve the commonly-used acronym while changing its full name to a nonstigmatizing one. |
| Having dirty/clean urine | Toxicology testing positive/negative for a [substance]. Results are unexpected/expected; inconsistent/consistent with the prescribing record | |
| Recidivism | Remission Return to use |
The vast majority of individuals will achieve abstinence from substance use during pregnancy. Unfortunately, within one year postpartum, 80% of postpartum individuals will have a return to substance use. Clinicians should be aware of both patient-level factors and systems-level issues that create potentially destabilizing situations for postpartum individuals with substance use and SUD. Important considerations, including physiological changes of the postpartum period, potential destabilization of maternal mental health, demands of a newborn, and social stressors, place postpartum individuals at increased risk of return to use, SUD symptom recurrence (e.g., cravings, uncontrolled use), and overdose. Non–patient-related factors, including stigmatization of SUD, provider lack of knowledge of evidence-based approach to addiction treatment, lack of accessible SUD treatment and mental health care for parenting individuals, and loss of insurance are also contributing factors to return to use and overdose. Punitive policies that define substance use as child abuse or neglect increase the likelihood of adverse outcomes including neonatal abstinence syndrome (NAS) and preterm birth, which in turn increase the risk of maternal return to use and subsequent overdose. Several studies have also found an association between child protective service involvement, loss of custody, and discontinuation of addiction treatment postpartum. Particularly for individuals with OUD, MOUD discontinuation in the postpartum period is a significant risk factor for return to use and overdose. , Clinicians should strongly recommend continuation of MOUD during the postpartum period to prevent destabilization. Postpartum depression or exacerbation of underlying mental health conditions in the postpartum period, intimate partner violence including financial abuse, and disruption of interpersonal relationships may all lead to treatment disengagement. Clinicians should be aware of the risk factors and sequelae of treatment disengagement and engage in supportive conversations with postpartum individuals to illuminate and address barriers to continued care.
Optimization of postpartum care is critically needed for women with addiction and mental health concerns, including frequent and early follow-up after delivery, extending up to a year postpartum. SUD is a lifelong condition requiring chronic, rather than episodic or acute, care. Ongoing conversations about postpartum stress including ensuring adequate postpartum support, education about signs of postpartum depression and anxiety, plan for sleep and medication management, creating a plan of safe care including in the event of return to use, and discussing the role of child protective services are critically important. Because of high rates of unintended pregnancy and short pregnancy intervals among individuals with SUDs, full-spectrum contraceptive choices should be offered both in the prenatal and in the postpartum periods. Care should be taken to elicit and respect the postpartum individual’s reproductive goals during contraceptive counseling. Finally, clinicians caring for postpartum individuals who are transferring care to other providers should provide warm handoffs and MOUD and other medication continuation to avoid abrupt cessation and potential destabilization.
In subsequent sections, we will review substance-specific data available on breastfeeding. Here we focus on the overarching principles with respect to breastfeeding among lactating individuals. The American Academy of Pediatrics policy is that maternal substance use is “not a categorical contraindication to breastfeeding”; however, breastfeeding in the context of illicit substance use is not recommended due to a paucity of neurodevelopmental outcomes among the breastfed child in the setting of maternal illicit substance use. Most importantly, it is imperative for clinicians to recognize that recommendations for breastfeeding in the setting of maternal substance use is largely based on expert opinions, rather than high-quality data on maternal and neonatal outcomes. Data on health and developmental outcomes of breastfed children in the setting of maternal substance use are primarily available for legal substances such as tobacco and alcohol. , There is an almost complete lack of data on outcomes among breastfed children of lactating individuals who used illicit substances. These limited studies focus almost entirely on drug pharmacokinetics (presence of metabolites) among a small number of lactating individuals. Few studies examine the potential harm of recommending against initiation or cessation of breastfeeding in the setting of substance use. For example, while breastfeeding is well established to lower the risk of sudden infant death syndrome (SIDS), and passive tobacco exposure increases the risk of SIDS, it is still unknown to what extent breastfeeding is protective for infants of mothers who smoke. In other words, the question is not merely “is a substance present in breast milk?” but rather “in the absence of data demonstrating harm, does the presence of a substance in breast milk outweigh the harm of withholding breast milk from an infant?” These recommendations must be carefully weighed against the well-documented benefits of breastfeeding for maternal well-being, maternal-infant attachment, and infant development. In counseling women about lactation, clinicians should be aware of the available data for both benefits of breastfeeding and potential harm of substance exposure and engage in a shared decision-making approach to maximize maternal and child outcomes. Ideally, as outlined in the Academy of Breastfeeding Medicine, clinicians and lactating individuals collaboratively establish a breastfeeding plan that balances maternal goals, maternal and infant well-being and safety, encouragement of addiction treatment engagement, utilization of available support systems including nonjudgmental health care providers, and harm-reduction plans in the event of return to use.
Issues regarding child welfare notification for maternal substance use and/or newborn withdrawal are among the most vexing for clinicians. The periodic federal reauthorization of the Child Abuse Prevention and Treatment Act (CAPTA), coupled with state statute compliance, is difficult to track. In addition, hospital-specific policies, when they exist, are not always in alignment with this shifting landscape, and heterogeneity of local child welfare responses are common. State policies related to substance use in pregnancy are becoming more punitive in the United States. , This trajectory is driven by increasingly restrictive reproductive health policies rather than general drug policy which is becoming less punitive. As of January 2021, there were 25 states and the District of Columbia which mandated reporting for drug use in pregnancy and 3 states in which drug use in pregnancy was grounds for civil commitment. The assumption that addiction in pregnancy is associated with subsequent child abuse or neglect is not supported by clinical evidence. There is similarly no evidence of benefit in terms of either maternal health or child development from a child welfare report due to substance use in pregnancy, whereas the harms are well detailed. Page 5
Child welfare does not provide support. Agencies do mandate treatment, but they lack the authority to provide resources, and the actual provision of care remains the responsibility of the child welfare–involved person. The primary service provided by child welfare is surveillance, and there are marked racial inequities within the “womb-to-foster-care pipeline.” , Although universal drug testing at the time of delivery has been proposed as a strategy to prevent or minimize the racism of selective reporting, population health data demonstrate a persistence of racial inequities in child welfare reporting following implementation of universal testing.
Clinicians need to understand not just their local landscape of child welfare mandates, but also what child welfare as an agency does and does not provide. More importantly, we should evaluate the prioritization of legal interference over patient care and public health and consider the practice of medicine to include resistance to systems that perpetuate inequality. ,
Substance use and, in particular, untreated substance use disorders are a direct and strong risk factor for maternal death. However, the ability to accurately quantify the number of drug-related deaths among pregnant and postpartum individuals is difficult, partly due to epidemiological reporting and tracking of maternal deaths. In the United States, maternal deaths are tracked through three national surveillance mechanisms: National Vital Statistics System, the Pregnancy Mortality Surveillance System, and state-based maternal mortality review committees (MMRC). Data from these surveillance systems indicate that drug-related deaths now account for a significant proportion of pregnancy-associated (death in pregnancy or within one year of end of pregnancy) and pregnancy-related deaths (death directly attributable to pregnancy and the postpartum period). , While most drug-related deaths are considered pregnancy-associated, MMRC have recently developed criteria to determine whether drug-related and mental health–related deaths are pregnancy-related. Because of the variable definitions and monitoring systems across states, it is currently difficult to compare drug-related deaths among pregnant and postpartum individuals across states.
Significant knowledge gaps exist regarding the circumstances surrounding drug-related deaths among pregnant and postpartum women, hampering efforts to reduce or prevent these deaths. , The vast majority of drug-related pregnancy-associated deaths occurred in the postpartum year. , , , , , Among women with accidental drug-related deaths in Utah from 2015–16, the most common pregnancy-related cause was maternal destabilization after removal of custody of an infant, ultimately leading to death. Many pregnant and postpartum individuals do not spontaneously disclose substance use to clinicians, and multiple studies confirm that universal systematic screening is the exception, rather than the rule. Systematic underrecognition of substance use among pregnant and postpartum individuals who died of drug-related deaths is significant. , , This is particularly concerning as contact with the health care system is not uncommon prior to maternal death. In California and Massachusetts, prior to a drug-related death or overdose event, nearly two-thirds had at least one emergency department visit or inpatient hospital admission, suggesting many pregnant and postpartum individuals offer the health care system an opportunity to intervene and potentially prevent their deaths. , Lack of systematic screening may also be due to clinicians’ lack of knowledge and skills to intervene. Many clinicians, particularly those practicing obstetrics, receive no or minimal education on addiction in their training. , While medical school curricula increasingly emphasize the fundamentals of SUD treatment, many clinicians lack basic skills in managing medications, including buprenorphine, methadone, and naltrexone, or basic harm-reducing interventions including motivational interviewing, naloxone coprescription, and anticipatory guidance about return to drug use, overdose, and death. And even fewer provide instruction on specific considerations for the pregnant and postpartum population, including dosing considerations and recommendations against medication tapering or discontinuation in pregnancy. , The collective lack of knowledge about addiction in maternal-fetal medicine is likely one contributing factor to low rates of MOUD utilization and continuation in the obstetrical population. , Overall, it is well recognized that substance use and addiction are important factors in addressing and preventing maternal deaths in the United States, and further data are urgently needed to address contributing factors and preventability of these devastating deaths.
In the following section, we review class-specific information on tobacco and nicotine-containing products, alcohol, cannabis, opioids, stimulants (cocaine and methamphetamine), and benzodiazepines, with specific attention to impact on maternal-fetal health. For each class, we review the prevalence; pharmacology; screening; maternal, fetal and child outcomes; and treatment recommendations.
In the United States, tobacco continues to be the most common substance used in pregnancy ( Fig. 68.1 ). Based on birth certificate data, 7.2% of pregnant individuals smoked at any time during the pregnancy in 2016. The highest prevalence was in West Virginia (25.1%) and the lowest in ten states where it was <5%. There are significant differences in smoking prevalence by maternal characteristics. Prevalence of tobacco smoking was highest among pregnant individuals 20–24 years old (10.7%), followed by those 1–19 years old (8.5%) and those 25–29 (8.2%). With respect to race and ethnicity, non-Hispanic American Indian or Alaska Native individuals had the highest prevalence of smoking tobacco in pregnancy (16.7%) and non-Hispanic Asian women had the lowest (0.6%). In terms of education, smoking was highest in pregnancy among those who completed high school (12.2%) followed by those with less than a high school education (11.7%). Importantly, comparisons of maternal self-report with detection using biochemical markers, specifically urine metabolites of nicotine, indicate potentially underreporting or underrecognition of exposure to second-hand smoke.

Overall trends suggest substantial decreases in smoking among pregnant individuals over the past two decades; however, this decline has been more robust in some populations compared to others. For example, from 2007–16, there was a 17% greater reduction in smoking among urban individuals compared to those living in rural areas. Among pregnant individuals with OUD, smoking prevalence is as high as 50%–95% and there are few data to suggest a substantial decrease in this population.
While the reduction of smoking cigarettes among pregnant individuals nationwide is promising, this reduction must be interpreted with caution as it may not represent e-cigarettes (vaping), hookah, and cigars among pregnant individuals. Vaping, the common term for use of electronic cigarettes, is the process of inhaling aerosol typically containing nicotine, flavoring, and other additives. In 2015, 7.0% of individuals with a recent live birth in Oklahoma and Texas reported vaping prior, during, or after pregnancy; of these individuals, 1.4% vaped during pregnancy. Although most reported that they were vaping nicotine products, over a quarter reported not knowing if the product contained nicotine. Several studies suggest that among pregnant individuals vaping is perceived as a safer alternative to smoking and utilized for smoking cessation. In 2021, the United States Preventive Services Taskforce (USPSTF) issued a statement that there continues to be insufficient evidence to assess risks and benefits of vaping/e-cigarettes for tobacco cessation in adults including pregnant individuals.
The addictive properties of nicotine arise from dopaminergic effects on the brain, and the frequency of dosing with tobacco products likely contributes to both reward and reinforcement as well as intensity of withdrawal symptoms felt when attempting tobacco cessation. Nicotine rapidly reaches peak levels in the bloodstream and enters the brain, where peak levels are reached within 10 seconds after inhalation. Immediately after nicotine exposure, the adrenal glands are stimulated and epinephrine is released, causing an increase in blood pressure, respiration, and heart rate, which impacts maternal-fetal perfusion.
The most common nicotine-containing product used among reproductive age and pregnant individuals remains tobacco cigarettes. , The major psychoactive product in tobacco is nicotine but there are 4000 other substances involved in tobacco combustion including tar, carbon monoxide, acetaldehyde nitrosamines, ammonia, polycyclic aromatic hydrocarbons, and hydrogen cyanide. Cigarette smoking is a highly efficient means of nicotine delivery; the average person smoking inhales 1 to 2 mg of nicotine per cigarette and will take 10 puffs on a cigarette in approximately five minutes.
Noncombustible forms of nicotine including electronic nicotine deliveries systems (ENDS), dissolvable tobacco, and snus, a powder smokeless tobacco product, are increasingly used by reproductive-age and pregnant individuals. , ENDS include e-cigarettes and other vaping products such as vape pens, vaporizers, mod or pod systems, hookah pens, and e-pipes. ENDS produce carbonyl compounds (formaldehyde, aldehyde, acetone, acrolein), volatile compounds (benzene and toluene), and heavy metals (zinc, copper, lead, arsenic), which are inhaled and likely cause acute lung injury and other adverse health outcomes. , The Centers for Disease Control and Prevention (CDC) has issued advisories about thousands of serious lung injuries and dozens of deaths associated with vape products and e-cigarettes. , These injuries are likely due to vitamin E acetate, a thickening agent most commonly found with informal sources of Δ-9-tetrahydrocannabinol (THC) or nicotine vape products. Pregnant and lactating individuals should be advised that alternative nicotine-containing products have similar risks of maternal, fetal, and infant adverse outcomes as cigarette smoking and that discontinuation is strongly advised. ,
In the most recent guideline, the USPSTF recommends that clinicians screen all adults, including pregnant individuals, using methods such as the Five A’s: Ask, Advise, Assess, Assist, Arrange. The American College of Obstetricians and Gynecologists (ACOG) supports the Five A’s approach to screening all pregnant individuals for use of any nicotine-containing products, in conjunction with screening for alcohol and other substance use. ACOG’s suggested approached tailored to pregnant individuals is outlined in Fig. 68.2 . However in practice, many clinicians are much more likely to only ask (98%) and advise (66%) but far less likely to assess (42%), assist (29%), or arrange for follow-up visits or referrals (6%). An important consideration in the operationalization of interventions for tobacco cessation among pregnant individuals is that guidelines do not take into account gender. Women report more perceived stress than men, and this stress is more highly correlated with nicotine withdrawal among women than men. Among pregnant individuals who have quit smoking, postcessation craving and withdrawal symptoms may decrease less than among nonpregnant individuals, which may lead to return to use. Knowledge of these gender differences may help clinicians address challenges pregnant and postpartum individuals may face in achieving tobacco reduction and cessation.

Cotinine is the primary metabolite of nicotine that is measured in both urine and saliva drug tests. , Cotinine levels are able to distinguish between active and passive exposure in a pregnant individual. , and can identify passive exposure in infants and children. Recently, third-hand exposure to tobacco (e.g., furniture residue, particles on hands or clothing) has been associated with elevated levels of cotinine in infants in a neonatal intensive care unit.
The risks associated with tobacco or other nicotine product exposure during pregnancy are well described and profound. Use of tobacco and other nicotine-containing products is the leading modifiable cause of preterm delivery (<37 weeks) in the United States. , It is also causally associated with miscarriage, stillbirth, fetal growth restriction, and sudden infant death syndrome. , Increased maternal and perinatal risks include spontaneous abortion (1% relative risk increase per cigarette smoked per day), stillbirth, placental abruption, placenta previa, preterm delivery, , low birth weight (LBW), and ectopic pregnancy, in addition to postnatal associations with neonatal death and SIDS. Pregnant individuals who smoke have a higher risk for deep venous thrombosis, stroke, pulmonary embolus, myocardial infarction, and pulmonary complications such as influenza, pneumonia, and bronchitis. Pregnant individuals who smoke may, in fact, have a reduced risk for preeclampsia. , Examining the potential mechanisms by which maternal smoking affects these outcomes is an important step in reducing smoking-related morbidity and mortality.
The American Academy of Pediatrics (AAP) historically opposed breastfeeding while utilizing nicotine-containing products. However in its 2012 policy statement, the AAP clearly states that smoking is not an absolute contraindication to breastfeeding. However, smoking may diminish the protective effects of breastfeeding against respiratory infection and SIDS. Among lactating individuals who smoke, nicotine is found in breast milk in concentrations 3 times greater than in maternal blood plasma. However, newer nicotine products may expose infants to high concentrations with slower clearance. For example in a small Swedish study, 8 of 13 (61%) lactating individuals using snus had detectable nicotine after 11 hours of abstinence, whereas all 6 lactating individuals who smoked cigarettes had no detectable levels after four hours of abstinence. Research indicating that such concentrations constitute a health risk to the infant is lacking.
Maternal smoking can result in impaired fetal oxygen delivery, as demonstrated by structural changes in the placentas of individuals who smoked during pregnancy. A reduction in fraction of capillary volume and increased thickness of the villous membrane likely contribute to impaired gas exchange. Smoking acutely decreases intervillous perfusion, a possible effect of vasospasm. Direct toxicity from the other substances found in cigarettes besides nicotine may also influence pregnancy outcomes. Carbon monoxide contributes to formation of carboxyhemoglobin, which is cleared slowly from the fetal circulation and causes a left shift of the oxyhemoglobin dissociation curve. , Maternal smoking is also associated with increased resistance in uterine, umbilical, and fetal middle cerebral arteries, which likely explains the causal relationship to fetal growth restriction. Epidemiological studies do suggest a higher risk of small-for-gestational age (SGA) infants among individuals who only vaped in late pregnancy (16.5%, adjusted OR = 2.4; 95% CI, 1.0–5.7), those who only smoked (20.8%, adjusted OR = 2.4; 95% CI, 1.8–2.9), and those who smoked and vaped (20.1%, adjusted OR = 2.3; 95% CI, 1.3–4.1) compared to those who neither smoked nor vaped (8.9%). In this same study, there was an increased risk of preterm delivery among individuals who only smoked (11.7%, adjusted OR = 1.6; 95% CI, 1.2–2.0), no increased risk among individuals who only vaped (7.8%, adjusted OR = 1.6; 95% CI, 0.7–3.4) or who smoked and vaped (7.9%, adjusted OR = 1.3; 95% CI, 0.8–2.3) compared to those who did not smoke or vape (7.6%).
Smoking may also result in direct genotoxicity, leading to chromosomal instability, which is seen more commonly in individuals who smoke compared to those who do not smoke. De la Chica and colleagues published a study of 25 pregnant individuals who smoked and 25 who did not smoke undergoing amniocentesis. Amniocytes were evaluated for structural abnormalities. Twelve percent of participants who smoked and 3.5% of those who did not smoke demonstrated genetic instability ( P < .002). The most common location of deletion or translocation was in the 11q23 region, which is implicated in hematologic malignancies. Other studies have also indicated that tobacco compounds may cross the placenta and induce chromosomal losses and breaks. The results of these studies suggest, but do not confirm, the association of prenatal smoking exposure with childhood cancer.
A teratogenic risk associated with tobacco has been suggested, although no malformation syndrome has been identified. The suggested malformations linked to smoking include talipes, craniosynostoses, cleft lip or palate, urinary tract malformations, cardiac malformations, and limb reduction defects. The data on malformations vary and do not represent a consistent pattern ( Table 68.2 ). In a review of first-trimester nicotine exposure in the Danish National Birth Cohort (1997–2003), there was no association with smoking for all anomalies. However among children with prenatal nicotine replacement therapy (NRT), there was an increased relative prevalence rate ratio of 1.61 (95% CI, 1.01–2.58) for any anomaly and 2.62 (95% CI, 1.53–4.52) for musculoskeletal anomalies compared to no exposure. However, a subsequent meta-analysis of NRT use in pregnancy showed studies were generally of poor quality and findings were not in a consistent direction. Another comprehensive systematic review and meta-analysis of studies published from 1959–2010 including 173,687 cases of congenital anomalies and over 11 million controls showed a pattern of increased anomalies with maternal smoking. While there is much less supportive data, paternal smoking is also increasingly associated with congenital anomalies. However, it remains unclear if this is due to DNA changes, mutations in sperm, second-hand smoke, or other causes.
| Malformation | Study | Findings |
|---|---|---|
| Craniosynostoses | Kallen, 1999 | First-trimester maternal smoking related to isolated craniosynostoses |
| Alderman 1997 | Smoking associated with increased risk of craniosynostoses (OR = 1.7; 95% CI, 1.2–2.6) Smoking of more than one pack per day, the relative odds 3.5 (95% CI, 1.5–8.4) |
|
| Honein and Rasmussen, 2000 | Possible dose-response relationship between maternal smoking and craniosynostoses, although not statistically significant | |
| Kallen and Robert-Gnansia, 2005 | No significant association between craniosynostoses and smoking | |
| Carmichael et al., 2008 | No significant association between outcome and smoking | |
| Cleft lip or palate | Hwang et al., 1995 | Dose dependence of maternal smoking and transforming growth factor-α (TGF-α) polymorphism associated with outcome |
| Shaw et al., 1996 | Dose dependence of maternal smoking and TGF-α polymorphism associated with outcome | |
| Kallen, 1997 | Association of smoking and facial clefting without evaluation of genetic polymorphisms | |
| Chung et al., 2000 | Association of smoking and facial clefting without evaluation of genetic polymorphisms | |
| Little et al., 2004 | Meta-analysis shows increased risk for cleft lip, with or without cleft palate (RR = 1.34; 95% CI, 1.25–1.44) Cleft palate (RR = 1.22; 95% CI, 1.10–1.35) |
|
| Shi et al., 2007 | Absence of GSTT1 gene associated with facial clefting in smokers | |
| Urinary tract abnormalities | Li et al., 1996 | Increased risk for outcome in association with light smoking |
| Shnorhavorian et al., 2011 | No association between maternal tobacco use and outcome | |
| Gastroschisis | Hawkshaw et al., 2011 | Pooled OR = 1.50; 95% CI, 1.28 –1.76 |
| Congenital heart disease | Kallen et al., 1998 | Association between congenital heart defects and smoking |
| Malik et al., 2008 | Maternal smoking associated with septal and right-sided heart defects | |
| Hawkshaw et al., 2011 | Pooled OR = 1.09, 95% CI, 1.02–1.17 | |
| Limb reduction abnormalities | Kallen, 1997 | Association between limb reduction defects and smoking |
| Czeizel et al., 1994 | Association between limb reduction defects and smoking | |
| Man and Chang, 2006 | Association between limb reduction defects and smoking | |
| Kelsey et al., 1978 | No association between limb reduction defects and smoking | |
| Shiono et al., 1986 | No association between limb reduction defects and smoking | |
| Van den Eeden et al., 1990 | No association between limb reduction defects and smoking |
Multiple studies now indicate that maternal smoking is associated with low birth weight (LBW), 186,187 child overweight, and later psychological problems. There may be genetic susceptibility that helps to explain why some individuals who smoke are more vulnerable to adverse perinatal outcomes. CYP1A1, GSTM1, and GSTT1 genes encode for enzymes that participate in the elimination of toxic substances contained in cigarette smoke. Individuals who smoked with CYP1A1 heterozygous and homozygous variants (Aa/aa) and absence of GSTT1 (deletion) had significantly greater reductions in infant birth weight than those homozygous for the wild-type CYP1A1 (AA) or with an extant GSTT1 genotype. Another study found the GSTT1 deletion to be associated with a significant reduction in gestational age–adjusted birth weight among the offspring of smoking mothers.
Recent studies have shown that maternal smoking may directly impair lung development, which may explain why some children have measurable defects on pulmonary function testing, independent of environmental exposure to tobacco smoke at birth. Nicotine may interact with nicotinic acetylcholine receptors (nAChRs), which in primate models appear to be abundant in fetal lung tissue. The same investigators demonstrated that continuous nicotine infusion into pregnant rhesus monkeys resulted in significantly decreased lung weight and volume and increased airway resistance. The same maternal genotype that increases the risk for LBW may also affect the pulmonary function in the offspring with prenatal nicotine exposure. When spirometry was performed on the offspring of 370 individuals who smoked, maternal smoking was found to be associated with decreased lung function, particularly in those children 6 to 10 years of age whose mothers had the CYP1A1 Aa/aa and GSTM1 -absent genotype. These studies suggest a unique interplay between genetics and environment and shed light on the outcomes previously identified as being associated with smoking.
Pregnancy is a uniquely motivating time, especially when coupled with frequent interaction with a provider, to reinforce smoking abstinence and lend support. Nearly half (45%) of pregnant individuals who smoked stop completely by the end of pregnancy. Pregnant individuals who are most likely to quit completely have generally already done so by the time of their first prenatal visit, but those who still smoke at their first prenatal visit are likely to continue to smoke throughout their pregnancy without an effective intervention. Importantly, nearly half (42%) of postpartum individuals who quit use in pregnancy have a postpartum return to use.
The USPSTF recently concluded with high certainty (“A” rating) that behavioral interventions for smoking, preceded by screening and brief advice (such as the Five A’s approach), provide a net benefit for pregnant and nonpregnant adults. Behavioral interventions have consistently been shown to be effective in decreasing smoking in pregnancy. In a Cochran review of behavioral interventions, primarily cognitive-behavioral therapy and contingency management, there was a significant reduction in smoking in late pregnancy following interventions (risk ratio [RR] = 0.94; 95% confidence interval [CI], 0.93–0.96), and an absolute difference of six in 100 women who stopped smoking during pregnancy. These interventions, even late in pregnancy, appear to have potential to decrease LBW and preterm births. In one study, a voucher-based contingency management program (in which individuals who abstained from smoking earned vouchers exchangeable for retail items) was effective in promoting abstinence (34.1%, compared with 7.4% among those who received a voucher regardless of smoking status) and also improved mean birth weight and decreased the percentage of LBW babies. Additionally, new electronic and web-based interventions are increasingly available. Pregnant individuals using tobacco receiving e-SBI, a validated web-based electronic behavioral intervention, are ten times more likely to achieve abstinence compared to those receiving usual care.
While there is robust data to support behavioral intervention among pregnant individuals, there is insufficient evidence for medications as few studies include this population. In contrast, the USPSTF concluded that the benefit of US Food and Drug Administration (FDA)-approved medications for tobacco smoking cessation in nonpregnant adults who smoke is substantial . Current FDA-approved medications for nicotine use disorder are NRT (nicotine replacement therapies including nicotine transdermal patches, lozenges, gum, inhalers, or nasal spray), bupropion hydrochloride sustained release, and varenicline. A recent Cochrane review on medications included 11 trials of 2412 pregnant individuals who smoked at time of study; nine were trials of NRT and two trials of bupropion as adjuncts to behavioral interventions and controls with behavioral interventions. There were no trials assessing varenicline or electronic cigarettes. NRT was associated with smoking cessation in late pregnancy, although quality of the data was low (RR = 1.37; 95% CI, 1.08–1.74; I 2 = 34%, 9 studies, 2336 women). There was no evidence of a difference between NRT and control groups for adverse perinatal outcomes including miscarriage, stillbirth, premature birth, birthweight, low birthweight, admissions to neonatal intensive care, cesarean delivery, congenital abnormalities, or neonatal death. While NRT is widely used in pregnancy, studies have failed to demonstrate efficacy in tobacco cessation and these products do contain nicotine, which raises concerns of associated adverse perinatal outcomes. , , There is also no evidence that bupropion was effective for smoking cessation during pregnancy, although the two available studies are limited. While bupropion did not demonstrate efficacy, there was no evidence that it is unsafe in pregnancy and breastfeeding and the benefits may outweigh risks.
Recent data suggest that sex and gender substantially impact efficacy of medications for nicotine use disorder. Sex differences include differences in GABA receptor associated with increased tobacco cravings among women, whereas gender differences relate to social stigma around smoking while pregnant and motivations for tobacco cessation. Compared to men, women are less likely to achieve smoking cessation. Women have different response rates to the three FDA-approved options. , Varenicline, a partial nicotinic receptor agonist selective for α 4 β 2 nicotinic acetylcholine receptor subtypes, reduces tobacco craving, withdrawal symptoms, and the reinforcing effects of smoking relative to placebo, bupropion, and transdermal nicotine patch. This pathway may be particularly important as women have more cravings and withdrawal symptoms than men. , , , Two meta-analyses of pharmacotherapy trials of over 14,000 individuals (7000 women) demonstrate that varenicline appears to be the most effective medication among nonpregnant women. , Among nonpregnant women, varenicline is more efficacious than NRT (RR = 1.41; 95% CI, 1.12–1.76) and bupropion (RR = 1.38; 95% CI, 1.08–1.77).
While varenicline has not been systematically studied among pregnant persons, there is some available dating suggesting safety. In preclinical studies, administration of varenicline to pregnant rats and rabbits at doses 36–50 times higher than human doses based on serum concentration did not demonstrate any increased risk of congenital anomalies. In four human cohort studies and one case report, no evidence of maternal or fetal harm was identified. Available safety data on varenicline in pregnancy, although limited, are reassuring, making this a promising intervention in this population, although it should be used with caution with lactating women.
Given the magnitude of impact that nicotine and tobacco products have on reproductive, pregnancy, and child outcomes, research on interventions focused specifically with this population are urgently needed. An annual decrease of one percentage point in maternal smoking prevalence would prevent 1300 LBW deliveries. Using a conservative estimate that 4% of all preterm deliveries are directly attributable to prenatal smoking, effective smoking cessation interventions for pregnant individuals could save $232 million annually. In summary, data on effective interventions are currently lacking and have the potential to substantially impact short- and long-term maternal, fetal, and child outcomes.
CDC messaging around alcohol and pregnancy is clear: there is no known safe amount, safe time, or safe type of alcohol to consume during pregnancy or while trying to get pregnant. Despite public health campaigns, however, current patterns of use demonstrate limited adherence to these recommendations. Recent data from the National Survey on Drug Use and Health (NSDUH) estimate that, among pregnant women aged 12–44 years, 64.7% report drinking within the past year, 19.6% of people in the first trimester report drinking within the past month, and 4.7% of people in their second or third trimester report drinking in the past month. Binge drinking (more than three drinks in a single occasion in the past month) was reported by 10.5% of people in the first trimester and 1.4% in the second or third trimester. Alcohol use in pregnancy varies by state, and in some states, the highest prevalence was reported among women older than 35 years of age, non-Hispanic women, women with more than a high school education, and women with higher income. These findings suggest that alcohol use in pregnancy is prevalent across a variety of demographic groups.
Alcohol acts as an antagonist at N -methyl- d -aspartate (NMDA) receptors and as a facilitator at γ-aminobutyric acid (GABA) receptors. It also interacts with endogenous opioids and with serotonin and dopamine systems. Alcohol stimulates dopamine release specifically from the nucleus accumbens, and this stimulation is thought to be involved in the initiation of alcohol reinforcement. Different responses in blood alcohol levels among individuals ingesting the same amount of alcohol may be explained by polymorphisms in the alcohol dehydrogenase gene. Maternal polymorphisms in the ADH1B gene are hypothesized to affect peak blood alcohol levels by altering alcohol metabolism. These polymorphisms may correlate with the risk for adverse fetal effect. Additionally, the difference in abundance and efficiency between maternal and fetal enzymes results in reduced fetal alcohol elimination, prolonged fetal exposure, and the development of fetal adverse effects.
The US Preventive Services Task Force recommends screening for unhealthy alcohol use in primary care settings for adults 18 years or older, including pregnant individuals, and providing persons engaged in risky or hazardous drinking with brief behavioral counseling interventions to reduce unhealthy alcohol use. Similarly, ACOG recommends screening, though the committee opinion is a bit out of date. The Society of Obstetricians and Gynaecologists of Canada has published a recent and excellent guideline for screening and counseling for alcohol consumption during pregnancy. They recommend universal screening with a single nonjudgmental question. Anyone who consumes alcohol should then be further screened with either the AUDIT-C or T-ACE, and those that screen positive should be provided a brief intervention. The AUDIT-C is a three-item survey that is validated in pregnancy and among women in general. The T-ACE is a variation of the CAGE questionnaire validated for pregnant women and also useful for identifying at-risk drinking. The four T-ACE questions address T olerance, A nnoyance, the need to C ut down, and the use of E ye-openers.
Questions that pose alcohol drinking (or use of tobacco or other drugs) as a normative behavior may be more sensitive in providing accurate results, rather than asking a woman to endorse or deny any use, because the latter approach biases the woman’s response toward denying use. Because any use during pregnancy is considered to be significant, a clinician’s screening may feasibly be accomplished with a single question: “How much beer, wine, or other alcoholic beverages do you consume in an average week?”
Recent survey data supports screening acceptability for alcohol as part of prenatal care. Self-administered survey data coupled with structured interviews at four prenatal clinic sites in Louisiana and Maryland found that nearly all pregnant women found screening acceptable for alcohol (97%), with acceptability rates higher for those reporting binge and risky drinking, and 99% reported they would disclose their alcohol use if screened.
Toxicology testing for alcohol use without the patient’s consent is not endorsed except in the case of significant impairment and intoxication. Acute use can be captured in serum and breathalyzer. Although many biomarkers have been evaluated in the literature over the past three decades, none are established or recommended for routine clinical care.
Women are uniquely affected by alcohol. Because of their differing alcohol-processing abilities, women demonstrate a higher blood alcohol level than men when exposed to the same dose, and they suffer alcohol-related illness at lower levels of alcohol exposure than men. Some studies suggest that women are more likely to demonstrate cognitive and motor impairment, and they may be more likely than men to suffer physical harm and sexual assault when using alcohol. Importantly, the increased risk of sexual assault is due to gender-based violence perpetrated against women, including pregnant individuals. Alcohol has effects on all aspects of reproduction, including fertility, fetal anomalies, and lactation. Kesmodel and colleagues correlated the risk for stillbirth with maternal consumption of alcohol in a Danish cohort of 24,768 mothers. The rate of stillbirth was increased across all categories of maternal alcohol use, even after adjusting for potentially confounding variables that included smoking, caffeine intake, prepregnancy weight, and parity. The rate of death from otherwise unexplained stillbirth ranged from 1.37 cases per 1000 women consuming less than one drink per week to 8.83 cases per 1000 women consuming five or more drinks per week (RR = 2.96; CI, 1.37–6.41).
The AAP recommends that the ingestion of alcoholic beverages be minimized and limited to an occasional intake of no more than 0.5 gm per kg body weight (maximum 2 oz liquor). Women who do drink while breastfeeding should be advised to have no more than one drink and to wait at least 2 hours after this drink before breastfeeding to minimize its concentration in ingested milk. These recommendations limit but do not prevent newborn alcohol exposure through breast milk. Within an hour of ingestion, alcohol concentration in breast milk resembles that in maternal blood, and newborns metabolize alcohol at half the rate of adults. Compared to postpartum women who drank alcohol but did not breastfeed, alcohol consumption during lactation is associated with development, specifically reduced abstract reasoning ability at 6 to 7 years in a dose-dependent fashion. These findings suggest a reevaluation of current breastfeeding guidelines.
There is no known lower limit of safety for alcohol exposure in pregnancy to avoid the common and most severe associated outcomes: fetal alcohol spectrum disorder (FASD) and stillbirth. Data on miscarriage vary and are not definitive. The term FASD describes the broad range of adverse sequelae in newborns and children, including alcohol-related birth defects (ARBDs), alcohol-related neurodevelopmental disorder (ARND), and fetal alcohol syndrome (FAS). ARBDs and ARND fall short of meeting all the criteria for the diagnosis of FAS, but they are terms that refer to offspring with structural or neurodevelopmental abnormalities in the setting of alcohol use. FAS is defined by maternal drinking during pregnancy, fetal growth problems at any point in time, facial dysmorphia (i.e., smooth philtrum, thin vermilion border, and small palpebral fissures), and central nervous system (CNS) abnormalities (i.e., structural abnormalities, neurologic problems, and low functional performance).
Fetal alcohol exposure can result in specific impairments of verbal learning, visual-spatial learning, attention, reaction time, and executive functions, which may be related to developmental abnormalities in the CNS. Functional magnetic resonance imaging (fMRI) identifies reduced overall brain size in persons with FAS. Although specific size reductions in the basal ganglia and cerebellum and an impaired or absent corpus callosum have been associated with fetal alcohol exposure, detailed autopsy data reveals more varied and less severe associations between prenatal alcohol exposure and brain abnormalities. The prevalence of FASDs is remarkably high when assessed via active surveillance. An active case ascertainment using physical examinations of first graders in the United States reported a weighted prevalence for FASDs from 31.1 to 98.5 per 1000 children. CDC reports a more conservative estimate: up to 1 in 20 US school children may have FASDs.
FASDs are considered to be completely preventable birth defects and neurodevelopmental abnormalities, and they are arguably the most common nongenetic cause of developmental delay. The risk of FASDs is not based solely on the timing or quantity of alcohol exposure, as twin studies confirm that identical prenatal exposure can lead to markedly different FASD outcomes. Given the heterogeneity of outcomes and continued uncertainties of mechanism, public health messaging continues to support alcohol abstinence in pregnancy.
Maternal alcohol consumption can have negative effects at any time during pregnancy. A prospective study of 992 subjects between 1978 and 2005 correlated the timing and pattern of alcohol exposure with the incidence of dysmorphia associated with FAS. Dysmorphia and growth disturbance were increased in women with first-trimester alcohol use. The risk was dose related without evidence of a threshold. Decreased birth length correlated with exposure in any trimester, and birth weight was more significantly affected by second-trimester exposure. A meta-analysis found no significant relationships between the frequency of LBW or SGA infants and alcohol intake up to approximately one drink per day or for preterm birth and alcohol intake up to 1.5 drinks per day, although LBW and SGA were associated with higher levels of alcohol consumption.
Prenatal exposure is associated with problems in childhood and adult life, including psychiatric illnesses, SUDs, poor social relations, inferior school performance, and legal issues. It is, however, difficult to separate the effect of in uterine exposure from the important contribution of the caregiving environment in child development. In fact, the quality of the caregiving environment and family function are associated with improved long-term outcomes of children with FASDs. Although the primary characteristics of FASDs are considered permanent, the severity of secondary characteristics (such as conduct disorders) are amenable to behavioral intervention. , Therefore, all infants prenatally exposed to alcohol should be referred for early intervention services.
Both screening and brief intervention are associated with a reduction in drinking in pregnancy. In a randomized controlled trial of 250 women with a positive alcohol screen, participants decreased their drinking by one-third to two-thirds when given an alcohol assessment tool with or without brief intervention by the care provider. Reduction in alcohol use by those with heavy use (defined as those having a positive screen on the T-ACE) was greater when a partner chosen by the patient was included in a brief intervention. People who screen positive for alcohol use need to be evaluated for alcohol use disorder (AUD), and those with AUD need treatment.
People with current alcohol use are at risk of withdrawal with abrupt cessation. Alcohol withdrawal, if untreated or undertreated, can be fatal and is considered a medical emergency. The severity of withdrawal increases with each withdrawal episode. More than 50% of people with AUD can experience alcohol withdrawal symptoms, and 3%–5% will exhibit symptoms of severe withdrawal including profound confusion, autonomic hyperactivity, seizures, and cardiovascular collapse (also known as delirium tremens). Delirium tremens (DT) occurs as early as 48 hours after abrupt cessation of alcohol and can last up to 7 days. Mortality has reduced greatly since the utilization of benzodiazepine treatment, though it still ranges from 1 to 4%. Alcohol treatment rests upon (1) assessment via CIWA-Ar (Clinical Institute for Withdrawal Assessment for Alcohol, Revised protocol), (2) benzodiazepine treatment, and (3) vitamin supplementation. All pregnant individuals with AUD need to be counseled and evaluated for the possibility of withdrawal and treated appropriately. The American Academy of Addiction Medicine recommends initial inpatient management for people at risk of severe withdrawal, including those with history of withdrawal seizures. For all pregnant individuals with AUD who require withdrawal management, inpatient treatment should be offered, particularly for those with moderate alcohol withdrawal (CIWA-Ar ≥10). Pregnancy is considered a medical condition that qualifies for inpatient management and this recommendation may be helpful for billing purposes. Most importantly, withdrawal management must be linked to continuing care. Withdrawal management (or detoxification) alone is not to be confused with addiction treatment and is associated with a nearly 5% subsequent yearly mortality rate. It is incumbent upon clinicians to ensure warm handoffs to ensure inpatient to outpatient continuity with providers knowledgeable about care for pregnant individuals.
There are several medications approved for the treatment of AUD (acamprosate, disulfiram, and naltrexone) and other medications that have been studied with established positive outcomes but for which FDA approval has not been sought (topiramate and gabapentin). None of these medications have been evaluated via randomized controlled trial in pregnancy. Medication recommendations for AUD in pregnancy rest upon the general literature of effectiveness as well as the recognition that both alcohol and untreated AUD are certainly more harmful than medications for AUD in pregnancy.
Disulfiram is an aldehyde dehydrogenase inhibitor that results in the unpleasant effects of accumulated acetaldehyde in the blood: sweating, headache, nausea, and vomiting. It is an aversive agent and therefore not grounded in the contemporary neuroscience of addiction. In practice, this medication has not been particularly effective, largely due to medication nonadherence, as suggested by a study of US veterans in which the results for disulfiram were similar to those for placebo. In pregnancy, there is limited data associating disulfiram with fetal malformations. ,
Naltrexone, a μ-opioid receptor antagonist, decreases heavy drinking to 84% of the placebo group and decreases heavy drinking days by 4%. It is available in both oral and long-acting injectable formulations but has not been studied for the treatment of AUD in pregnancy. There is currently a prospective trial evaluating naltrexone in both opioid use disorder and AUD.
Acamprosate’s mechanism of action is not completely established but is thought to be through modulation of glutamate neurotransmission. Acamprosate significantly reduces the risk of any drinking and increases the cumulative duration of abstinence across randomized controlled trials with a number needed to treat of 9–11. Animal data suggest possible teratogenicity, but there are limited human data.
Both gabapentin and topiramate have been studied for the treatment of AUD with results similar in terms of safety and efficacy to the three FDA-approved medications. , Neither have been specifically studied for the treatment of AUD in pregnancy. Gabapentin is not associated with major malformations but is associated with a higher risk of preterm birth, small for gestational age, and NICU admission. Systematic review data of antiepileptic medications in pregnancy demonstrates that topiramate may affect postnatal development but to a lesser extent than valproic acid and carbamazepine.
There is no reason to expect that the effectiveness of medication to treat AUD in general would be diminished in pregnancy. Although the limited data on safety may be concerning to some, when contrasted to the known risks of alcohol, consideration of medication for AUD should be standard in clinical care.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here