Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Skin provides an elastic, self-regenerating, protective covering for the body. The skin and its appendages are an important means by which we are viewed in the world and physical appearances are often critical to the well-being of patients. Examination of the skin, hair, and nails is performed as part of both the comprehensive and focused physical examination. The skin, hair, and nails can provide external visible clues to systemic disease that may not otherwise be apparent.
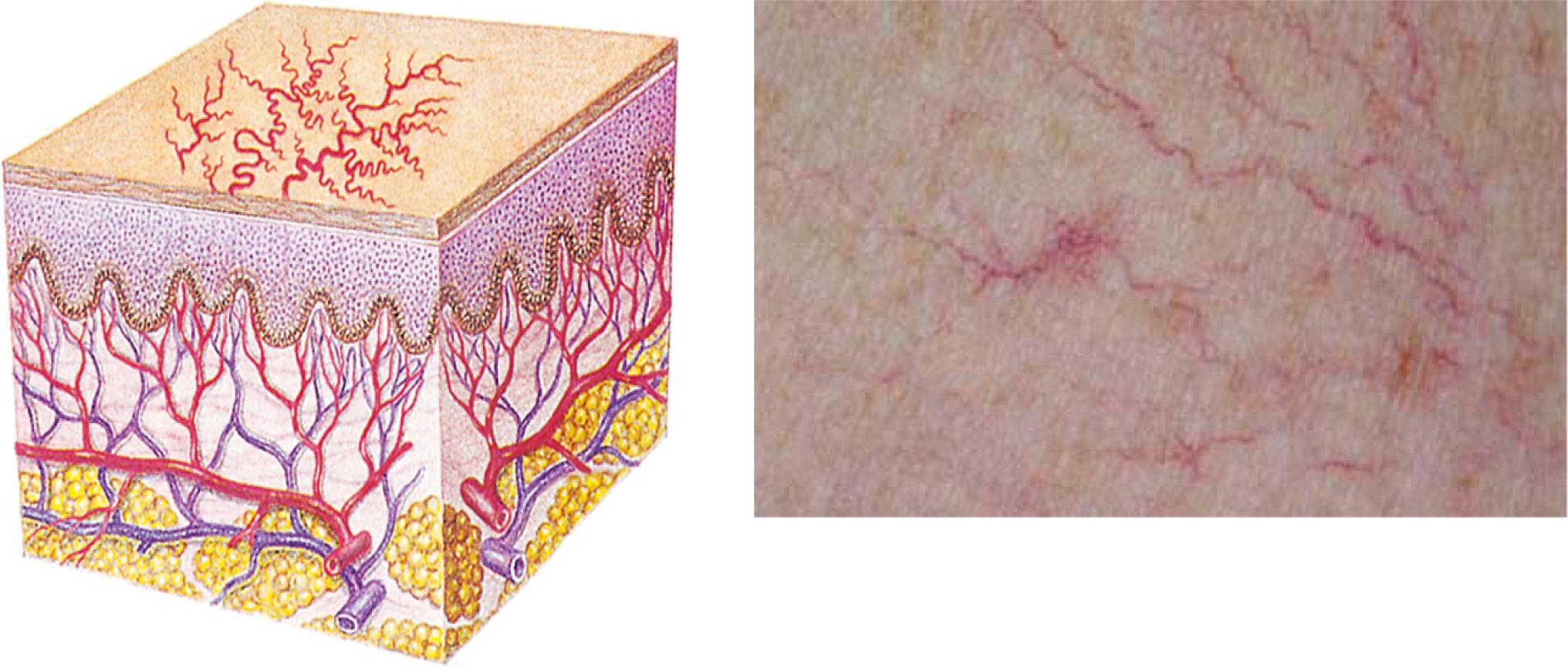
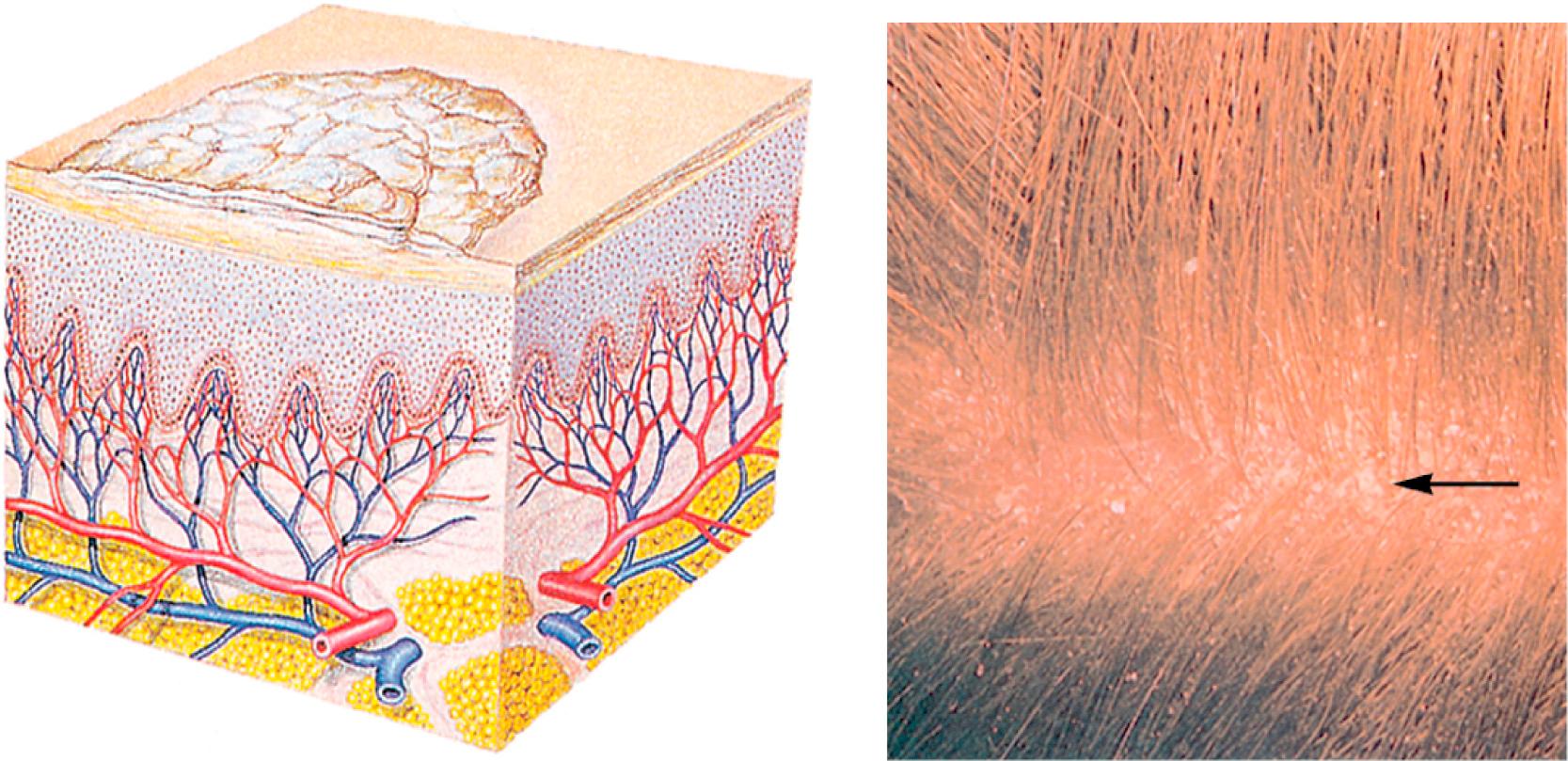
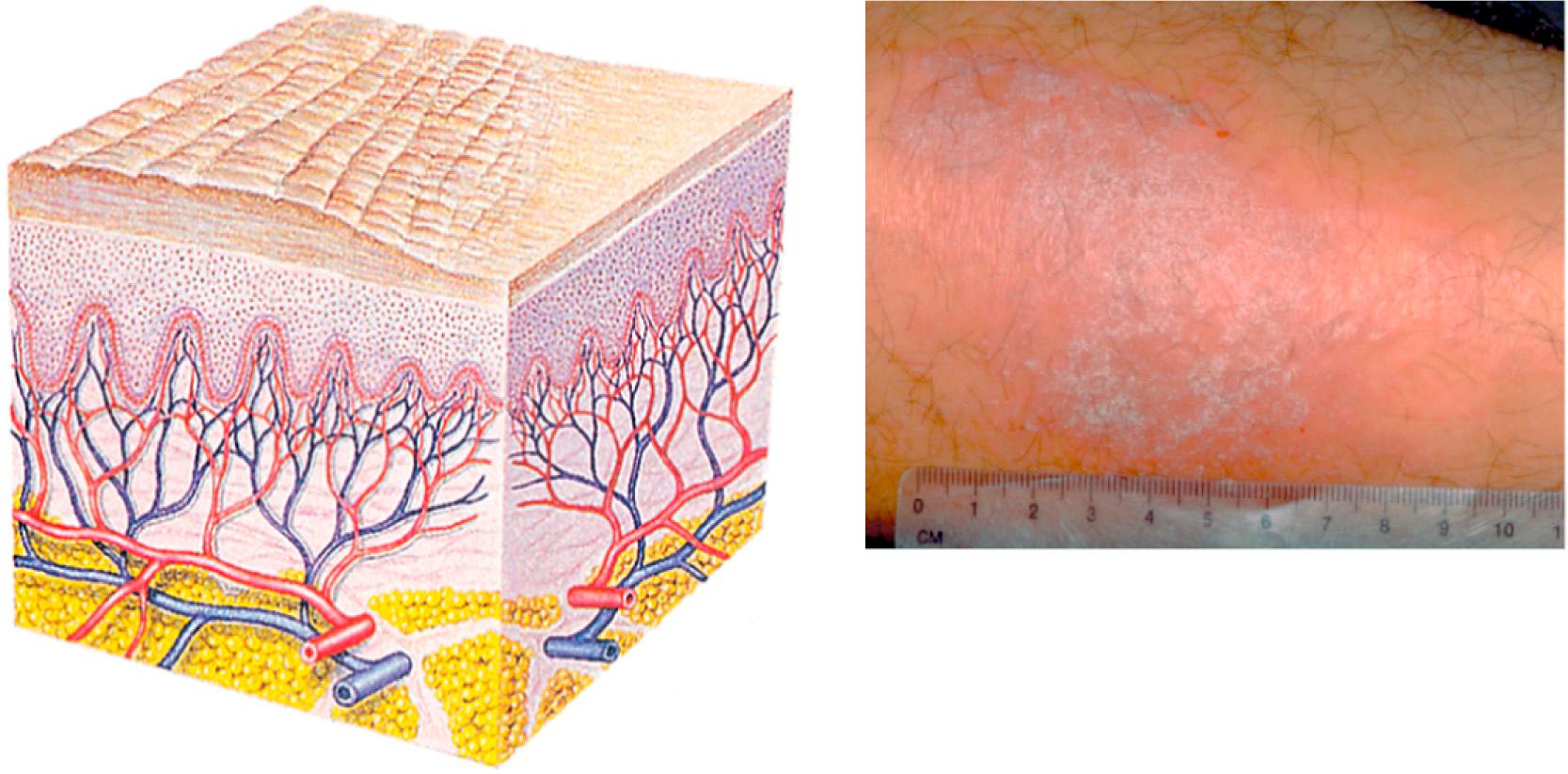
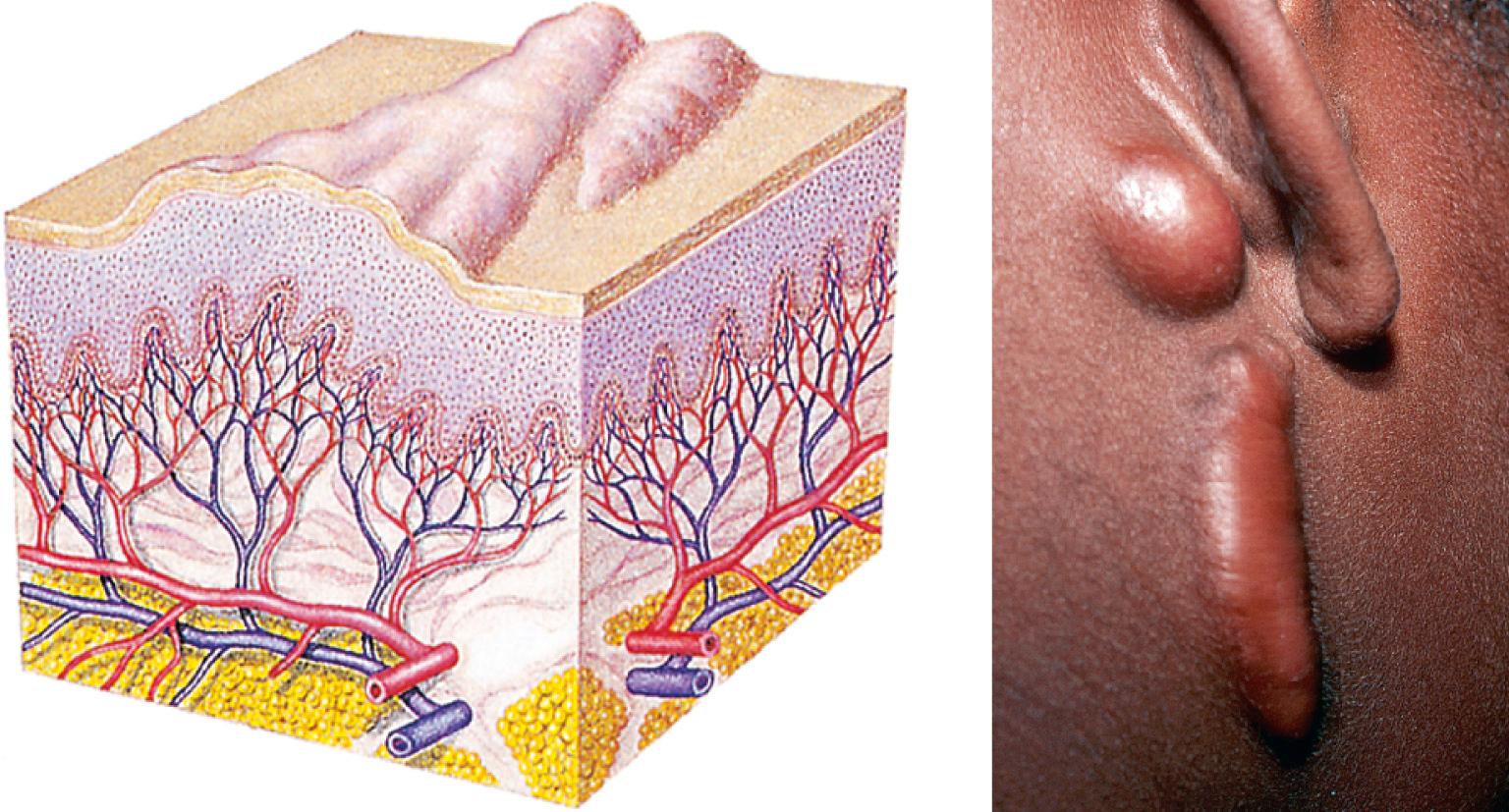
The skin is a stratified organ composed of several functionally related layers. Fig. 9.1 shows the main structural components and their approximate spatial relationships. It is important to note that the anatomy of the skin varies from one part of the body to another.

Skin structure and its physiologic processes perform the following integral functions:
Protect against microbial and foreign substance invasion and minor physical trauma
Restrict body fluid loss by providing a restrictive barrier
Regulate body temperature
Provide sensory perception via free nerve endings and specialized receptors
Produce vitamin D from precursors in the skin
Contribute to blood pressure regulation through constriction of skin blood vessels
Repair surface wounds by exaggerating the normal process of cell replacement
Excrete sweat, urea, and lactic acid
Express emotions
Systematically inspect the entire skin surface. During evaluation of each organ system, evaluate the overlying skin for:
Color
Uniformity
Thickness
Symmetry
Hygiene
Lesions
Odors
Palpate skin surfaces for:
Moisture
Temperature
Texture
Turgor (fullness or tension produced by the fluid content of the cells and tissue)
Elasticity
Inspect hair for:
Color
Distribution
Density
Palpate hair for texture and fragility
Inspect for:
Pigmentation of nail plates and nail beds
Length
Symmetry
Surface changes (ridging, beading, pitting, peeling)
Inspect and palpate proximal and lateral nail folds for:
Redness
Swelling
Pain
Exudate
Growths (warts, cysts, tumors)
Shape of lunulae
Palpate nail plate for:
Texture
Firmness
Thickness
Uniformity
Adherence to nail bed
Measure nail base angle
Observe the cuticles for:
Color
Vasculature
Integrity
The epidermis is the outermost portion of the skin and is composed of several cellular layers. The topmost layer is the stratum corneum (cornified layer), which is composed of closely packed, dead, keratin-filled squamous cells, and it is the chief mechanical barrier protecting the body against environmental exposures, pathogens, and restricting water loss. The keratins contained in the stratum corneum are synthesized in the lower layers of the skin, beginning at the stratum basale (basal layer). This lower layer contains stem cells, which allow for the regenerative properties of the skin to manifest. As keratinocytes mature, they pass from the basal layer through the granular layer to the cornified layer, a process that takes 28 days.
The thick skin of the palms and soles contains an additional layer compared with other parts of the body called the stratum lucidum, which lies just below the stratum corneum. Mucosal skin on the other hand, lacks a stratum corneum, allowing for diffusion through the skin surface. The stratum basale also contains melanocytes, the cells that synthesize melanin, which gives the skin its color.
The dermis is the richly vascular connective tissue layer of the skin that supports and separates the epidermis from adipose tissue. Interdigitating papillae secure the epidermis to the dermis and provide nourishment to the epidermal cells. Elastin, collagen, and reticular fibers provide resilience, strength, and stability. Sensory nerve fibers located in the dermis form a complex network that provides sensations of pain, touch, and temperature. The dermis also contains autonomic motor nerves that innervate blood vessels, glands, and the arrector pili muscles.
The dermis is connected to underlying tissues by the hypodermis, a subcutaneous layer that consists of loose connective tissue filled with adipose. This adipose layer generates heat and provides insulation, shock absorption, and a reserve of calories.
Cutaneous appendages are outgrowths of the skin and include eccrine sweat glands, apocrine sweat glands, sebaceous glands, hair, and nails.
The eccrine sweat glands open directly onto the surface of the skin and help regulate body temperature through sweat secretion. These glands are distributed throughout the body except at the lip margins, eardrums, nail beds, inner surface of the prepuce, and glans penis.
The apocrine glands are specialized structures found only in the axillae, nipples, areolae, anogenital area, eyelids, and external ears. Apocrine glands secrete an oily fluid containing protein, carbohydrate, and other substances. Secretions from these glands are odorless. Body odor is produced by bacterial decomposition of apocrine sweat.
The sebaceous glands secrete sebum, a lipid-rich substance that acts as a lubricant and moisturizer for skin and hair. Secretory activity, which is stimulated by sex hormones (primarily testosterone), varies according to hormonal levels throughout the life cycle.
A strand of hair consists of a root and a shaft which sit in a follicle. At the base of the follicle the papilla contains a loop of capillaries supplying nourishment for growth. Melanocytes in the follicle synthesize pigment, which gives hair its color. . Adults have both vellus and terminal hair. Vellus hair is short, fine, soft, and nonpigmented. Terminal hair is coarser, longer, thicker, and usually pigmented. Each hair goes through cyclic changes: anagen (growth), catagen (atrophy), and telogen (rest), after which the hair is shed (exogen). Males and females have about the same number of hair follicles with differential stimulation by hormones. The shape of the hair follicle directly relates to the shape of the hair itself (straight versus curly). This shape does vary by skin type.
The nails are appendages of the skin, which are composed of epidermal cells converted to hard plates of keratin. They protect the fingertips and are important in dexterity. The nail plate sits on the highly vascular nail bed which lies on periosteum. The white crescent-shaped area extending beyond the proximal nail fold marks the end of the nail matrix, the site of nail growth. The layer of skin covering the nail root is the cuticle, or eponychium, which pushes up and over the lower part of the nail body. The paronychium is the soft tissue surrounding the nail border ( Fig. 9.2 ).

 Infants and Children
Infants and ChildrenThe skin of infants and children is smoother than that of adults due to the absence of coarse terminal hair and diminished exposure to the elements, particularly ultraviolet (UV) radiation. Desquamation of the stratum corneum may be present at birth or shortly thereafter. It may vary from mild flakiness to course shedding of large sheets of skin, but post-term infants often have cracked, peeling skin. Vernix caseosa, a mixture of sebum and cornified epidermis, covers the infant’s body at birth. The subcutaneous fat layer is poorly developed in newborns, predisposing them to hypothermia. The newborn’s body, particularly the shoulders and back, can be covered with fine, silky hair called lanugo. More commonly seen in preterm infants, this hair is shed within 10 to 14 days. Some newborns are bald, whereas others have a large amount of head hair. Most of the hair is shed by about 2 to 3 months of age, to be replaced by more permanent hair with a new texture and often a different color.
The eccrine sweat glands begin to function after the first month of life, whereas apocrine function does not begin until puberty, thus children lack offensive perspiration.
AdolescentsDuring adolescence, the apocrine glands enlarge and become active, causing increased axillary sweating and sometimes body odor. Sebaceous glands increase sebum production in response to increased hormone levels, primarily androgen, giving the skin an oily appearance and predisposing the individual to acne.
Coarse terminal hair appears in the axillae and pubic areas of all adolescents and on the faces of adolescents assigned male at birth. Hair production is one response to changing androgen levels. (Refer to Chapter 8 . for a more thorough discussion of maturational changes during adolescence.)
Pregnant PatientsIncreased blood flow to the skin, especially to the hands and feet, results from peripheral vasodilation and increased numbers of capillaries. Acceleration of sweat and sebaceous gland activity occurs as well. Both processes assist in dissipating the excess heat caused by increased metabolism during pregnancy. Spider angiomas and cherry hemangiomas that are present may increase in size.
The skin thickens, and fat is deposited in the subdermal layers. Because of increased fragility of connective tissues, separation may occur with stretching. Most pregnant patients have some degree of increased pigmentation that is seen on the face, nipples, areolae, axillae, vulva, perianal skin, and umbilicus. During pregnancy, nevi may grow, change color, and new nevi may appear.
Older AdultsSebaceous and sweat gland activity decreases in older adults, and, as a result, the skin becomes drier with less perspiration produced. With aging and increased sun exposure, the epidermis thins and becomes more fragile, with decreased resistance to trauma. Epidermal permeability is increased, reducing the efficiency of the barrier function of the stratum corneum, causing skin to become dry.
Aging and sun exposure also contribute to decreasing elasticity and collagen loss in the dermis. The dermis shrinks, causing the epidermis to fold and become wrinkled. This effect is increased in lighter skin individuals, who have an earlier onset and greater skin wrinkling and sagging signs than darker skin types.
Subcutaneous tissues also decrease, particularly in the extremities, giving joints and bony prominences a sharp, angular appearance. The hollows in the thoracic, axillary, and supraclavicular regions deepen as well.
Gray hair results from a decrease in the number of functioning melanocytes. Axillary and pubic hair production declines because of a reduction in hormones. The density and rate of scalp hair growth (anagen phase) decline with age. The size of hair follicles also changes, and terminal scalp hair progressively transitions into vellus hair, causing age-associated baldness in both men and women. The opposite transition, from vellus to terminal, occurs in the hair of the nares and on the tragus of men’s ears. Both genders experience overall loss of hair from the trunk and extremities. Peripheral extremity hair loss may also occur when peripheral vascular disease is present.
Nail growth slows and nails become more brittle because of decreased peripheral circulation. The nails, particularly the toenails, become thick, brittle, hard, and yellowish. They develop longitudinal ridges and are prone to splitting into layers.
For each of the symptoms or conditions discussed in this section, targeted topics to include in the history of the present illness are listed. Responses to questions about these topics provide clues to focus the physical examination and develop an appropriate diagnostic evaluation. Questions regarding medication use (prescription and over the counter preparations) as well as complementary and alternative therapies are relevant for each.
Changes in skin: dryness, pruritus, sores, rashes, growths, color, texture, odor, amount of perspiration; changes in wart or nevus; lesion that does not heal or is chronically irritated (see Risk Factors boxes)
Temporal sequence: date of initial onset; time sequence of occurrence and development; intermittent; sudden or gradual onset; date of recurrence, if any
Symptoms: itching, pain, exudate, bleeding, color changes, seasonal or climate variations
Location: skinfolds, extensor or flexor surfaces, localized or generalized, sun exposed or protected, mucosal involvement
Associated symptoms: recent illness, presence of systemic disease or fever, relationship to stress or leisure activities
Recent exposure to environmental or occupational toxins or chemicals, new skin or personal care products, new household cleaning products (aerosols)
Recent exposure to persons with similar skin condition
Apparent cause of problem, patient’s perception of cause
Travel history: where, when, length of stay, exposure to diseases, contact with travelers
What the patient has been doing for the problem, response to treatment, what makes the condition worse or better
How the patient is adjusting to the problem
Medications: antibiotics, any new medications; either over-the-counter or prescription, topical preparations to treat—steroids, antifungals
Exposure to sunlight or ultraviolet radiation (UVA and UVB) including
Severe blistering sunburns, even as a child
Indoor tanning device usage
Geographic exposure (people who live in areas that get large amounts of UV radiation from the sun, e.g., higher altitude)
Previous personal history of melanoma
Family history of melanoma (first-degree relative)
Atypical nevi
Large congenital nevus (>15 cm)
Immune suppression
Skin type, relative inability to tan (Skin types, Box 9.1 )
People burn or tan depending on their skin type, the time of year, and how long they are exposed to ultraviolet (UV) rays. The six types of skin, based on how likely it is to tan or burn, are as follows:
I: Always burns, never tans, sensitive to UV exposure
II: Burns easily, tans minimally
III: Burns moderately, tans gradually to light brown
IV: Burns minimally, always tans well to moderately brown
V: Rarely burns, tans profusely to dark
VI: Never burns, deeply pigmented, least sensitive
Although everyone’s skin can be damaged by UV exposure, people with skin types I and II are at the highest risk.
Age (older than 50 years)
Exposure to sunlight or ultraviolet radiation (UVA and UVB)
Indoor tanning device usage
Blistering sunburns
Chronic and cumulative exposure—squamous cell carcinoma
Intermittent exposure—basal cell carcinoma
Geographic location: near equator or at high altitudes
Skin type, relative inability to tan (see Skin Type, Box 9.1 )
Exposure to arsenic, creosote, coal tar, and/or petroleum products
Overexposure to radium, radioisotopes, or x-rays
Repeated trauma or irritation to skin
Precancerous dermatoses
Large scars
Changes in hair: loss or growth, distribution, texture, color
Occurrence: sudden or gradual onset, symmetric or asymmetric pattern, recurrence
Associated symptoms: pain, itching, lesions, presence of systemic disease or high fever, recent stress, hair-pulling, infection
Exposure to drugs, environmental or occupational toxins or chemicals, commercial hair care chemicals
Nutrition: dietary changes, dieting
What the patient has been doing for the problem, response to treatment, what makes the problem worse or better
How the patient is adjusting to the problem
Medications: drugs or preparations for hair loss (minoxidil, finasteride, dihydrotestosterone [DHT] inhibitors)
Changes in nails: splitting, breaking, discoloration, ridging, thickening, markings, separation from nail bed
Recent history: systemic illness, high fever, trauma, stress, biting
Associated symptoms: pain, swelling, exudate
Temporal sequence: sudden or gradual onset, relationship to injury of nail or finger
Recent exposure to drugs, environmental or occupational toxins or chemicals; frequent immersion in water
What the patient has been doing for the problem, response to treatment, what makes the problem worse or better
Medications: chemotherapy (taxanes, anthracyclines), psoralens, retinoids, tetracyclines, antimalarials
Previous skin problems: sensitivities, allergic skin reactions, skin disorders (e.g., atopic dermatitis), congenital or acquired lesions, treatment
Tolerance to sunlight ( Box 9.1 )
Diminished or heightened sensitivity to touch
Cardiac, respiratory, liver, endocrine, or other systemic diseases
Hair
Previous hair problems: loss, thinning, unusual growth or distribution, brittleness, breakage, treatment
Systemic problems: thyroid disorder, rheumatologic disease, any severe illness, malnutrition, associated skin disorder
Previous nail problems: injury; bacterial, fungal, or viral infection
Systemic problems: associated skin disorder; congenital anomalies; respiratory, cardiac, endocrine, hematologic, or other systemic disease
Current or past dermatologic diseases or disorders in family members; melanoma and other skin cancers; dermatoses (e.g., psoriasis); infestations; bacterial, fungal, or viral infections
Allergic hereditary diseases such as asthma or allergic rhinitis
Autoimmune disorders such as systemic lupus erythematosus
Familial hair loss or pigmentation patterns
Skin care habits: cleansing routine; soaps, oils, emollients, or local applications used; cosmetics; home remedies or preparations used; sun exposure patterns and history; sunburn history; use of sunscreen agents; recent changes in skin care habits (see Patient Safety, “Sunscreen”)
Skin self-examination ( Box 9.2 )
Always use a good light, positioned to minimize distracting glare. Look for a new growth or any skin change.
Be aware of the locations and appearance of nevi and birthmarks.
Examine your back and other hard-to-see areas of the body using full-length and handheld mirrors. Ask a friend or relative to help inspect those areas that are difficult to see, such as the scalp and back.
Begin with your face and scalp using one or more mirrors. Proceed downward, focusing on neck, chest, and torso. Patients, check under breasts. With back to the mirror, use hand mirror to inspect back of neck, shoulders, upper arms, back, buttocks, legs. Concentrate especially on areas where atypical nevi (those with unexpected changes) are most common—the shoulders and back; and areas where ordinary nevi are rarely found—the scalp, breast, and buttocks. Check hands, including nails. In a full-length mirror, examine elbows, arms, underarms. Sitting down, check legs and feet, including soles, heels, nails, and between the toes. Use a hand mirror to examine genitals. See as well as feel any early signs of a nevus change. Use a cell phone to take photos of nevi and compare the photographs of the same nevi over a period of several months. Monitor change in size by measuring. It can be done simply with a small ruler or even by comparing the nevi to the size of your thumb or fingernail.
Consult your healthcare provider promptly if any pigmented skin spots look like melanoma, if new nevi have appeared, or if any existing nevi have changed. See also the ABCDE changes in nevi (Melanoma, in Abnormalities).
Hair care habits: cleansing routine, shampoos and oils and moisturizers, coloring preparations used, permanents, applied heat, hair straightening, extensions, recent changes in hair care habits. Note that hair care practices can vary by hair type.
Nail care habits: any difficulty in clipping or trimming nails, instruments used; biting nails; use of artificial nail overlays
Exposure to environmental or occupational hazards: dyes, chemicals, plants, toxic substances, frequent immersion of hands in water, frequent sun exposure, hand sanitizers
Recent psychological or physiologic stress
Use of alcohol, tobacco
Sexual history: sexually transmitted infections (syphilis, gonorrhea, human immunodeficiency virus [HIV])
Use of illicit drugs
Do you ask if your patients use sunscreen? Keep this in mind when they respond: Skin should be the same color all year long. Those who use sunscreen with a protection factor of 30 or higher are still at risk for significant sunburn. Why? People often don’t use enough sunscreen. They think they are protected, but they are in fact getting significant UV exposure. It is necessary to apply sunscreen generously (about 1 shot glass full over entire body) and frequently. Apply minutes before exposure and then reapply after swimming or bathing and every 2–3 hours of sun exposure.
Other recommendations include:
Do not sunbathe.
Avoid unnecessary sun exposure, especially between 10:00 am and 4:00 pm , the peak hours for harmful UV radiation; seek shade if you must be outdoors during these hours.
When exposed to sunlight, wear protective clothing such as long pants, long-sleeved shirts, broad-brimmed hats, and UV-protective sunglasses. Look for SPF-containing clothing, which offers the benefit of not needing reapplication.
Never use tanning booths.
Teach children good sun protection habits at an early age: the damage that leads to adult skin cancers starts in childhood.
Infants
Birth history: term or premature
Feeding history: breast or formula, type of formula, what foods introduced and when (see Clinical Pearl, “Carotenemia”)
Diaper history: type of diapers used, skin cleansing routines, and methods of cleaning
Types of clothing and washing practices: soaps and detergents used, new blanket or clothing
Bathing practices: frequency, types of soap, oils, shampoos or emollients used
Dress habits: amount and type of clothing in relation to environmental temperature
Temperature and humidity of the home environment: air conditioning, heating system (drying or humidified)
Carotenemia, or xanthoderma, common in infants who have started eating baby foods, is characterized by yellow pigmentation of the skin and increased beta-carotene levels in the blood. Carotenemia does not cause orange discoloration of the sclerae, and is thus typically easy to distinguish from jaundice. In most cases, it is a benign condition which follows increased consumption of carotene-rich foods, such as carrots, squash, and sweet potatoes. If parental anxiety is high, provide reassurance and counsel that after discontinuation of carotene-rich foods, the skin color will normalize in weeks or months.
Children and Adolescents
Eating habits and types of food
Food allergies. Some children with eczema have worsening with specific foods.
Exposure to infectious diseases in childcare settings, school: impetigo; viruses that produce skin rashes (Coxsackie); measles, mumps, rubella, varicella in unvaccinated children, sexual activity
Allergic disorders: eczema, urticaria, pruritus, allergic rhinitis, asthma, other chronic respiratory disorders
Pets or animal exposure
Activities: sports, use of musical instruments
Outdoor exposures such as hiking, camping, picnics, gardening
Skin injury history: frequency of falls, cuts, abrasions; repeated history of unexplained injuries
Chronic hair-pulling or manipulation
Nail-biting
Pregnant Patients
Weeks of gestation or postpartum
Prior pregnancies
Hygiene practices
Presence of skin problems before pregnancy (e.g., acne may worsen)
Effects of pregnancy on preexisting conditions (e.g., autoimmune disorders may remit; condylomata acuminata commonly become larger and more numerous)
Older Adults
Increased or decreased sensation to touch or to the environment
Generalized chronic itching; exposure to skin irritants, detergents, lotions (any moisturizer that comes in a pump has a high alcohol content), woolen clothing, humidity of environment
Susceptibility to skin infections
Healing response: delayed or interrupted
Frequent falls resulting in multiple cuts or bruises
Risk for pressure ulcers secondary to immobilization or non-ambulatory status
History of chronic medical conditions (e.g., diabetes mellitus, vascular disease)
Medications and polypharmacy
Centimeter ruler (flexible, clear)
Flashlight or penlight
Handheld magnifying lens or dermatoscope
Wood’s lamp (to view fluorescing or depigmented lesions)
Use inspection and palpation to examine the skin, and remember, the most important tools you have are your own eyes and powers of observation. When gross inspection leaves you uncertain, sometimes a handheld magnifying glass or dermatoscope will help.
Adequate lighting is essential. Direct, overhead lighting should be used when examining patients. Tangential lighting is helpful in assessing contour. Inadequate lighting can result in inadequate assessment.
Although the skin is commonly observed as each part of the body is examined, it is important to make a brief but careful overall visual sweep of the entire body. This “bird’s-eye view” gives a good idea of the distribution, extent, and symmetry of any lesions. It also allows for identification of “ugly duckling” lesions that stand out. The gross view will allow the practitioner to know where to pay particular attention during the remainder of the examination ( Box 9.3 ).
The use of certain traditional health practices by various cultural groups can produce cutaneous manifestations that could be wrongly confused with disease or physical abuse. Two such practices are “coining” and “cupping” as used by some Asian subcultures. In coining, a coin dipped in mentholated oil is vigorously rubbed across the skin in a prescribed manner, causing a mild dermabrasion. This practice is believed to release excess force from the body and hence restore balance. In cupping, a series of small, heated glasses are placed on the skin, forming a suction that leaves a red or purpuric circular mark, drawing out the bad force. The skin markings may alarm the healthcare provider who is unaware of such practices. The lesson: in the history, ask about home remedies or practices.

Adequate exposure of the skin is also necessary. It is essential to remove clothing and to fully remove drapes or coverings as each section of the body is examined, while keeping in mind the patient’s sense of privacy. Make sure that the room temperature is comfortable. Look carefully at all areas, remembering to inspect areas that are usually not exposed, such as the axillae, buttocks, perineum, backs of thighs, and inner upper thighs. Remove shoes and socks to look at the feet, and pay careful attention to intertriginous surfaces (areas where two skin surfaces may touch, e.g., axillae and groin), especially in infants, older adults, and bedridden patients. As you complete the examination for each area, re-drape or cover the patient. When inspecting the skin, it is important to have a systematic routine in place to ensure that no areas are forgotten or overlooked. Skin thickness varies over the body, with the thinnest skin being on the eyelids and the thickest present in areas subject to increased pressure or rubbing; most notably the soles, palms, and elbows. Make note of calluses on the hands or feet and look for corns on pressure points. Corns are flat or slightly elevated with a central core, circumscribed, painful lesions with a smooth, hard surface ( Fig. 9.3 ). A superficial area of hyperkeratosis is called a callus. Calluses usually occur on the weight-bearing areas of the feet and on the palmar surface of the hands. Calluses are not as well demarcated as corns and are usually not as tender, if at all ( Fig. 9.4 ).


The range of expected skin color varies from dark brown to white with pink or yellow overtones. Although color should assume an overall uniformity, there is often pigment variation that may be sun related, trauma induced, or simply normal (e.g., knuckles may be darker in dark-skinned patients). Callused areas may appear yellow. Vascular flush areas (e.g., cheeks, neck, upper chest, and genital area) may appear pink or red, especially with anxiety or excitement. Be aware that skin color may be masked by cosmetics and tanning agents. Look for localized areas of discoloration.
Individuals with dark skin may show pigmentary demarcation lines. These lines, a normal variation, mark the border between deeply pigmented skin and lighter pigmented skin. They are most commonly seen on the arms, legs, chest, and back and have been reported most often in Black and Japanese populations. Accentuation of preexisting lines or appearance of new lines may occur during pregnancy.
Nevi (moles) occur in forms that vary in size and degree of pigmentation. Nevi are present on most persons regardless of skin color and may occur anywhere on the body. They may be flat, raised, dome-shaped, smooth, rough, or hairy. Their color ranges from pink, tan, gray, blue, and shades of brown, to black. Table 9.1 describes the features and occurrence of various types of pigmented nevi.
| Type | Features | Occurrence | Comments |
|---|---|---|---|
| Halo nevus | Sharp, oval, or circular; depigmented halo around nevus; may undergo many morphologic changes; usually disappears and halo repigments (may take years) | Usually on back in young adult | Usually benign; biopsy indicated because same process can occur around melanoma |
| Intradermal nevus | Dome-shaped; raised; flesh to black color; may be pedunculated or hair bearing | Cells limited to dermis | No indication for removal other than cosmetic |
| Junction nevus | Flat or slightly elevated; dark brown | Nevus cells lining dermoepidermal junction | Should be removed if exposed to repeated trauma |
| Compound nevus | Slightly elevated brownish papule; indistinct border | Nevus cells in dermis and lining dermoepidermal junction | Should be removed if exposed to repeated trauma |
| Congenital nevus | May be present at birth; may cover large area; hair growth may occur after several years | Should be removed if changes occur | |
| Blue nevus | Blue to blue/gray in color | Nevus cells in dermis | Typically benign, but should be removed if changes occur |
Nevi occur more often in lighter-skinned than in darker-skinned individuals. There is a strong association between sun exposure and the number of nevi. They increase in number throughout infancy and childhood, with peak incidence in the fourth to fifth decades. Nevi frequently involute and diminish in number with advancing age and rarely develop after 40 years of age.
Although most nevi are harmless, some may be atypical or develop into melanoma. Table 9.2 describes differences in the features of normal and atypical nevi. Atypical nevi tend to occur on heavily sun damaged skin, classically upper back in men and on the legs in women ( Box 9.4 “Atypical Nevi or Melanoma?”).
| Feature | Normal Nevus | Atypical Nevus |
|---|---|---|
| Color | Uniformly tan or brown; all nevi on one person tend to look alike | Mixture of tan, brown, black, and red/pink; nevi on one person often do not look alike |
| Shape | Round or oval with a clearly defined border that separates the nevus from surrounding skin | Irregular borders may include notches; may fade into surrounding skin and include a flat portion level with skin |
| Surface | Begins as flat, smooth spot on skin; becomes raised; forms a smooth bump | May be smooth, slightly scaly, or have a rough, irregular, “pebbly” appearance |
| Size | Usually less than 6 mm (size of a pencil eraser) | Often larger than 6 mm and sometimes larger than 10 mm |
| Number | Typical adult has 10–40 nevi scattered over the body | Many persons do not have increased number; however, persons severely affected may have more than 100 nevi |
| Location | Usually above the waist on sun-exposed surfaces of the body; scalp, breast, and buttocks rarely have normal nevi | May occur anywhere on the body, but most commonly on back; may also appear below the waist and on scalp, breast, and buttocks |
Atypical nevi occur predominantly on the trunk. They tend to be large, usually greater than 5 mm, with a flat component. The border is typically ill defined. The shape can be round, oval, or irregular. The color is usually brown but can be mottled with dark brown, pink, and tan. Some individuals have only 1–5 nevi; others have more than 100.
In melanoma, the border is more irregular. Lesions tend to be larger, often greater than 6 mm. Color variation within the lesion is characteristic, ranging from tan-brown, dark brown, or black to pink, red, gray, blue, or white. Any lesion suggestive of a melanoma must be biopsied.
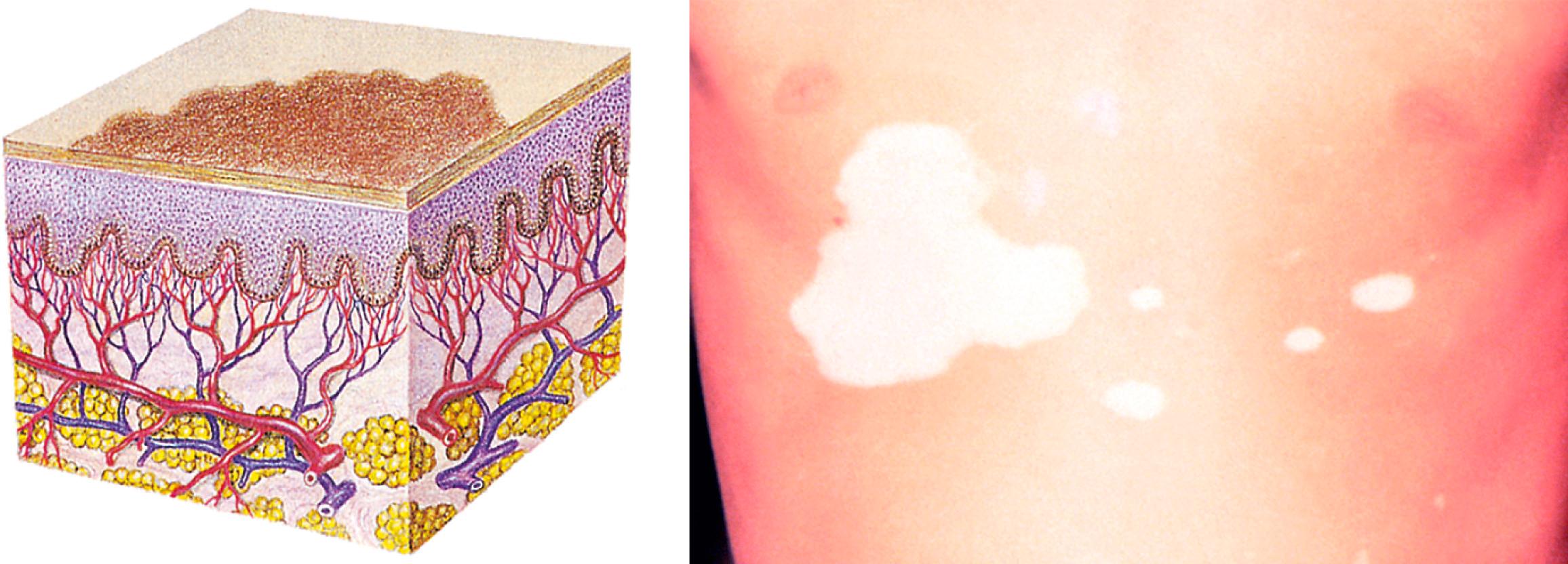
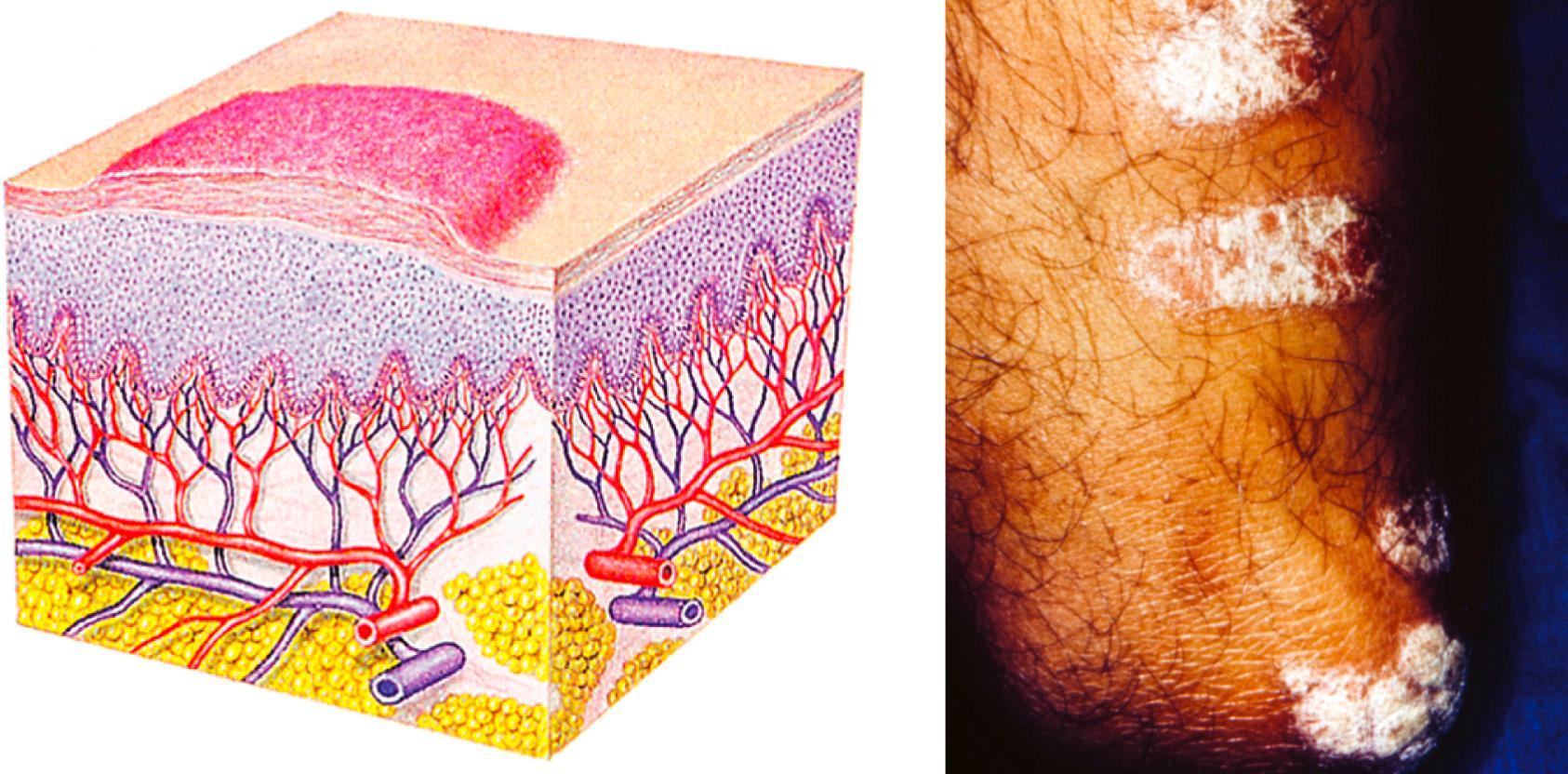
Several variations in skin color occur in almost all healthy adults and children, including nonpigmented striae (i.e., silver or pink “stretch marks” that occur during pregnancy, adolescent growth spurts, or weight gain), freckles in sun-exposed areas, birthmarks, and nevi ( Fig. 9.5 ). Adult women (and sometimes men) will commonly have melasma ( Fig. 9.6 ), areas of hyperpigmentation on the face and neck that are associated with pregnancy or hormonal variation. This condition is more noticeable in darker-skinned patients. The absence of melanin produces patches of unpigmented skin or hair, such as with vitiligo ( Fig. 9.7 ).

.")

Alterations in color in dark-skinned persons are best seen in the sclera, conjunctiva, buccal mucosa, tongue, lips, nail beds, and palms. Particular variations in skin color may be the result of physiologic pigment distribution. The palms and soles are lighter in color than the rest of the body and should be assessed when concerned for diffuse skin changes such as erythroderma, which is an intense, widespread reddening of the skin. Hyperpigmented lentigos on the palms and soles of the feet are common in darker skinned patients. These are small pigmented spots on the skin with a clearly demarcated edge that is surrounded by normal-appearing skin. It is a harmless (benign) hyperplasia of melanocytes. Freckling of the buccal cavity, gums, and tongue commonly occurs and is benign. The sclera may appear yellowish brown (often described as “muddy”) or may contain brownish pigment that resemble nevi. A bluish hue of the lips and gums can be a normal finding in persons with dark skin. Some dark-skinned persons have very blue lips, giving a false impression of cyanosis.
Systemic disorders can produce generalized or localized color changes; these are described in Table 9.3 . Localized redness often results from an inflammatory process. Pale, shiny skin of the lower extremities may reflect peripheral changes that occur with systemic diseases such as diabetes mellitus and peripheral vascular disease. Injury, steroids, vasculitis, stasis, and several systemic disorders can cause localized hemorrhage into the skin, producing red-purple discolorations. Bleeding into the skin results in ecchymoses (i.e., bruising); pinpoint bleeding from capillaries is called petechiae (smaller than 0.5 cm in diameter) ( Fig. 9.8 ) or purpura (larger than 0.5 cm in diameter) ( Fig. 9.9 ). Vascular skin lesions are characterized in Fig. 9.10 (see Clinical Pearl, “Telangiectasias: Spider Angioma”). Box 9.5 describes some characteristic odors that you may note as you examine the skin.
Telangiectasias are small, permanently dilated blood vessels consisting of venules or arterioles. Spider angiomas are arterial. Blanch the center, and they will refill in an organized way from the center out and evenly in all directions (see Fig. 9.10 ).
| Color | Cause | Distribution | Select Conditions |
|---|---|---|---|
| Brown | Darkening of melanin pigment | Generalized | Pituitary, adrenal, liver disease |
| Localized | Nevi, neurofibromatosis | ||
| White | Absence of melanin | Generalized | Albinism |
| Localized | Vitiligo | ||
| Red (erythema) | Increased cutaneous blood flow | Localized | Inflammation |
| Generalized | Fever, viral exanthem, urticaria | ||
| Increased intravascular red blood cells | Generalized | Polycythemia | |
| Yellow | Increased bile pigmentation (jaundice) | Generalized | Liver disease |
| Increased carotene pigmentation | Generalized (except sclera) | Hypothyroidism, increased intake of vegetables containing carotene | |
| Blue | Increased unsaturated hemoglobin secondary to hypoxia | Lips, mouth, nail beds | Cardiovascular and pulmonary diseases |
| Violaceous | Damage to blood vessels or extravasation of blood into skin | Localized | Vasculitis, Vasculopathy, Bruising |



Even the skin may have odors suggesting a variety of problems; infectious, metabolic, or neurologic. Sweatiness intensifies the odor.
| CAUSE OF ODOR | TYPE OF ODOR |
|---|---|
| Clostridium gas gangrene | Rotten apples |
| Proteus infection | Mousy |
| Pseudomonas infection (especially burns) | Grapelike |
| Tuberculous lymphadenitis (scrofula) | Stale beer |
| Anaerobic infection; scurvy | Putrid |
| Intestinal obstruction, peritonitis | Feculent |
| Phenylketonuria | Mousy, musty |
As you inspect, palpate the skin for moisture, temperature, texture, turgor, and elasticity. Palpation may yield additional data for describing lesions, particularly in relation to elevation or depression.
Minimal perspiration or oiliness should be present. Increased perspiration may be associated with activity, a warm environment, obesity, anxiety, or excitement; it may be especially noticeable on the palms, scalp, forehead, and in the axillae. The intertriginous areas, or skin in body folds, may also be damp leading to development of intertrigo ( Fig. 9.11 ).

The skin should range in temperature from cool to warm-to-the-touch. Use the dorsal surface of your hands or fingers in this case because these areas are most sensitive to temperature perception. At best, this assessment is a rough estimate of skin temperature; what you are really looking for is bilateral symmetry. Environmental conditions, including the temperature of the examining room, as well as body location may affect surface temperature.
The texture should feel smooth, soft, and even. Roughness on exposed areas or areas of pressure (particularly the elbows, soles, and palms) may be caused by dry skin or irritation. Extensive or widespread roughness may be the result of a keratinization disorder or damaged skin. Hyperkeratosis, especially of the palms and soles, may be a sign of a systemic disorder such as exposure to arsenic, other toxins, or a sign of internal malignancy.
Assessment of skin elasticity can be helpful in detecting certain conditions. Gently pinch a small section of skin on the forearm or sternal area between the thumb and forefinger and then release the skin ( Fig. 9.12 ). The skin should move easily when pinched and return to place immediately when released. Poor skin turgor can indicate severe dehydration. In this case, the skin is very slow to return to normal and “tents” up. This may occur with excessive vomiting, diarrhea, or dehydration from another cause. Skin that is firm or cannot be pinched may suggest an underlying connective tissue disease such as scleroderma.

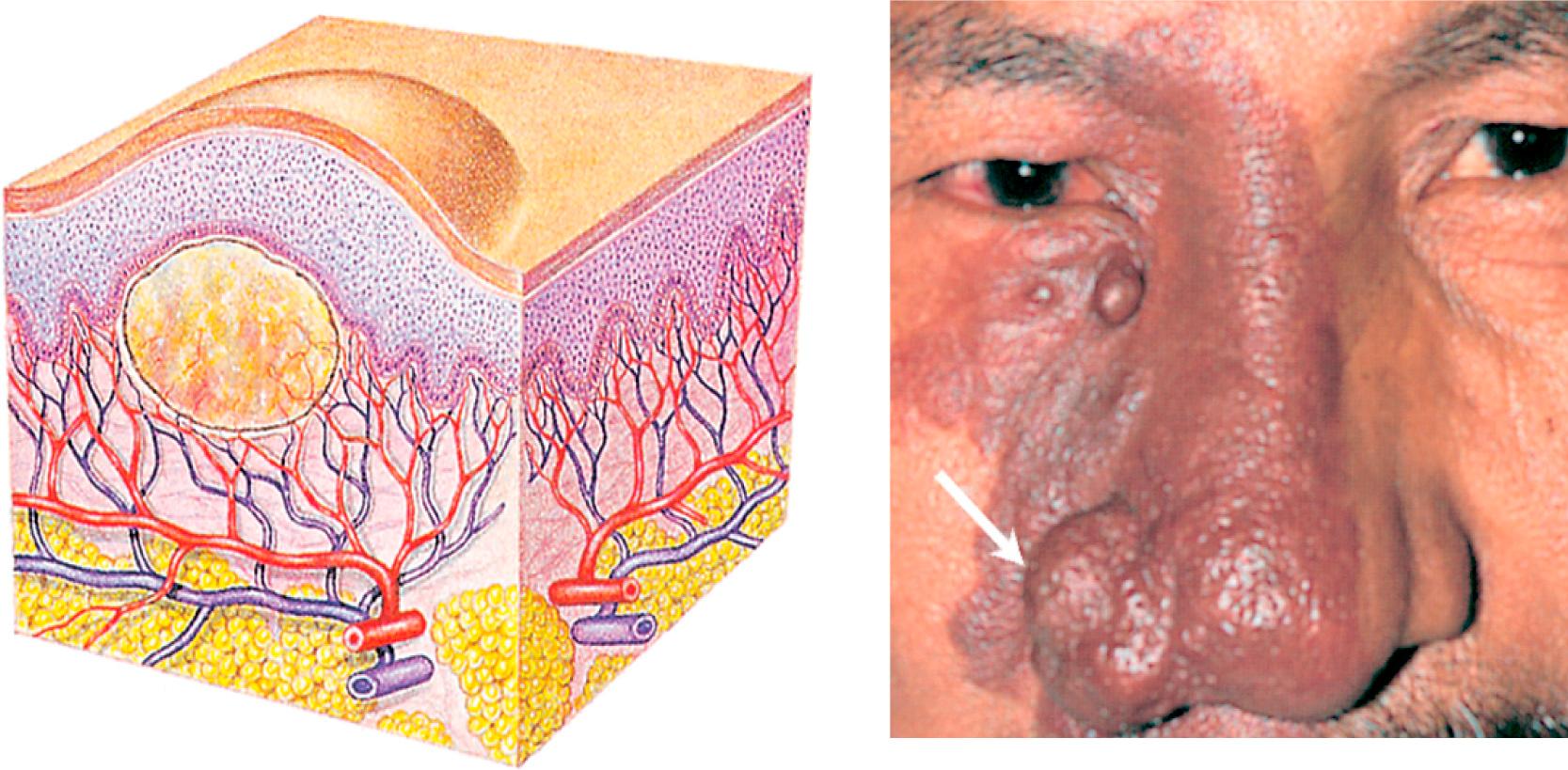
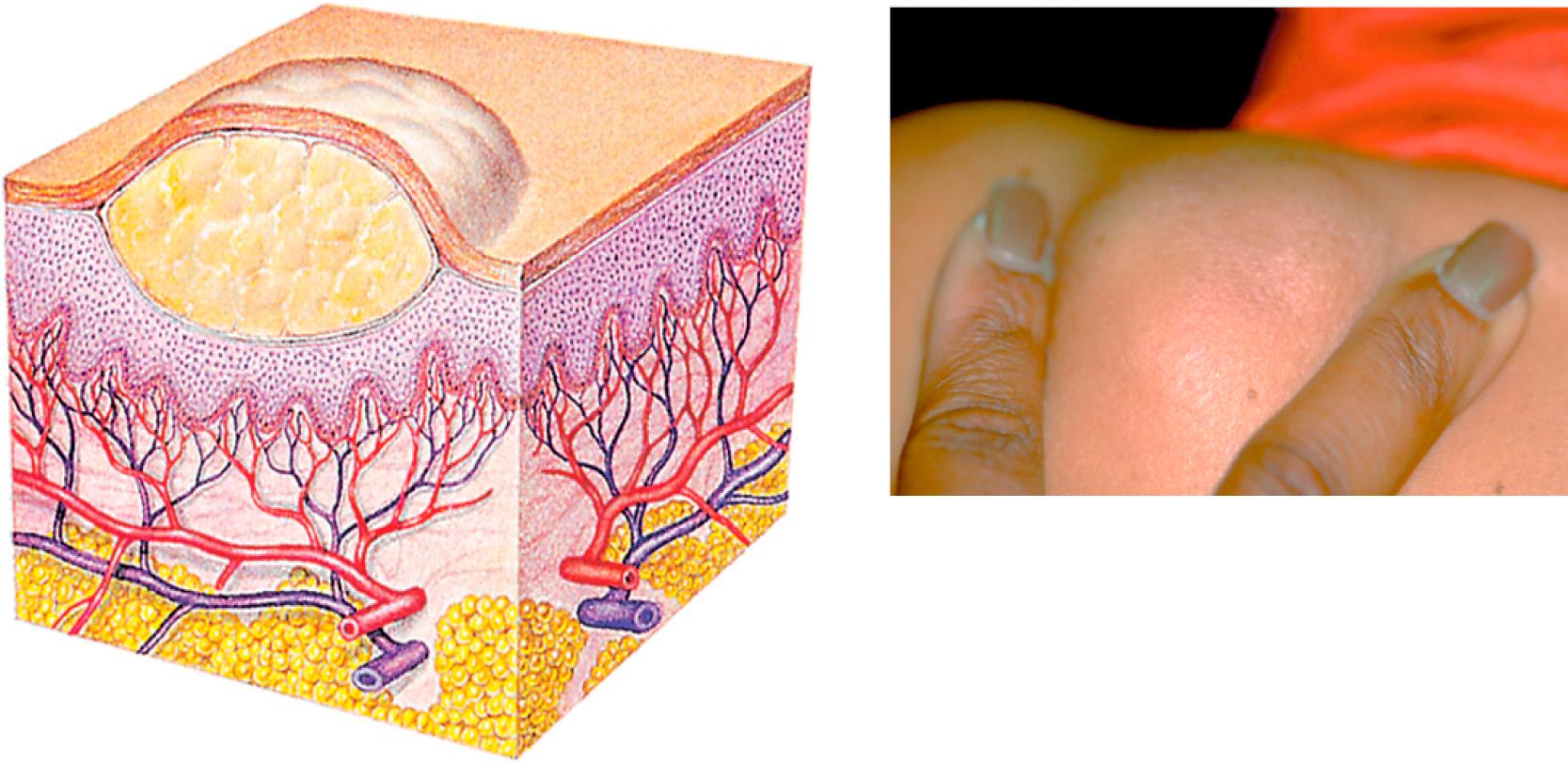
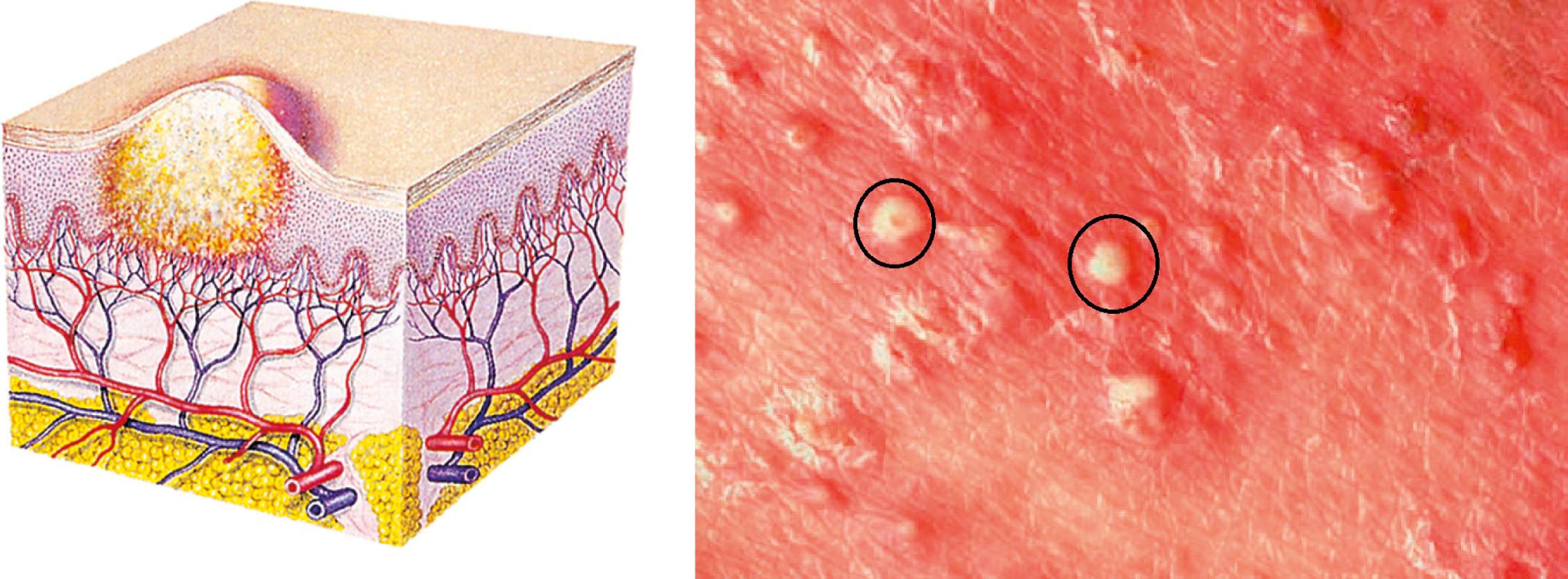
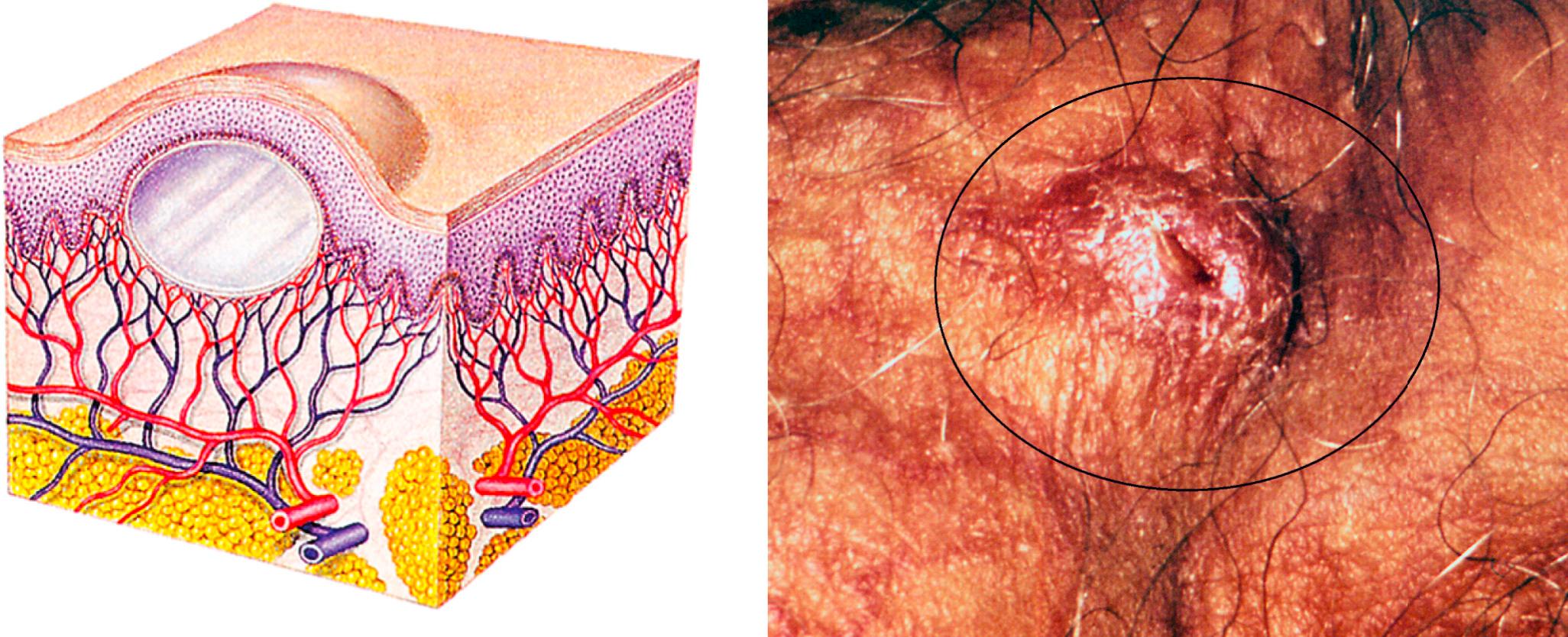
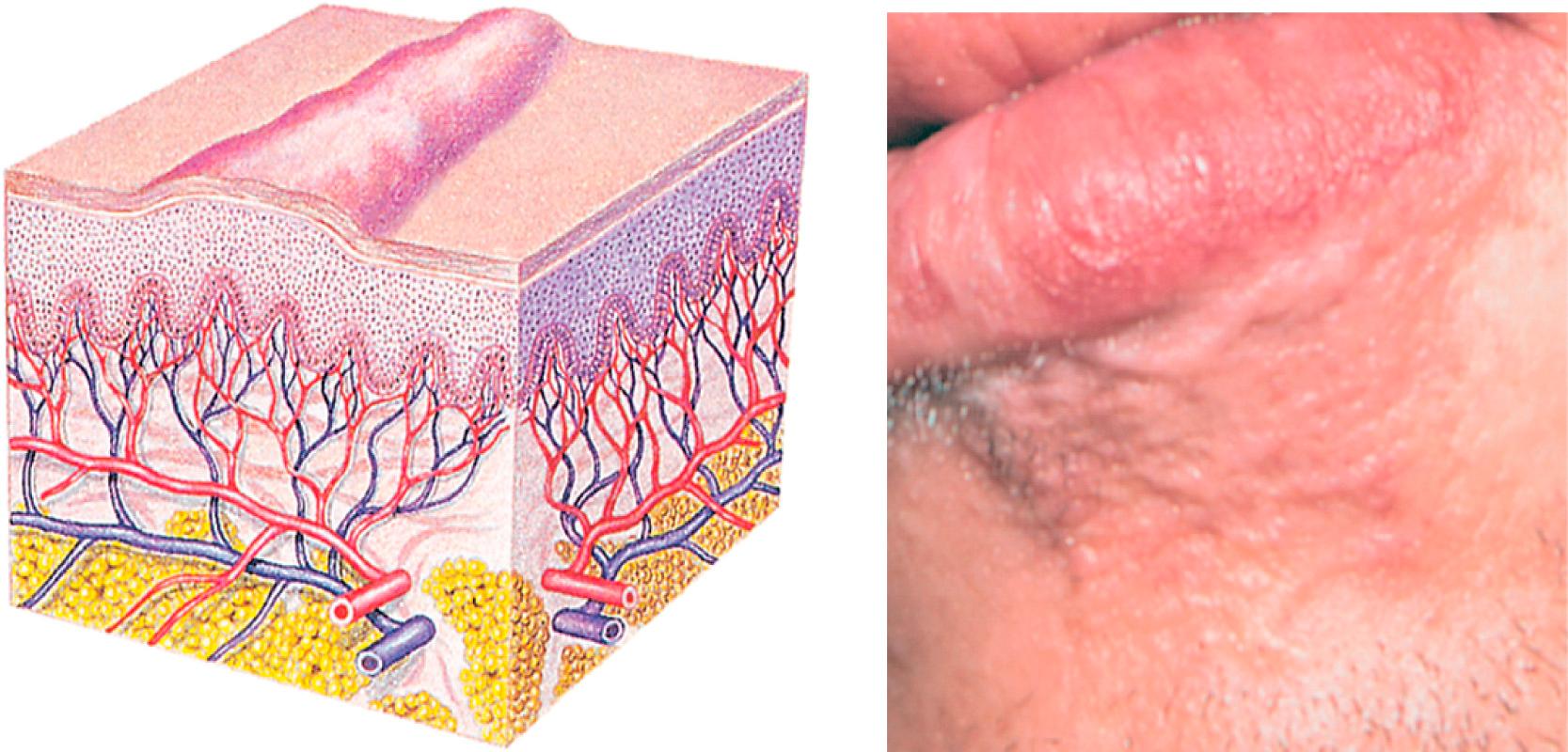
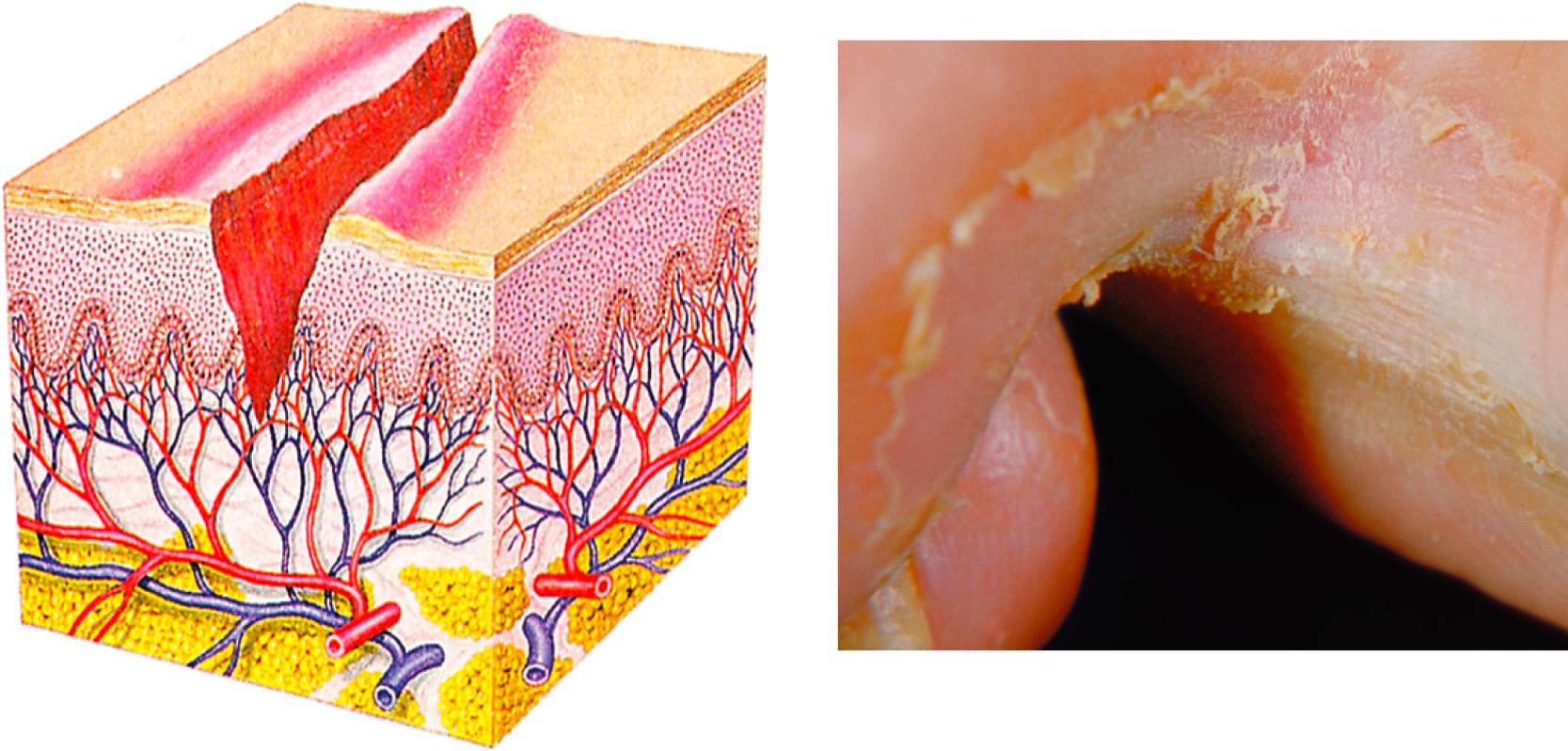
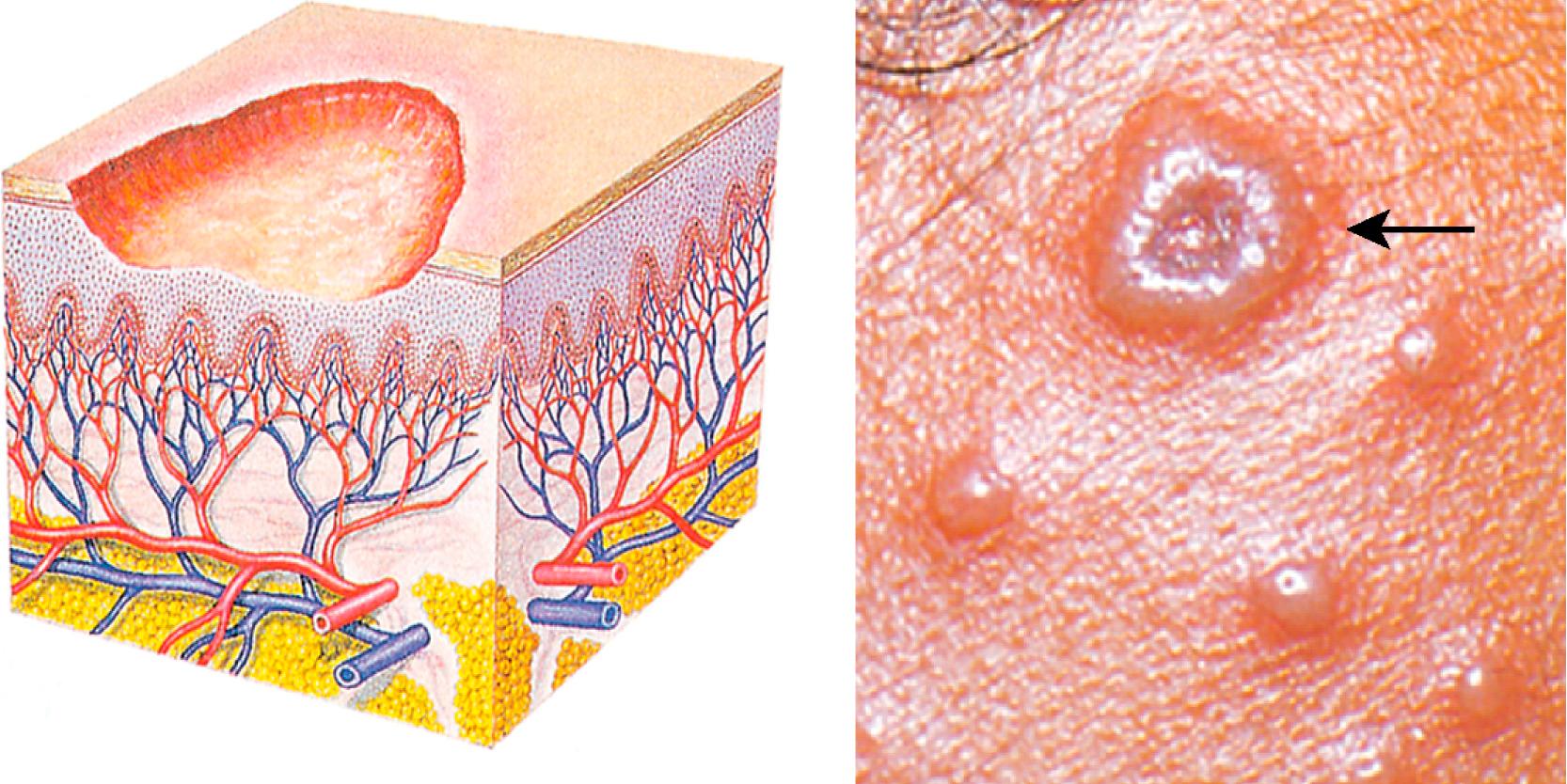
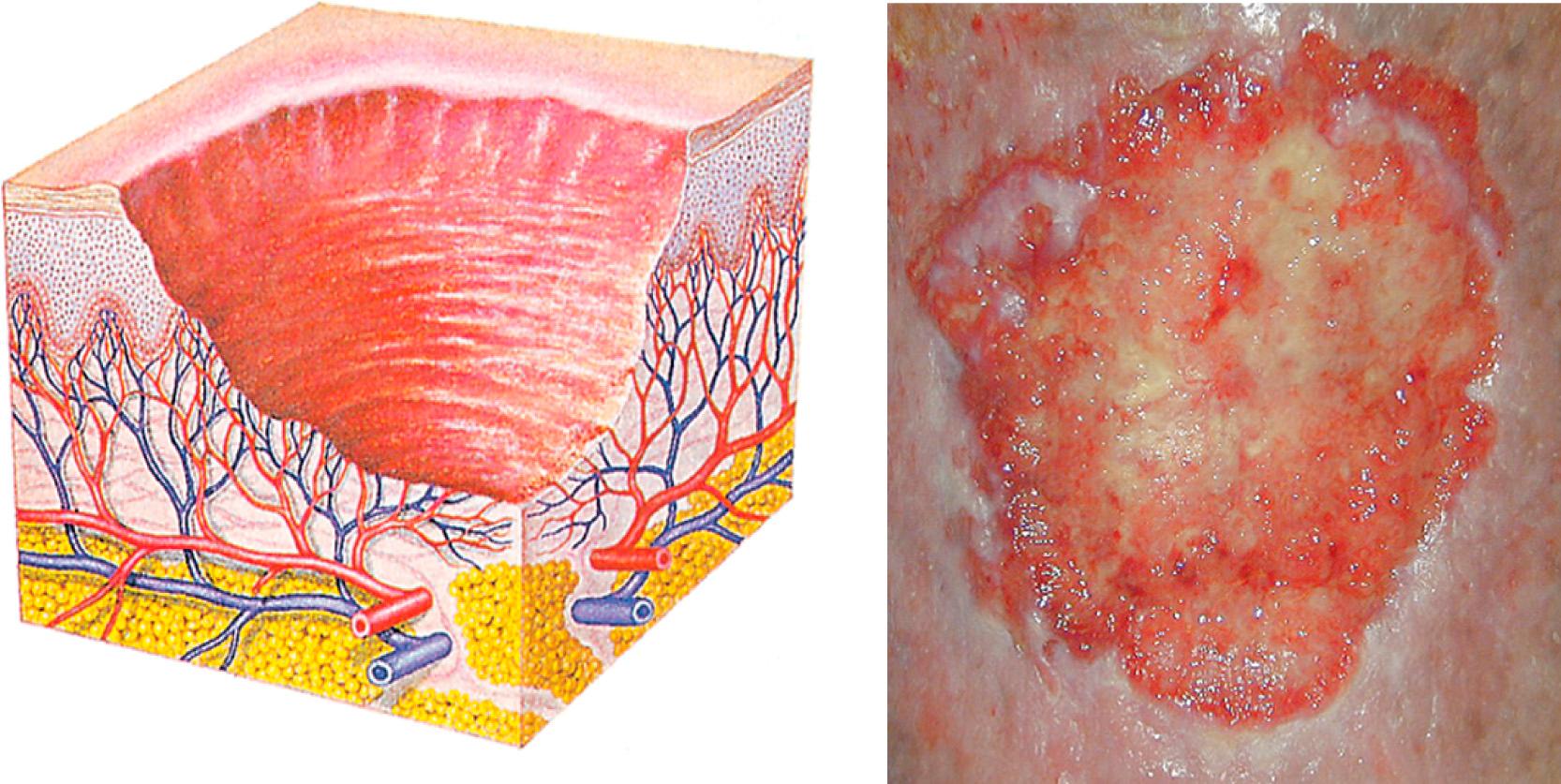
As you assess the skin, pay particular attention to any lesions that may be present. “Skin lesion” is a general term that collectively describes any pathologic skin change or occurrence. Lesions may be primary (i.e., those that occur as initial spontaneous manifestations of a pathologic process) or secondary (i.e., those that result from later evolution of or external trauma to a primary lesion).
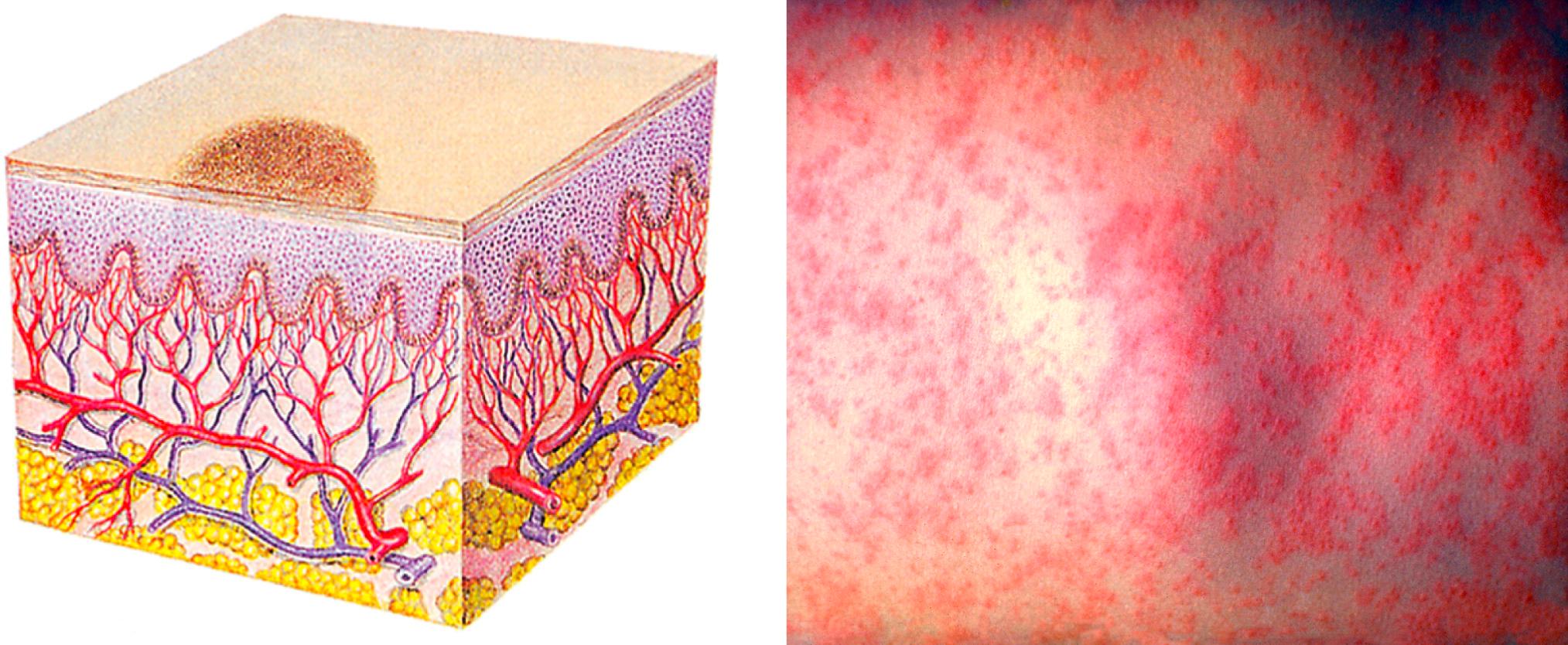
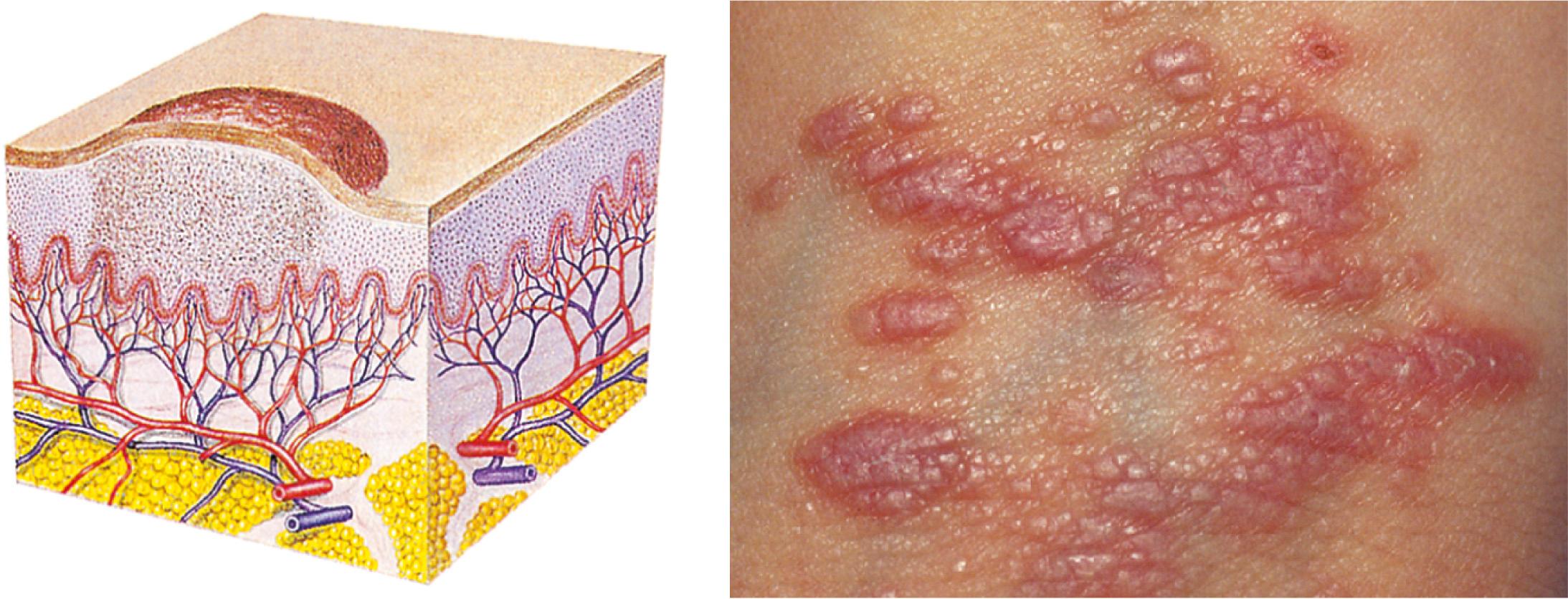
Tables 9.4 and 9.5 show the characteristics of primary and secondary lesions. The nomenclature is often used inaccurately; if you are uncertain about a lesion, use the descriptors rather than the name. Be aware that several types of lesions may occur concurrently and that secondary changes may obscure primary characteristics.
Photos from Public Health Image Library (PHIL), Centers for Disease Control and Prevention: macule/measles, Heinz F. Eichenwald, MD, Bob Craig; Patch/Vitiligo, Brian Hill, New Zealand; Plaque/psoriasis, Richard S. Hibbets; Vesicle/varicella, Dr. John Noble, Jr.; sebaceous cyst, Dr. Gavin Hart; fissure/tinea pedis, Dr. Lucille K. Georg.
Hypertrophic nodule; hypertrophic scar, from Goldman and Fitzpatrick (1994) .
Bulla/blister; papule/lichen planus; keloid, from Weston et al. (2007).
Pustule/acne, from Ferri (2009) .
Tumor/lipoma; telangiectasia; excoriation; lichenification, from Lemmi and Lemmi (2000) .
Scaling, from Baran et al (1991).
Stasis ulcer, from Pozez et al. (2007).
Striae, courtesy Antoinette Hood, MD, Department of Dermatology, Indiana University School of Medicine, Indianapolis.
Describe lesions according to characteristics ( Table 9.6 ), exudates, configuration, and location and distribution:
| Characteristic | Description | Examples |
|---|---|---|
| Distribution | ||
| Localized | Lesion appears in one small area | Impetigo, herpes simplex (e.g., labialis), tinea corporis (ringworm) |
| Regional | Lesions involve a specific region of the body | Acne vulgaris (pilosebaceous gland distribution), herpes zoster (nerve dermatomal distribution), psoriasis (flexural surfaces and skin folds) |
| Generalized | Lesions appear widely distributed or in numerous areas simultaneously | Urticaria, disseminated drug eruptions |
| Shape/Arrangement | ||
| Round/discoid/nummular | Coin-shaped (no central clearing) | Nummular eczema |
| Oval | Ovoid shape | Pityriasis rosea |
| Annular | Round, active margins with central clearing | Tinea corporis, sarcoidosis |
| Zosteriform (dermatomal) | Following a nerve or segment of the body | Herpes zoster |
| Polycyclic | Interlocking or coalesced circles (formed by enlargement of annular lesions) | Psoriasis, urticaria |
| Linear | In a line | Contact dermatitis, poison ivy |
| Iris/target lesion | Pink macules with purple central papules | Erythema multiforme |
| Stellate | Star-shaped | Meningococcal septicemia |
| Serpiginous | Snakelike or wavy line track | Cutanea larva migrans |
| Reticulate | Netlike or lacy | Polyarteritis nodosa, lichen planus, lesions of erythema infectiosum |
| Morbilliform | Measles-like: maculopapular lesions that become confluent on the face and body | Measles, roseola, drug eruptions |
| Border/Margin | ||
| Discrete | Well demarcated or defined, able to draw a line around it with confidence | Psoriasis |
| Indistinct | Poorly defined, have borders that merge into normal skin or outlying ill-defined papules | Nummular eczema |
| Active | Margin of lesion shows greater activity than center | Tinea capitus |
| Irregular | Nonsmooth or notched margin | Malignant melanoma |
| Border raised above | Center of lesion depressed compared with the edge | Basal cell carcinoma center |
| Advancing | Expanding at margins | Cellulitis |
| Associated Changes Within Lesions | ||
| Central clearing | An erythematous border surrounds lighter skin | Tinea eruptions |
| Desquamation | Peeling or sloughing of skin | Rash of toxic shock syndrome |
| Keratotic | Hypertrophic stratum corneum | Calluses, warts |
| Punctation | Central umbilication or dimpling | Basal cell carcinoma, molluscum contagiosum |
| Telangiectasias | Dilated blood vessels within lesion blanch completely, may be markers of systemic disease | Basal cell carcinoma, actinic keratosis |
| Pigmentation | ||
| Flesh | Same tone as the surrounding skin | Neurofibroma, some nevi |
| Pink | Light red undertones | Eczema, pityriasis rosea |
| Erythematous | Dark pink to red | Tinea eruptions, psoriasis |
| Salmon | Orange-pink | Psoriasis |
| Tan-brown | Light to dark brown | Most nevi, pityriasis versicolor |
| Black | Black or blue-black | Malignant melanoma |
| Pearly | Shiny white, almost iridescent | Basal cell carcinoma |
| Purple | Dark red-blue-violet | Purpura, Kaposi sarcoma |
| Violaceous | Light violet | Erysipelas |
| Yellow | Waxy | Lipoma |
| White | Absent of color | Lichen planus |
Size (measure all dimensions)
Shape
Color
Texture
Elevation or depression
Attachment at base: pedunculated (having a stalk) or sessile (without a stalk)
Exudates
Color
Odor
Amount
Consistency
Configuration
Annular (rings)
Grouped
Linear
Arciform (bow-shaped)
Diffuse
Location and distribution
Generalized or localized
Region of the body ( Box 9.6 )
Sunburn
Lupus erythematosus
Pellagra
Porphyria
Irritant contact dermatitis
Miliaria
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here