Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124


 Access video and video lecture content for this chapter online at Elsevier eBooks+
Access video and video lecture content for this chapter online at Elsevier eBooks+
Lower extremity reconstruction following severe trauma, cancer ablation, and chronic infections remains challenging. The involvement of multiple structures from bone, muscle, vessel, nerve to skin makes it difficult to achieve the goals of lower extremity reconstruction where restoration of limb function, coverage for vital structures, and satisfactory appearance is achieved.
In recent years, management of the lower extremity has evolved, with numerous new techniques and innovations and thus extremities are salvaged where they would have been amputated in the past. Introduction of vascularized bone grafting, Ilizarov lengthening, bone matrix, and growth factors to manage the bone defects along with new ideas for coverage like perforator flaps, propeller flaps, negative pressure therapy and increased knowledge for anatomy has led to successful management of lower extremity soft-tissue and bone defects. If the extremity cannot be salvaged, the next goal would be to maintain maximal functional length with good soft-tissue coverage on the stump to bear the prosthesis for functional gait.
Extremity salvage is a long and complex process for the medical professionals as well as patients. Patients and family members must be educated, included in the decision-making process, and made aware of expected prognosis. The patient’s motivation and compliance along with the family’s support will be critical during physical and psychological recovery.
Although early amputation and prosthetic treatment was thought to offer the potential of faster recovery and lower cost, recently reports have provided different views. A multicenter, prospective, observational study to determine the functional outcome of 569 patients with severe leg injuries resulting in reconstruction or amputation has provided information based on Sickness Impact Profile, a measure of self-reported health status. Although reconstruction may be faced with more challenging process, the Lower Extremity Assessment Project, or LEAP study, showed no significant difference in outcome at two years. Costs following amputation and salvage were also derived from data in a study that emerged from the Lower Extremity Assessment Project concluding that amputation is more expensive than salvage and amputation yields fewer quality-adjusted life-years than salvage. Other reports have shown similar findings where projected lifetime healthcare cost for amputation may be as high as three times.
Treatment of salvage evolves as with the coverage strategy. But still this process can be long and complicated. Although normal function and appearance can be difficult to achieve, it may be warranted to support successful reconstruction leading to successful salvage of the extremity.
The early history of lower extremity reconstruction dates back to Hippocrates (460–370 BC), and amputation and procedures trying to improve the success of amputation and survival were the main practice up to World War I.
Although the term flap originated in the 16th century from the Dutch word flappe , meaning something hanging by one side, and the concept dates back as far as 600 BC when Sushruta Samhita described nasal reconstruction using a cheek flap, it was not until the First and Second World Wars that pedicled flaps were used extensively for reconstruction of the extremity. The next evolution came as surgeons started to use axial pattern flaps. The term “axial pattern” used to describe flaps with named pedicles was presented by McGregor and Morgan and this concept, along with contributions from many surgeons, led to the understanding of the hemodynamic aspect of flap circulation. The first muscle flap for lower extremity coverage was first described by Stark for coverage of debridement sites for osteomyelitis but went unnoticed till Ger reported that the leg muscles were reliable for leg coverage with abundant blood supply. These progresses led to the distinction between axial and random flaps and muscle and musculocutaneous flaps which led to the introduction of free tissue transfer.
Prior to the introduction of microsurgery, limitations existed to reconstruct large and extensive wounds including bone defects. With the beginning of the era of microsurgery, tissue coverage for extensive and complex defects, even after severe trauma and radical debridement, truly allowed advances in lower extremity coverage. In 1986, a landmark publication for reconstructive microsurgery in the extremity was presented by Marko Godina, where he established the principle of early debridement, free tissue transfer and aggressive rehabilitation to achieve functional limb after salvage. Based on this principle and advances made in the new millennium, treatment for infected wounds like osteomyelitis, complicated wounds such as diabetic foot ulcers and ischemic limb, and large defects after cancer ablation now turns routinely to soft-tissue coverage using microsurgery. With respect to function, free functioning muscle transfer using rectus femoris muscle and gracilis muscle and composite free flaps such as dorsalis pedis with extensor tendons or fibula osteocutaneous flaps may achieve acceptable functional results in the extremity with composite defects. Innervated flaps utilizing microsurgical coaptation of nerves may help regain early protective sensation for sole reconstruction. Tissue expansion technique combined with or without microsurgery may allow coverage for large chronic defects or healed scars, minimizing donor morbidity. The most recent advances in flap surgery came in the 1990s with the introduction of perforator flaps. Koshima and Soeda described the use of an inferior epigastric artery skin free flap without rectus abdominis muscle for reconstruction. This implied reduction of donor site morbidity, being able to be tailored regarding thickness, and increased freedom of orientation of pedicle allowing more flexibility while providing coverage of the defect. Advances in wound healing science have synergistically made closure of lower extremity wounds more successful. The vacuum-assisted closure may provide stable temporary dressing, which allows increased blood flow and decreased bacterial counts to allow a better environment for flap coverage.
Currently, state-of-the art technologies in tissue engineering, genetic engineering, diagnostic technology, wound healing, limb transplantation, and supermicrosurgery will widen the possibility for increased salvage with better function and appearance. Nevertheless, the concept of soft-tissue coverage with or without microsurgery will remain as an essential part of functional and cosmetic recovery for lower extremity reconstruction.
The primary goal of surgical reconstruction of the lower extremity wound is to restore or maintain function. Function is addressed through a well-vascularized extremity, skeletal structure able to support gait and weight-bearing, and innervated plantar surface to provide protective sensation. Without proper function, the value of reconstruction will be reduced, significantly increasing emotional and financial burden to the patient.
An evaluation of the patient as a whole allows proper decisions to be made with regard to systemic conditions, socioeconomic status, and rehabilitative potential. Extremity injuries are best approached by teams of surgeons with knowledge of skeletal, vascular, neurologic, and soft-tissue anatomy. Although evaluations such as the Mangled Extremity Severity Score (MESS), the Predictive Salvage Index, and the Limb Salvage Index can assist the team in making a decision for amputation, they must not be used as the sole criterion and the decision to amputate must be individualized for each patient.
Whether acute or chronic, evaluation of lower extremity wounds and the eligibility for soft-tissue reconstruction begins with vascular status evaluation. If clinical and diagnostic examination reveal inadequate perfusion and the value of reconstruction minimal, amputation should be individually decided. An amputated or avulsed tissue should never be disregarded, especially in acute traumas, unless severely contaminated or lacking vascular structure. Nothing can mimic the superiority of an autologous tissue, and all tissues from amputated parts should be considered as potential donor tissues for reconstruction. The skin harvested from the degloved or amputated part can be utilized as biologic dressings to permanent skin grafts ( Fig. 5.1A–E ). The leg length can be preserved using soft tissue distal from the zone of injury as fillet pedicled or free flaps. Amputated bones can be banked or used as a flap to reconstruct the leg.
 This 67-year-old patient was involved in a pedestrian traffic accident, which left her with ≈90% degloving injury of the entire left leg. (B,C) The injury involved major artery and nerve defects making salvage impossible and resulting in below-knee amputation. The skin was harvested and defatted from the degloved tissues and grafted in hope of primary take as well as biologic dressings. (D,E) Only about 15% of the initial graft was taken, but healthy granulation was noted underneath the biologic dressing and made a favorable bed for secondary graft procedure.")
Once the wound is evaluated to have good vascular supply, stable skeletal structures and a relatively clean wound, soft-tissue coverage is then considered. The concept of a reconstructive ladder was proposed to achieve wounds with adequate closure using a step-ladder approach from simple to complex procedures ( Fig. 5.2A ). Although still valued and widely taught, the reconstructive ladder comes from the concept of the wound-closure ladder dating back beyond the era of modern reconstructive surgery. In the era of modern reconstructive surgery, one must consider not only adequate closures but form and function. A skin graft after mastectomy can still provide coverage but a pedicled TRAM (transverse rectus abdominis muscle) flap will provide superior results in addition to coverage. Now with introduction of DIEP (deep inferior epigastric perforator) flaps, the reconstructive ladder approach seems to show more flaws. Other techniques including tissue expansion, skin stretching, and vacuum-assisted closure have made new changes in approaching reconstructive options. A simpler reconstructive option may not necessarily produce optimal results. This is especially true for lower extremity coverage, where consequences of inadequate coverage will lead to complications such as additional soft-tissue loss, osteomyelitis, functional loss, increased medical costs, and even amputation. Thus, to provide optimal form and function, we jump up and down the rungs of the ladder. The reconstructive elevator requires creative thoughts and considerations of multiple variables to achieve the best form and function rather than a sequential climb up the ladder ( Fig. 5.2B ). This paradigm of thought does not eliminate the concept of the reconstructive ladder but replaces it as a ladder of wound closure and makes its mark in the field where variety of advanced reconstructive procedures and techniques is not readily available. Based on the reconstructive elevator, the method of reconstruction should be chosen based on procedures that results in optimal function as well as appearance.

Autologous skin grafts are used in a variety of clinical situations. They can be full- or partial-thickness and require a recipient bed that is well vascularized and free of bacterial contamination. The split-thickness grafts are usually used as the first line of treatment where wounds cannot be closed primarily or undue tension is suspected. In the extremity often with complex wounds – bone exposure and/or avascular beds, infected wounds, wound with dead space and poorly coagulated beds – skin grafts should be avoided. Autologous cultured keratinocytes can be used where split-thickness donor sites are limited. However, the use of cultured epithelial autograft has been hampered by reports that show it to be more susceptible to bacterial contamination, to have a variable take rate, and to be costly.
A skin substitute is defined as a naturally occurring or synthetic bioengineered product that is used to replace the skin in a temporary, semi-permanent, or permanent fashion. Temporary epidermal replacements may be beneficial in superficial to mid-dermal depth wounds. In deeper wounds, dermal replacements are of primary importance. Bioengineered products for superficial wounds are porcine products such as EZ Derm and Mediskin (Brennen Medical, LLC, Saint Paul, MN), which help to close the wound, decrease pain, and improve the rate of healing. Biobrane (UDL Laboratories Inc., Rockford, IL) is a bilaminate skin substitute that is used temporarily. The outer layer is formed of a thin silicone layer with pores that allow removal of exudates and penetration of antibiotics. The inner layer is composed of a three-dimensional nylon filament weave impregnated with type I collagen to adhere to the wound. Bioengineered products that are used for deep wounds are Allograft, Alloderm (Life Cell Corporation, Woodlans, TX), Integra (Integra Life Sciences, Plainsboro, NJ), and Apligraf (Organogenesis Inc, Canton, MA). The gold standard for temporary skin coverage is cadaver skin or allograft. Allograft is used to cover extensive partial- and full-thickness wounds. It prevents tissue desiccation, decreases pain and the insensible loss of water, electrolytes and protein, suppresses the proliferation of bacteria, and decreases the hypermetabolic component of thermal injuries. Alloderm is an acellular dermal matrix engineered from banked human cadaver skin. It can also provide single-stage reconstruction when used with a split-thickness skin graft. Alloderm is known to improve functional and cosmetic results in deep burn wounds ( Fig. 5.3 ). Integra is an acellular collagen matrix composed of type I bovine collagen cross-linked with chondroitin-6-sulfate and covered by a thin silicone layer that serves as an epidermis. It is readily available and does not require a donor site, converts open to closed wound, and decreases metabolic demand on the patient. However, Integra must be used on clean wounds and requires a two-stage procedure later for the graft. Simultaneous use with negative wound pressure therapy may accelerate the vascularization. Apligraf is a bilaminate human epidermal and dermal analogue that can act as a permanent skin substitute. The epidermal layer is formed by human keratinocytes with a well-differentiated stratum corneum. The dermal layer is formed with bovine type I collagen lattice impregnated with human fibroblasts from neonatal foreskin. Apligraf is not antigenic and the dermal layer incorporates into the wound bed. Apligraf has been shown to significantly decrease the time of venous ulcer healing compared to compression.

The thigh can be divided into 3 parts: the proximal thigh, mid-thigh, and the distal thigh (supracondylar knee) regions.
The proximal thigh wounds can result from various causes such as complications from hip fractures, infected bypass vascular graft, after tumor resection, and trauma. The medial portion of the proximal thigh can be especially challenging due to location of vital structures and the likely formation of dead space. Local lower extremity muscle or myocutaneous flap options include using the flaps based from the lateral circumflex femoral artery, such as tensor fascia lata, vastus lateralis, and rectus femoris flaps. Vertical rectus abdominis muscle or myocutaneous flaps using the deep inferior epigastric artery can allow stable coverage of the proximal thigh. The gracilis muscle or myocutaneous flap based on the medial femoral circumflex artery may lack muscle bulk but is a good option when the dead space is not extensive. Now with increased knowledge of perforator and perforator-based flaps, basically any perforator can be chosen as a source of vascular supply to the skin flap and be rotated to cover a defect known as the propeller flap. When the use of local flaps is not feasible due to the complexity of the wound, free tissue transfer is indicated.
The mid-thigh wound, due to the anatomical character where femur is surrounded by a thick layer of soft tissue, rarely requires reconstruction using free tissue transfer and often is sufficiently reconstructed by skin graft or local flap. Local muscle or musculocutaneous flaps based on the lateral or medial femoral circumflex artery can be used when available. Also, any perforator can be chosen as a source of vascular supply to the skin flap and be rotated to cover a defect. However, if the patient has undergone massive resection or has special considerations such as postoperative radiation therapy, it may warrant free tissue coverage.
The wounds of the distal thigh (supracondylar knee) can be very difficult due to the limit of rotation from previously described local muscle or musculocutaneous flaps from the thigh. Pedicled medial gastrocnemius muscle or musculocutaneous flap from the lower leg can be extended to cover this region. However, extensive or complex defects may require free tissue transfer or coverage using a perforator-based rotation (propeller) skin flap ( Fig. 5.4 ).
 A 70-year-old patient is noted with chronic drainage after failed total knee replacement. (B) After complete debridement, a perforator-based flap was elevated and advanced using a perforator (dissected until just beneath the fascia) with visible pulse. (C) Long-term follow-up shows no recurrence of any infections, allowing her to undergo total knee replacement.")
The traditional planning for reconstruction of the lower extremity has been approached according to the location of the defect. It is divided into thirds: gastrocnemius muscle flap for the proximal third, soleus muscle flap for the middle third, and free flap transfer for the distal third of the leg. Like the reconstructive ladder concept, this traditional approach can be useful, but the surgeon must individualize each wound and choose the initial procedure that can yield the best chance of success and avoid morbidity.
One must choose a proper surgical plan to achieve optimal function and cosmesis. Flaps are selected based on accessibility of local tissue and donor morbidity. Lower extremity trauma, due to the high energy impact, frequently results in extensive and complex wounds. Workhorse flaps for soft-tissue coverage include muscle or musculocutaneous flaps such as latissimus dorsi, rectus abdominis, and gracilis. The perforator flap, where a skin flap is based on a single or multiple perforators, such as the anterolateral thigh flap or thoracodorsal artery perforator flap, has been added to the list.
Whichever flap you select, the guideline for lower extremity reconstruction using free flaps remains the same: anastomose the vessel outside the zone of injury, make end-to-side arterial anastomosis and end-to-side or end-to-end venous anastomosis, and reconstruct the soft tissues first and then restore the skeletal support.
The initial evaluation of the lower extremity wound involves visual and manual examination. An examination on the location, size, depth, and character of the wound is made. Neurological evaluation, as well as vascular and skeletal evaluation, is made to develop a plan for reconstruction. Also, presence of comorbidities including smoking, diabetes, obesity, and peripheral vascular disease should be accounted for. The initial evaluation allows for assessment of overall function and consideration of possible outcome. One must not make the mistake of addressing the wound locally but rather approach the patient as a whole and also take into consideration socioeconomic status, rehabilitative potential, the patient’s motivation, and compliance.
After the decision is made to reconstruct the lower extremity, the first preoperative evaluation should start with vascular status. Physical examination of palpable pulse, color, capillary refill, and turgor of the extremity allows the surgeon to assess initial status, and Doppler examination can provide additional information. The use of preoperative arteriography for lower extremity reconstruction is considered when physical/Doppler exam reveals inconclusive vascular status or chronic vascular disease is suspected ( Fig. 5.5 ). The use of computed tomographic angiography may obtain vascular information of the recipient region without the risk of complications from arterial puncture of the groin and also can provide vascular information of the donor flap facilitating the planning and the surgical procedure. In association with prior injuries to the lower extremity, the routine preoperative use of angiogram is controversial. It is selectively recommended in patients who have loss of one or more peripheral pulses, a neurologic deficit secondary to the injury, or a compound fracture of the extremity that has undergone reduction and either external or internal fixation. As an easier solution to obtain vascular status not only for the injured or ischemic limb but to evaluate the flap pedicle status, the use of duplex ultrasound has been increasing steadily. It is minimally invasive and provides accurate anatomic as well as additional physiologic information that can be useful in planning for reconstruction.

Nerve injuries that are irreversible may require special considerations. Peroneal nerve injuries result in foot drop and loss of sensation of the dorsum of the foot. Thus, lifelong splinting or tendon transfers may be required. Complete loss of tibial nerve function results in loss of plantar flexion and is an absolute contraindication for reconstruction. The loss of plantar sensation can be devastating and may hinder the need for reconstruction although it is not an absolute contraindication.
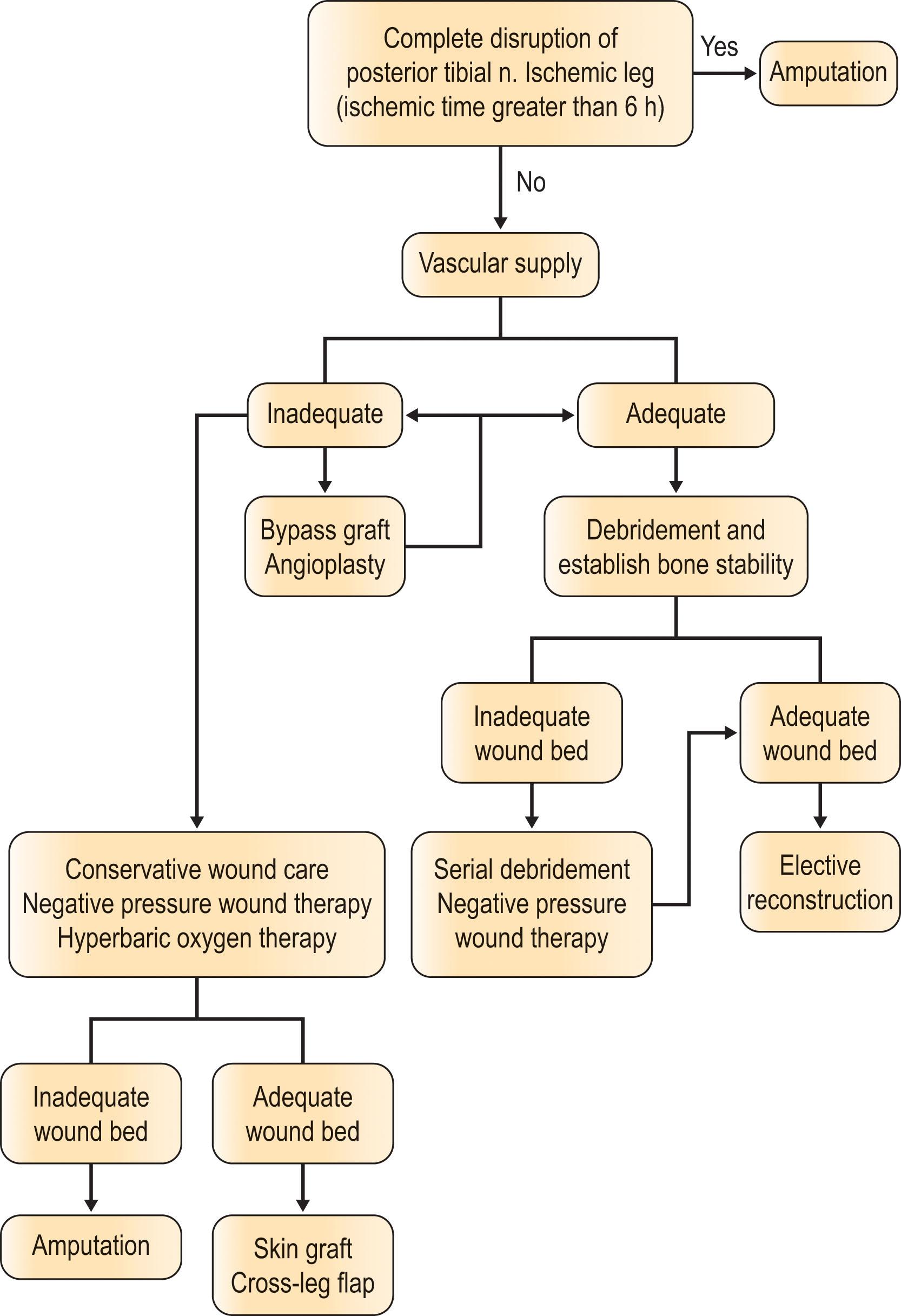
The approach is outlined in Algorithm 5.1 .
A study by Lange describes absolute and relative indications for primary amputation of limbs with open tibial fractures. Absolute indications include anatomically complete disruption of the posterior tibial nerve in adults and crush injuries with warm ischemia time greater than 6 hours. Relative indications include serious associated polytrauma, severe ipsilateral foot trauma, and anticipated protracted course to obtain soft-tissue coverage and tibial reconstruction.
In these cases where limb salvage is not possible, attempt should be made to salvage as much limb length as possible. Every effort should be made to save the functional knee joint as below-knee amputation results in far superior ambulatory outcome and up to two- to threefold more full mobility compared to above-knee amputation. The energy consumption is far less for below-knee amputation, and this allows these patients to walk significant daily distance thus maintaining good quality of life. Though the ideal stump length below the knee is greater than 6 cm, any length of tibia should be preserved. If adequate soft tissue exists, the stump may be closed primarily and where local tissue is inadequate, microsurgery allows preservation of the maximal length of the stump. If the tissue distal to the amputation is usable, a fillet flap can be performed. Other flaps such as muscle, musculocutaneous, fasciocutaneous, and perforator flaps can be used for microsurgical reconstruction and also achieve the same goal. Muscle flaps may have a tendency to heal slowly and to shrink due to muscle atrophy while skin flaps may provide better contour and sensibility.
Bony stability is first established using external or internal fixation devices. An external device is usually preferred if there is significant bone loss or bone revascularization and may facilitate coverage procedure. Debridement must cover devitalized soft tissue and bone and be performed until fresh bleeding is noted. Multiple stages of debridement may be needed to achieve adequate wound bed prior to soft-tissue coverage.
The vacuum-assisted closure can be used to optimize the wound bed and minimize dressing changes until definitive reconstruction. It must be used with caution and in conjunction with serial debridement. It does not replace surgical debridement and should not be used in heavily contaminated wounds with necrotic tissue. If a lower extremity wound is clean, bony stability is present, and no vital structures are exposed, application may be indicated. This device facilitates dressing of the wound and often promotes healing.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here