Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Access video content for this chapter online at Elsevier eBooks+ 
The new age of social media presence and identity places a far greater importance on the face and its appearance than ever before. Burns involving the face interfere with identity, aesthetics, and basic functions like speech and expression of thoughts and feelings. Certain structures like the lip and eyelid are irreplaceable, and there is no tissue in the body which can achieve the “like for like” principle in their reconstruction. Constituting almost 50% of all burn injuries, burns of the head, neck, and face region deserve special consideration in their management. The rich vascular supply of the face helps in rapid heat dissipation limiting the depth of burns often to just partial-thickness injury. Burns involving the face also present with tell-tale signs of the more sinister and hidden danger of inhalation injury, one of the top causes of mortality in the burn patient. Management of facial burns is a multidisciplinary team effort involving the burn surgeon, trained nurses, the therapist, and the psychosocial support team.
With the advent of the SARS-CoV-2 (COVID-19) pandemic, facial burns have become more relevant in terms of the risk entailed by the healthcare worker involved in wound care. Surgical decisions in individuals affected by the virus may have to be put off for a more conservative approach. Advanced wound care products that may reduce the dressing frequency and hence viral load of exposure to the healthcare worker may be preferred. The ramifications of burn care in affected patients are still unfolding, and evidence continues to accumulate regarding the protocols which may be needed to be followed in these difficult times.
An effective scar management protocol goes a long way toward achieving the ultimate goal of deformity and contracture prevention. The psychological overlay associated with the condition of facial burns cannot be overstated. The ultimate goal is an empathetic but realistic approach to help the survivor overcome psychological distress and achieve social reintegration.
The face has a complex architectural makeup with sensory, mimetic, and sphincteric functions while playing an important role in heat and fluid homeostasis.
The head and neck region can be involved in burns caused by transfer of thermal, chemical, electrical, or lightning energy to the skin. Injury to the epidermal layer alone comprises first degree burn. With increasing energy and contact duration, increasing depths of the dermis are also damaged. This constitutes denaturation of collagen and thrombosis of blood vessels. A pink-appearing dermal layer indicates a superficial burn whereas it turns more whitish in appearance with increasing depth.
Burn wound re-epithelializes from the remnant adnexal structures like pilosebaceous units, sweat glands, and apocrine glands, which occur in a high density on the face and scalp. Burn wounds taking longer than 3 weeks to heal may be prone to considerable scarring and hypertrophy. However, a decision to surgically intervene needs to be taken by the end of the first week of treatment and is based solely on the experience and clinical judgment of the treating burn surgeon. Another factor that has a bearing on the burn depth is the skin thickness, which varies with the age, sex, and anatomic location on the face. Children have relatively thinner skin. Skin thickens with age and starts thinning again after the fifth decade of life. Men have thicker skin compared to women. Eyelid and postauricular skin is thinner (0.5 mm thick) than other anatomic areas on the face.
Goals of facial burn management are to obtain early wound re-epithelialization, pain control, and to minimize functional sequelae while taking care to preserve aesthetic landmarks. Certain special features that make facial burns unique are the rich vascularity, which hastens healing and reduces infection rate, difficulty in accurate depth assessment, and the potential to cause contour deformities by aggressive surgical management.
The treatment principles can be broadly classified into three groups based on the depth of the burn:
In patients who have sustained epidermal and superficial partial-thickness burns, spontaneous healing is the rule. The mainstay of treatment involves open dressings and topical care ( Fig. 20.1 ).
 2-year-old child with facial burns due to scalds. (B) Collagen sheets have been applied. (C) Face healed and sheet separating in other places on chest. (D) Result at 3 months.")
In patients who have sustained deep or full-thickness burns estimated at initial evaluation, the apparent next step is to proceed with workup and early excision of the burn wound with coverage (dermal substitute, allograft or autograft).
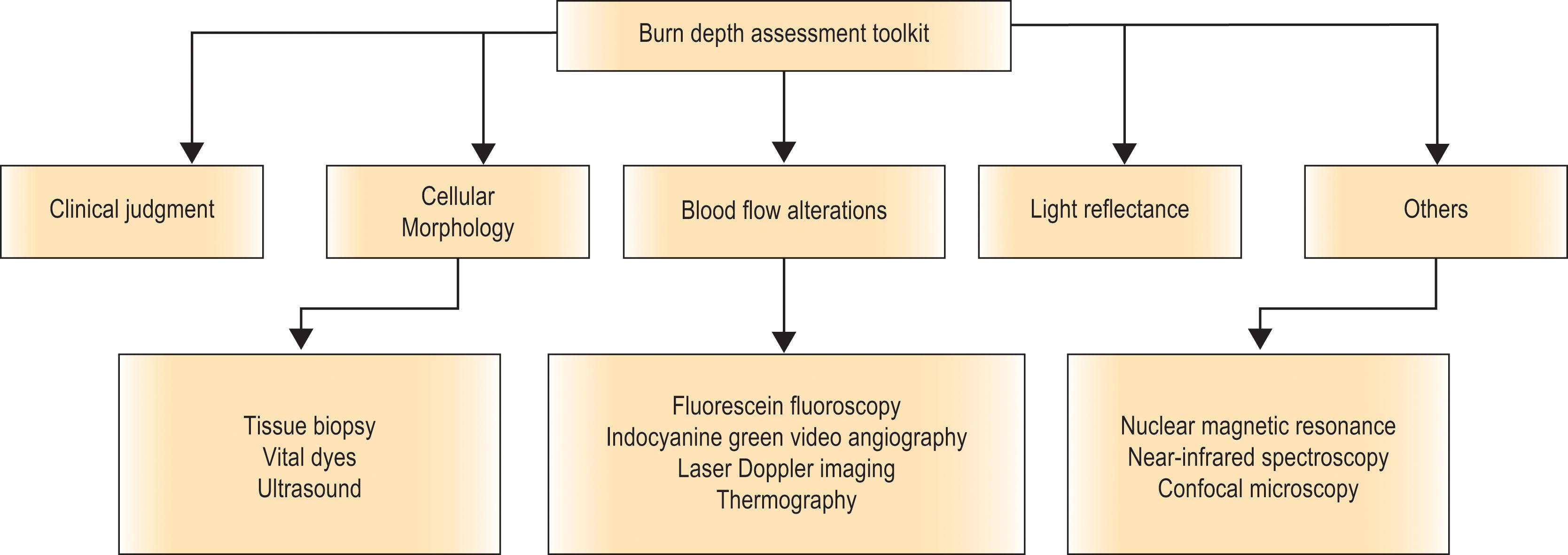
The third group of patients with intermediate or indeterminate thickness of burns incites the most controversy or dilemmas in management. If excised too early the patient may end up with grafts in areas that may have appeared aesthetically superior if allowed to heal conservatively. On the other hand, waiting too long may lead to development of hypertrophic scars ( Figs. 20.2 & 20.3 ). Herein lies the role of diagnostic tools for diagnosing burn depth. There are many diagnostic tools for burn depth assessment ( Algorithm 20.1 ). One such advancement is the laser Doppler technique. Though lacking level 1 evidence, laser Doppler imaging done between 48 and 72 hours post-burn injury was shown to predict depth with an accuracy of 97% when compared to 70% accuracy of clinical judgement. A treatment decision delayed until 10 days may help in determining the areas that are deeper and will require surgery.
 Deep partial-thickness and full-thickness burns in a patient with high TBSA burns on day 10. (B) Managed by conservative treatment and no surgical intervention, healing at 4 weeks. (C) Hypertrophic scarring at 4 months.")
 35% mixed flame burns in a 4-month-old child – at 5 days on presentation to us from another facility. He was managed with conservative management and later grafting. (B) At 3 months post-burn. (C) At 6 months post-burn.")
Facial burns should receive emergent care in the form of prolonged washing with clear running water or saline to reduce the depth. In the case of chemical injury, the particular antidote if available should be immediately used, or water can be used for at least an hour to dilute the noxious agent. Facial burns often act as a marker for upper or lower airway injury. An early decision has to be made regarding intubation or for elective tracheostomy before signs of laryngeal edema develop. Special care has to be taken to prevent tube pressure necrosis.
It is the practice in the authors’ unit to cover all facial burn injuries with synthetic bovine collagen dressing ( Fig. 20.4 ) ( ). This helps in maintaining a closed environment, reducing the pain and distress, retaining moisture, and helping in rapid re-epithelialization in first and second degree burns (see Fig. 20.1 ). In deeper burns this dressing does not adhere well to the wounds and is seen to peel off within 48 hours and thus also acts as a guide in burns of indeterminate depth.

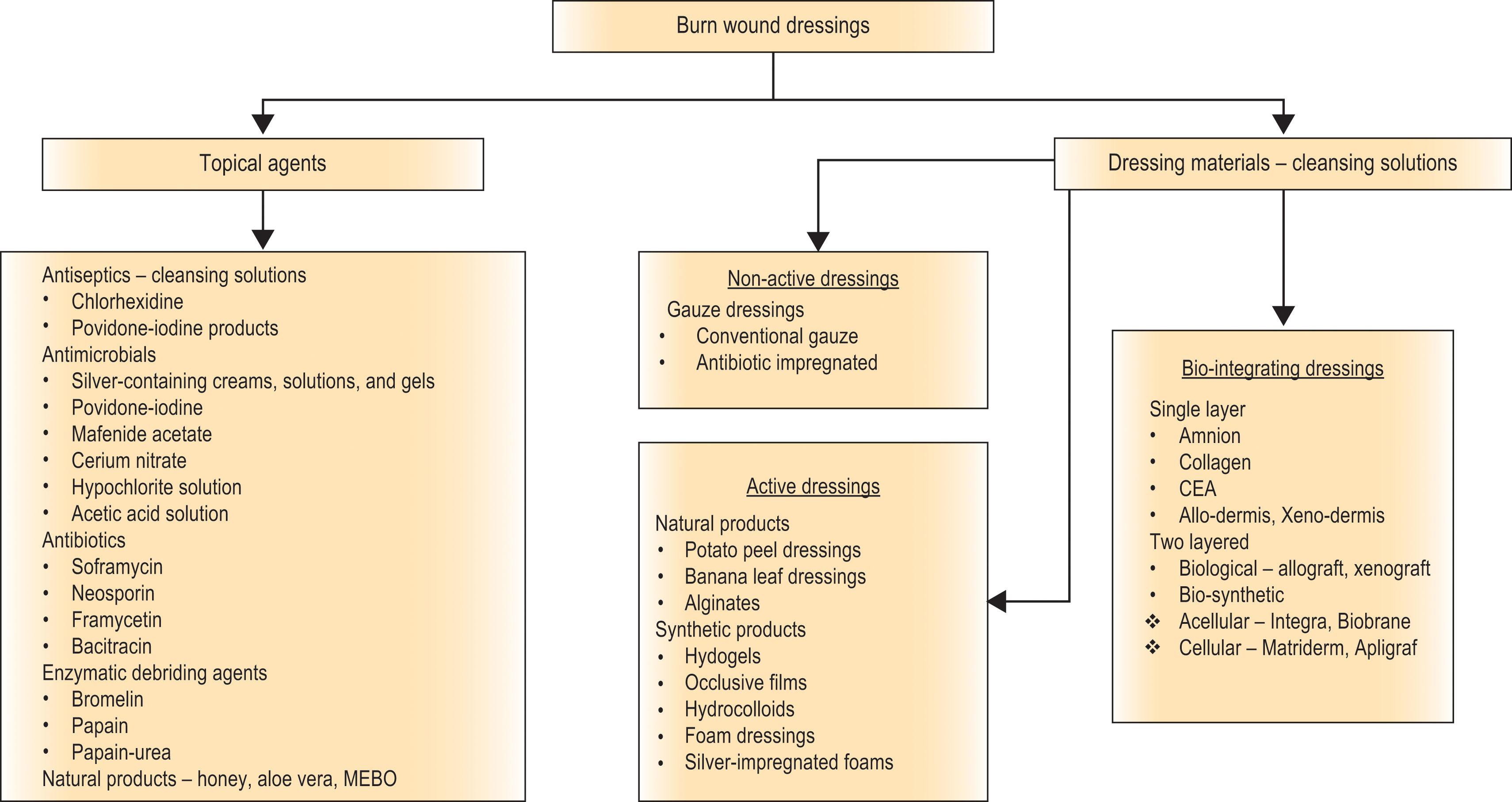
The face is one of the rare regions of the body where there are equal proponents advocating open and closed methods of burn wound care to this day. Closed dressing is advocated due to certain advantages like assisting keratinocyte migration, moist wound environment, growth factor retention, pain relief, etc. Open dressing would need repeated application of topical agents, failing which the wounds would tend to crust and form scabs which may lead to development of raw areas and oozing. The burn wound dressings on the whole can be classified as shown in Algorithm 20.2 .
The facial burn wounds are cleaned daily with a cleansing solution like normal saline or sterile water to gently remove crusts and necrotic material. A cream-based topical agent with paraffin gauze application or any of the biological/synthetic skin substitutes can be used for cover as per the protocol of the burn unit.
Some of the more commonly used topical agents for wound care include the following:
Silver sulfadiazine (SSD) cream introduced by Fox in 1968 is the mainstay of burn wound management in many burn units worldwide. A combination of SSD with epidermal growth factor is seen to counter the deleterious effects of SSD on healing. Nanocrystalline silver dressings like ACTICOAT (Smith and Nephew) Urgotul Ag (Urgo) have been described to have good antimicrobial and desloughing properties.
Mafenide acetate is a deep eschar-penetrating agent with good antimicrobial spectrum. Available commercially as 5% and 11.1% solutions, it has been recommended for areas of the face like ears, where cartilaginous framework is exposed by burns though its application has been reported to have caused pain.
Antibiotics and antifungals: commonly used preparations include Neosporin, Polysporin, and bacitracin.
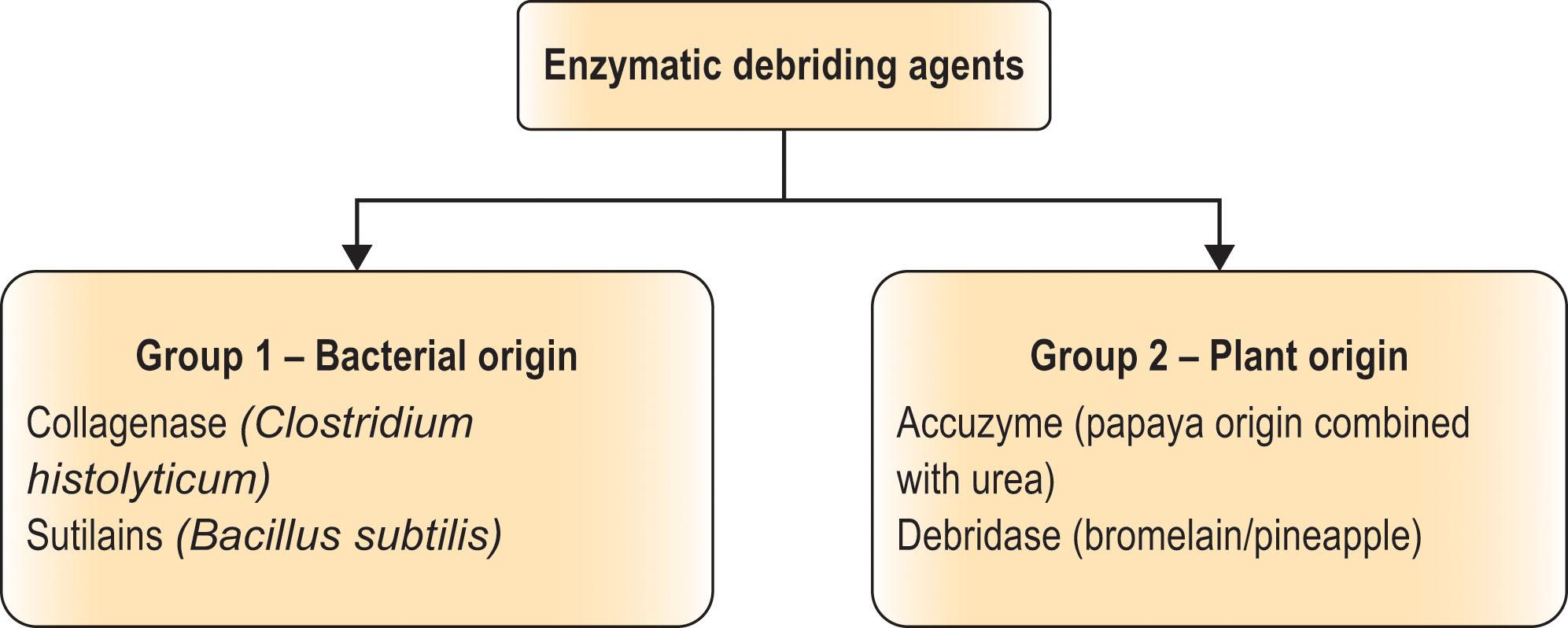
Enzymatic debriding agents: these chemical agents belong to one of two groups ( Algorithm 20.3 ). Recent studies indicate use of bromelain-based enzymatic debridement methods in mid to deep dermal burns show reduced time to complete wound closure and hospital stay, reduced need for surgical debridement procedures, autologous grafting, and better depth determination and final scar characteristics in terms of color, thickness, and pliability. Because of its dermis-preserving properties it is highly recommended for use in facial burns by consensus studies.
Skin substitutes may find a special niche for use in pediatric burns, which are usually small area burns, partial-thickness, and need only dressings for their management. They reduce the frequency of dressings, associated pain, and emotional trauma, and promote an early return to activities.
Some of the commonly used bioactive skin substitutes in head and neck burns include the following:
Biological dressings: amniotic membrane has been shown in clinical trials to be effective as a temporary wound cover, reducing pain and helping rapid re-epithelialization, but has not been seen to alter scar properties.
Synthetic dressings: these provide a moist wound environment and effectively seal off the wound. Some of these are water vapor permeable and allow the wound to respire. Commonly used brands include DuoDERM, OmniDerm, Opsite, and Suprathel. Hydrogel-based polymer masks (polyurea–polyurethane) containing 60% water have been described to have an excellent outcome in terms of reducing pain, scar outcomes, and facilitating wound observation.
Biosynthetic materials: these combine a biologic component with a synthetic one. The biologic component comprises fibroblasts, which proliferate producing dermal collagen, matrix proteins, and growth factors forming a scaffold over which epithelialization occurs or epithelial grafting needs to be done to hasten healing. Some commonly used examples include Integra, Biobrane, TransCyte, and Dermagraft.
Other skin substitutes: the other skin substitutes of notable mention include Xenoderm, Alloderm, Apligraf, and Epicel. These comprise a dermal latticework which could be monolayered acellular as in Xenoderm and Alloderm, and derived from porcine, bovine, or human cadaver skin combined occasionally with epidermal cells of human keratinocyte origin (Apligraf) or epithelial cells grown from patients’ own skin (Epicel). Cadaver allografts and xenografts are biological bilayered skin substitutes usually used after excision of full-thickness burns, but their use has also been described as a dressing material in partial-thickness facial burns.
Tangential excision of the full-thickness burn wound within the first week and coverage is now accepted as the standard of care universally. The face wound in particular incited controversy due to its aesthetic significance, vascularity, and excellent spontaneous healing.
Once the decision to excise has been made, the patient is hemodynamically optimized and consented for the procedure. Adequate blood products, homografts, skin substitutes, etc., should be prearranged. The surgery is performed under general anesthesia with the patient in a reverse Trendelenburg position. The endotracheal and feeding tubes are kept out of the field by suspending them from overhead hooks. Many methods have been devised to keep the tube out of the way and secured. The eyes can be protected with silicone pads, cornea shields, or temporary tarsorrhaphy sutures.
In large TBSA burns, facial burn wound excision can be done in multiple sittings with minimal use of autograft in each session.
Second look surgery has an important role in catching hematomas early and assessing the adequacy of excision.
In sensitive areas like ala and tip of the nose, chin, ear, etc., a delicate balance needs to be maintained between adequate excision and creating a contour deformity. Err on the side of excising less.
Treat entire aesthetic subunits even if a minor area within it is uninvolved to preserve uniformity.
In mixed depth injuries, excision should be performed to a uniform depth to avoid problems of retention of skin appendages like inclusion cysts, pits, and folliculitis.
Excision is performed with the help of a dermatome (Goulian) set to 0.008-inch thickness. This can tackle most areas except for certain areas like the medial canthal region, ears, philtral area, etc. For such areas, modalities like hydrosurgery systems (Versajet) can be used. This is a hydrosurgery system, which uses a high-pressure jet of sterile normal saline to debride wounds, drawing tissue debris and fluid into a chamber via the Venturi effect created by the normal saline jet.
Excision in the face is usually commenced with the central T-shaped area constituting the eyelids, nose, upper and lower lips, and chin. The amount of bleeding from a full face excision can be quite copious, and hemostasis has to be quick and adequate. Excisions of the face can hence be staggered to avoid heavy blood loss. Ear burns require a special mention as the instrumentation available does not allow a suitable excision of this architecturally complex structure. It can follow the traditional method of allowing an eschar to form and separate. Topical antimicrobials and moist dressings can be used to assist healing.
Starting with the lids, tarsorrhaphy stitches may be taken to protect the eyes. It is more useful to take stitches for traction at the lid margin to obtain a uniform plane for excision. The endpoint of excision is the orbicularis oculi muscle, a layer of which may also need to be excised. Punctuate bleeding is the endpoint to look out for. After excision, pads soaked in saline epinephrine solution (1 in 100,000) can be used for hemostasis. Caution has to be exerted during the use of the epinephrine, as if it is allowed to spread to neighboring tissues that are unexcised, it may interfere with the accurate determination of the endpoint due to its vasoconstricting effect. The medial canthal regions are next. This is a narrow-curved part, and hence the Versajet may be used or else excision may be performed with a number 15 scalpel blade and curved scissors in a piecemeal fashion.
The next area to be excised is the nose. The upper part of the nose being well supported by the bony and cartilaginous framework can be excised using the dermatome. However, caution has to be exerted at the ala and nasal tip where anatomic distortion can very easily occur with a deeper excision.
The upper lip and philtral region, even though lying anterior to the bony maxilla, are mobile structures that are difficult to excise. Care must be taken to excise the minimum possible tissue from the philtral region as it lends character to the appearance of the face.
The lower lip and chin are excised in a similar cautious manner. A special mention is made again, while excising the chin, to exercise restraint and save further excision for a later session rather than risk flattening the chin.
Having completed the excision of the central T area of the face, attention is shifted to the four outlying flat areas: the cheeks, forehead, and neck. These are excised in a similar manner. The dermatome can be set at 0.010- or 0.012-inch thickness. The eyebrow area is spared while excising a forehead burn.
Allograft, if available, is used initially for coverage of the excised areas. The allograft is gently removed after a week checking for adherence. The area of the face to be covered determines the donor area to be used. The scalp skin is good in terms of color match and texture for partial face excisions. In full face excisions, thick autografts are harvested from elsewhere in the body to the extent of 0.008 to 0.012 inches to improve the aesthetic appearance. The grafts are then laid on the wound bed and secured as previously described. Small darts are made in the graft margin, and small local Z-plasty flaps can be fed into the areas opened up by the darts. This breaks the margin and prevents contracture band formation.
Grafts are fixed meticulously with Vicryl, or fine Monocryl sutures. Meshing and stapling of grafts are preferably avoided.
It is not common, but when both lids have to be grafted, traction sutures can be used for the graft placement. Using tie over and bolsters, grafts can be well apposed to raw surfaces by many ingenious techniques.
In the neck, care has to be taken in the lateral aspect not to have a straight line. Instead, small darts are made in the graft margin to prevent band formation, and small local Z-plasty flaps can be fed into the areas opened up by the darts.
Dressing consists of a layer of non-adherent paraffin-impregnated gauze. This is covered by layers of absorbent gauze. Foam pads can be used to provide uniform pressure. Lastly the bubble mask or pressure garment is applied.
For the neck, in the authors’ institution an elaborate mold using plaster of Paris is made maintaining the important landmarks like the cervicomental angle. After the period of graft stabilization, the neck extension can be maintained with the help of a hard cervical collar or thermoplastic splints. Graft inspection regularly helps in catching hematomas, which can be drained through nicks in the skin. Gastric tube feeding for the initial 4 days may promote graft adherence by reducing jaw movements.
The other options for cover after excision include acellular dermi s, xenografts, MatriDerm, Integra, and cultured epithelial autografts.
Acellular dermal matrix (ADM) covered in a single stage with razor-thin autograft has been used successfully in the treatment of full- and partial-thickness burn injuries and in late reconstruction. Long-term follow-up results were good in terms of color, texture, appearance, and elasticity. Hypertrophic scarring and junctional scarring were minimal.
This is similar to allograft use in all respects and is popular in many centers, except for the fact that xenograft never adheres to the wound bed.
These collagen–elastin and collagen glucoaminoglycan type dressings have been used successfully to cover deep burns after excision. Some cited advantages of these include the ability to cover tendon and bone, good scar elasticity, and cosmesis. They do have disadvantages of cost and availability.
The use of cultured epithelial autografts in the form of cell layers and sprays has been described by various studies. A 4 × 4 cm biopsy sent at admission yields keratinocytes which are subcultured to produce a cell suspension within 8–10 days, which can be used as a spray on the wound bed. This potentially speeds up healing times, has an improved cosmesis, and reduces donor morbidity.
Ophthalmic injury with facial burns has been reported ranging from 4% to 36% of facial burns with 13% having direct corneal injury. Corneal injuries have been reported to occur more often with chemical burns and in some other reports due to flame burns.
An eyelid burn can signify underlying ocular damage and warrants a detailed ophthalmologic examination, which may include a slit-lamp microscopy, fluorescein staining, and fundoscopy. The crow’s feet area, if spared, can predict an uninjured cornea to a high degree of accuracy. The eyes should be irrigated with a balanced salt solution (BSS) and not with sterile water. The eyes are kept moist with lubricants and topical antimicrobials. In partial-thickness burns with incomplete eye closure, an early temporary lateral tarsorrhaphy can be carried out. Early excision and grafting in full-thickness burn with thick split-thickness or full-thickness grafts prevents ectropion, exposure keratitis, conjunctivitis, and corneal ulceration.
The nose is not only central on the face but also has projection. Owing to these properties it tends to be involved in a large percentage of facial burns. Both these structures have a cartilaginous framework closely covered by the skin. Deep thermal burns involving these structures would lead to exposure of cartilage or its deformities due to the inevitable chondritis that will follow their exposure. Conservative measures are equally common in these organs. Meticulous dressings which avoid pressure but conform to the loops and whorls of the ear framework will preserve its architecture and prevent abscess formation, in which event a formal incision and drainage may be required. Just as in the ear, avoidance of pressure, topical treatment, and use of splints go a long way in the reduction of nasal deformities.
Lips are prone to scab and crust formation. These must be cleaned repeatedly, and the lips should be kept moist with a petroleum jelly or liquid paraffin. Use of innovative methods and splints are essential to keep microstomia at bay. Hair-bearing regions are repeatedly trimmed to avoid scab build-up and folliculitis.
The scalp has a rich supply of blood vessels and hair follicles facilitating healing and re-epithelialization, making therapy essentially conservative.
This constitutes wound care measures like repeated cleaning of debris, shaving the region, and moist wound dressings combined with generous use of topical antimicrobials.
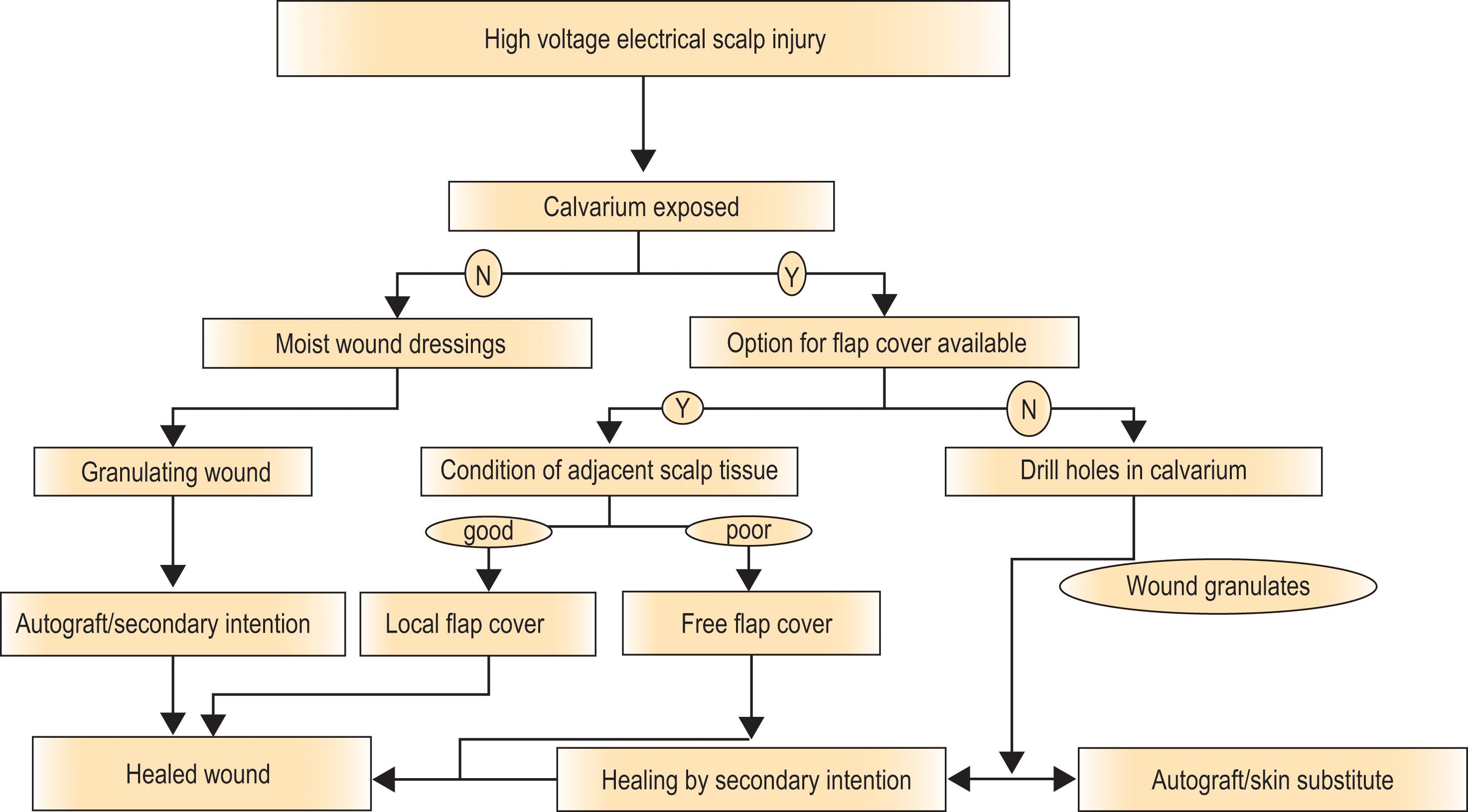
Management of deep calvarial burns ( Fig. 20.5 ) is outlined in Algorithm 20.4 .
 Full-thickness electric injury with eschar on scalp. He had a subdural hematoma which was evacuated by craniotomy at another hospital, and ten days later the patient presented to us with dead necrotic scalp and for management of burn. (B) One year postoperative after resurfacing with anterolateral thigh (ALT) flap.")
The neck is another important contiguous area that, when burnt and if neglected, can lead to development of disastrous secondary deformities. Posturing an acute burn patient can go a long way in preventing neck contractures if treated by a conservative method. The patient is made to lie with a bolster support behind the upper back, thus automatically extending the neck during the healing phase. When posturing is coupled with the use of thermoplastic splints or neck collars, neck contractures can be effectively prevented ( Fig. 20.6 ). If excision is opted for it is carried out like elsewhere on the face or body, taking care of splintage and posturing in the postoperative period also.

If, due to lack of infrastructure and advanced intensive care facilities, early excision is not feasible, a conservative approach to wound care till eschar development and separation with granulation formation is adopted. The patient is then taken up for wound debridement and coverage with split-thickness autografts. It is preferable to assess the wound microflora prior to surgery by sending regular wound swabs or, more reliably, wound biopsies to optimize graft take.
The rehabilitation of a facial burn is a continuum that begins on the day of admission, and every little done during the treatment and early healing phase goes a long way in the final appearance of the scars and facial aesthetics. Scarring is inevitable in burn wounds that take longer than 2 weeks to heal. The therapist and the surgeon have to work in close coordination in this phase to evaluate the patient in terms of goals of rehabilitation, areas needing special care, areas at risk of developing scar hypertrophy, or contractures.
Daily facial mobilization exercises along with special care paid to the eyelids, lips, and oral commissures prevent ectropion and microstomia formation, respectively. Exaggerating the action of facial muscles helps stretch the overlying skin and scars to improve their pliability.
Use of splints has been long advocated and is gaining popularity with the availability of newer technology and materials which can be serially molded and altered in shape. The use of oral splints in preventing microstomia formation and nasal silicone splints to prevent nostril stenosis cannot be overemphasized. In ear burns, use of splints serves to maintain the postauricular sulcus and preserve the overall cartilage architecture.
Most commonly used ancillary modalities include scar moisturization and massage therapy, compression garment use, topical silicone use in the form of liquid or sheets, total contact face mask use, and sunscreen use to avoid pigmentary problems.
Moisturization using a lubricant serves to make the scar or grafted skin more pliable, soft, and prevents ulcerations and scar breakdown. The scar massage done at the time of moisturizing helps in the scar maturation and fading even though evidence suggests a greater benefit in postsurgical rather than post-burn scars.
Pressure therapy , i.e., use of pressure garments at a recommended pressure of 15–20 mmHg, has been widely described and used in post-burn scars. It has come to be accepted as the standard of care for post-burn scar management. Most regimens remain empiric about the pressure and duration of use and are based on directives created by experienced surgeons. The patient is instructed to wear the garment, which is custom fit, for 23 hours a day and for at least 6–12 months ( Fig. 20.7 ). The pressure is claimed to improve thinning and pliability by 60% to 85%.

Silicone sheets have been used to soften scars, increase their pliability, change the color and texture, and reduce contracture formation by the property of occlusion and improving the hydration of the stratum corneum layer.
Total contact face masks have been developed using 3D printing technology and can be made of hydrogel polymers or silicone. These are transparent, conform to the exact facial contours of the patient and can be worn continuously to help exert pressure during the scar remodeling phase to improve scar thickness and pliability.
Despite the best of measures, the patient may develop hypertrophic scarring and contractures for which secondary reconstructive procedures may be required.
An acute facial burn is a psychologically distressing injury as this leads to alteration in perception of image and reduces the self-confidence. Acceptance in society for the facially disfigured is poor in most countries, and they have to settle for non-contact jobs. Studies have shown a difference between caretaker- and patient-perceived quality-of-life indicators. This suggests that sensitivity to patient-perceived post-trauma psychological issues have to be borne in mind by the parent or caregivers and treatment instituted early. Recent studies also indicate a positive influence of education on the overall psychological well-being of patients irrespective of their gender.
Psychosocial rehabilitation begins with a clear understanding of the patient’s preinjury psychiatric history. History of past illness, substance abuse, poor family support system, etc., predispose to requirement of psychotherapeutic interventions right from the acute burn stage.
Interventions may be needed in the acute phase, early post-recovery phase, and in the delayed recovery or chronic phase.
In the acute phase, intervention could be in the form of providing information to the patient regarding the stages of care, expected outcomes and addressing patient concerns and expectations. This has been shown by studies to allay patient anxiety and fears. Involvement of the family in the patient care and supportive psychotherapy in the form of positive coping strategies (distraction, imagery, etc.) can improve mood and reduce post-traumatic stress.
In the delayed acute phase or early rehabilitation phase, cognitive behavior therapy and supportive psychotherapy (grief counseling, addressing anxiety, and depression) are seen to be helpful.
In the chronic phase, support groups can play a pivotal role in social reintegration of the burn survivor. Regular counseling with empathy and enrollment in burn camps and survivor groups should become an essential part of psychological rehabilitation. The burn camp concept, which is well accepted and popular in the West, is now slowly being embraced by the Middle Eastern and Asian burn units. The authors’ institution has been conducting the only pediatric burn survivor camp of India, and the camp has been found to be an uplifting experience for the doctors and campers alike. In low- and middle-income countries (LMICs) often these patients are neglected and abandoned by their families, and they need legal and vocational support as well. The management of the scars should not be limited to the physical element alone, as the psychological aspect of care completes the circle of treatment for both the patient and the treating surgeon.
Scarring is an inevitable eventuality in the healing process. Scarring is dynamic and behaves as a continuum rather than as an endpoint due to the many factors at play that constantly alter the scar biology. As described in the previous segment, a post-burn scar requires a lot of early rehabilitative measures, which are now accepted as the standard of care. When an attempt at scar amelioration through these efforts cannot be made due to patient factors or poor follow-up by the burn unit, the incidence of scar morbidity in the form of hypertrophic scarring, keloid formation, and contractures rises. However, the tendency to excessive scarring may also depend on a number of other factors ( Table 20.1 ).
| Criteria | Factors that contribute to scarring | Less scarring |
|---|---|---|
| Sex | Males | Females |
| Race | Non-White | White |
| Healing time | >21 days | <10 days |
| Method of management in acute phase in full-thickness burn | Conservative or no treatment | Early excision and use of dermal substitute |
| Management after healing | No use of ancillary scar management methods | Early use and continuation of ancillary scar management methods |
Post healing, the patient may present to the burn surgeon for restoration of function or for non-functional reasons (aesthetic, pain, itching, or infective problems) or a combination of these reasons. Functional problems are more often than not due to contractures (for example, neck contracture) or distortion of vital parts like eyelid ectropion causing corneal ulceration. Non-functional issues could be related to quality of skin, pigmentation issues, loss of tissue, etc. The reasons are myriad and are enumerated in Table 20.2 .
| Functional reasons | Non-functional reasons | |
|---|---|---|
| Aesthetic | Infection | |
|
|
|
Facial burn survivors deserve a higher level of empathy from the surgeon compared to those who have burns sparing the face. The approach to these patients who come with expectations like “can these scars be removed?” has to be a realistic one. It has to be made clear to the patient and caregivers at the first consultation by explaining the process of healing and scarring, that skin once scarred cannot be made unblemished again despite the array of procedures at our disposal.
Restoration of function and aesthetic appearance in facial burns may require a number of procedures. The surgeon needs to be able to play out the entire sequence of procedures mentally leading toward the final outcome. The plan needs to be made after detailed discussion with the patient so that they have a shared vision of the final outcome. During the preliminary consultation, a detailed history should be elicited from the patient. All details of the earlier management should be asked for, like details of early or delayed surgery, donor site usage, early rehabilitation in terms of use of pressure garments, splints, positioning, and silicone sheets. Non-compliance to ancillary measures helps to red flag the patient as one who would need extra counseling and repeated reiteration of the benefits of these measures. In the outpatient clinic, the authors have often found it worthwhile introducing one patient to another showing how the other patient has benefited from being compliant to the post-healing care regimes. It is also beneficial to have photographs of patients (taken with informed consent) who have undergone reconstructive procedures, which may help illustrate some points to the new patient who may be unable to visualize how a flap or graft may appear. The consultation is concluded in a positive spirit, reiterating that the surgeon and patient would work together toward a common goal, i.e., good functionality with an adequate but realistic aim of aesthetics.
The final outcome of the patient is only as good as the overall plan. The patient may present with multiple contractures or scarring in many parts of the body. An overall plan has to be made keeping the entire body in perspective. When we see the patient as a whole, a note can be made of the available donor areas for skin grafts, flaps, or tissue expander placement.
The sequence of correction of the deformities with the interval between each procedure should be pinned down after discussing with the patient. This is especially true for patients who present with multiple contractures ( Fig. 20.8 ). For a patient who presents with bilateral hand, elbow, axillary, as well as neck contractures, the sequence can be as follows: first stage – release of neck contracture with dominant hand or worse hand and elbow release; second stage – opposite axilla + hand release; third stage – elbow of non-dominant side; fourth stage – axilla of dominant side. These decisions are based on many factors like present function of each hand, handedness, occupation, patient desires, etc. The fact that it is paramount to release the neck contracture first is not debatable.

Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here