Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Any lesion in the lower extremity with a clinical history of pain, continuous growth, size over 5 cm, or deep subfascial localization is suspicious of a sarcomatous malignancy and should be surgically biopsied according to established surgical rules.
Still the single statistically proven modality of curing sarcomas and prolonging postsurgical lifespan is surgical excision with wide margins resulting in a postoperative R 0 -status. To date, no other neoadjuvant or postoperative treatment modality can replace this approach. If wide margins cannot be achieved, adjuvant therapy is indicated for extremity preservation.
Plastic surgical lower extremity sarcoma reconstruction is – especially in bone sarcoma reconstruction – the classical field of an interdisciplinary, multimodal approach, most commonly working together with tumor and orthopedic surgeons, oncologic radiotherapists, oncologists and radiologists.
Modern oncoplastic reconstructive surgery can provide adequate reconstructive options for almost any defect size and composition, and so radical tumor excision can be combined with over 95% extremity preservation today.
The plastic reconstructions in sarcoma-related limb-sparing surgery (LSS) are often demanding and complex and consist of the full spectrum of plastic surgical options. They should be performed in specialized centers and specifically adapted to the patient and case profile.
 Access video content for this chapter online at Elsevier eBooks+
Access video content for this chapter online at Elsevier eBooks+
Soft-tissue tumors are a highly heterogeneous group of about 100 different tumor entities, which are still classified histogenetically according to the main adult tissue component they resemble most. The malignant subgroup among them is called sarcomas, which not only have the potential to grow locally invasive or even demonstrate destructive growth but also have a variable risk of recurrence and metastatic potential. As the term “ sarcoma ” (derived from the Greek word σαρξ “sarx” = “meat”) itself does not necessarily imply fast, expansive growth or metastasis, a further subclassification system into more aggressive sarcomas (high-grade, poorly differentiated) or less aggressive (low-grade, well differentiated) types does exist. Some lesions like the atypical fibroxanthoma are called “pseudosarcomas”, as they demonstrate a benign clinical course but are histologically malignant. However, usually well-differentiated tumors show low-grade characteristics and vice versa .
Primary bone sarcomas are even less frequent than soft-tissue sarcomas, and most malignant osseous lesions are metastatic, especially in advanced age. Despite having a low incidence, bone sarcomas have a high significance for both patient and surgeon due to their impact on extremity function and overall mobility. Limb-preserving surgery after wide tumor resections frequently poses a real challenge for the reconstructive surgeon.
Sarcomas can occur in every part of the body, as they derive from mesodermic tissue such as muscle, nerve, bone cartilage, blood vessels, or fat. The therapeutic mainstay for soft-tissue sarcomas is based on surgical excision. However, previous radical concepts in STS surgery have been gradually replaced by more moderate approaches with function and limb-sparing resections combined with radiotherapy, chemotherapy, and/or isolated limb perfusion. The complexity of the surgical resection and the subsequent plastic surgical reconstruction differs considerably depending on the localization.
Like any oncologic discipline, sarcoma treatment is a typical field of modern interdisciplinary and multimodal therapy. Lower extremity sarcoma reconstruction is – especially in bone sarcoma reconstruction – also a fascinating field for an effective interaction between the surgical disciplines of radiologists, orthopedic, oncologic, pediatric, and podiatric surgeons and plastic reconstructive (micro-)surgeons.
Modern plastic reconstructive surgery can provide adequate reconstructive options for almost any defect size and composition, so considerations about defect size should not play a role during tumor excision. Today, over 95% of the extremities can be preserved after radical tumor excision, and to close large defects and to largely preserve function of the extremity by transplantation of muscles, tendons, and bones as well as transplantations of nerves and blood vessels. The plastic reconstructive procedures are often demanding and complex and frequently encompass the full spectrum of plastic surgical options. These procedures may be best performed in specialized centers where regimens individually adapted to patient and case profiles may be optimized.
Sarcomas in the lower extremity are more common than in the upper limb (74% vs. 26%) and represent the most common location of sarcomas in the body overall (45%). Currently, they are safely treatable by extremity preservation in most cases, if properly performed according to the rules described in this chapter and in the pertinent current literature. In this context, several studies have now demonstrated that limb-sparing surgery (LSS) is oncologically not inferior to amputation in the treatment of lower extremity sarcoma. While amputation was still the keystone of previous surgical therapy several decades ago, it usually represents only an important last line therapeutic modality today. The common misconceptions that amputations have a better outcome both in tumor safety and quality of life have both definitely been proven wrong.
Sarcomas are rare, and a “soft-tissue swelling” is often misinterpreted by both patient and physician because of this fact. This can considerably delay proper diagnosis. Still, tumor manifestations in the extremities are often detected a bit earlier than in the trunk, as the extremities are constantly under personal “visual” control in daily life. This might be even truer for tumors on the upper extremity than on the lower.
Due to the highly functional anatomy of our extremities with vessels, nerves, tendons, bones, and muscles in the close vicinity, even smaller tumors can represent a challenge to both the resecting tumor surgeon as well as the reconstructive plastic surgeon. Preservation of the lower extremity in sarcoma reconstruction differs from alike manifestations in the upper extremity in several key points that have to be considered carefully:
Stability and weight-bearing capability are usually regarded higher than functional mobility or range of motion in the lower extremity.
Postoperative appearance is usually less important. In most urban cultures the reconstructed legs with their scars and possible voluminous flaps can easily be hidden in clothing and have a less important role in social interaction than the upper extremity (i.e., handshaking).
Weight-bearing demands are higher and atherosclerotic vessel damage and orthostatic venous pressure are more profound in the lower extremity. Both may play a major role in free tissue transfer.
Nerve regeneration is less successful in the lower extremity at any age.
Wound healing is slower, and the risk for an infectious complication is higher.
Soft-tissue sarcomas are a rare disease entity with an incidence range from 1.8 to 5:100,000 in adults and 10%–15% in children. The estimated new cases and deaths in the USA in 2021 are 13,460 and 5350 cases, respectively ( www.seer.cancer.gov ). There is no overall significant gender predisposition. The median age at diagnosis is 60 years old, with two incidence peaks, at 50 and 80 years old; 25% of diagnostic sarcomas are more than 75 years.
With about 45% of all sarcomas occurring in the lower extremity, 15% in the upper extremity, 10% in the head and neck region, 15% in the retroperitoneal space, and the remaining 15% in the abdomen and the chest wall, the musculoskeletal system of the extremities and the abdominal and thoracic walls are the most common predilection sites. Extremity sarcomas are most common in the thigh (50%–60%).
While most cases of soft-tissue sarcomas are sporadic, there are some genetic and non-genetic risk factors summarized in Table 4.1 . Up to 60% of all soft-tissue sarcomas contain a somatic mutation of p53. A detailed description of the various risk factors is beyond the scope of this chapter, but there are several strong associations to be mentioned: a history of radiation exposure accounts for up to 5.5% of all sarcomas. The risk is dose dependent, and the latency period between radiation and clinical tumor manifestation is around 5 years. Over 80% of radiation-associated sarcomas are high-grade types. Neurofibromatosis type NF-1 is strongly associated with the cumulative lifetime risk of up to 13% for the occurrence of malignant peripheral nerve sheath tumors (MPNST).
| Genetic | Neurofibromatosis NF-1 (von Recklinghausen disease) |
| Retinoblastoma | |
| Gardner syndrome | |
| Werner syndrome | |
| Bloom syndrome | |
| Fumarate hydratase leiomyosarcoma syndrome | |
| Diamond–Blackfan anemia | |
| Mechanical | Li–Fraumeni syndrome |
| Postparturition | |
| Chemical | Chronic irritation |
| Polyvinylchloride (PVC) | |
| Hemochromatosis | |
| Dioxin (TCDD) “Agent Orange” | |
| Radiation | Arsenic |
| Traumatic–accidental | |
| Lymphedema | Post-therapeutic |
| Parasitic (filariasis) | |
| Iatrogenic | |
| Stewart–Treves syndrome | |
| Infectious (viral) | Congenital |
| Kaposi sarcoma (HHV-8) |
The sarcoma subtype is determined by light and electron microscopy, immunohistochemistry, and cytogenetic analysis. If it results in a tumor that cannot be designated accordingly, a descriptive evaluation is given for an “unclassified sarcoma”. Obtaining reference pathologies for soft- and bone-tissue sarcomas should be standard, as the rate of diagnostic agreement among specialists is below 75%. The most common histopathologic subtype distribution in extremities in the largest series in the literature is shown in Fig. 4.1 .

About 2600 new primary bone sarcomas occur each year in the USA ( www.seer.cancer.gov ). The overall median age at diagnosis is 39 years. Many predisposing factors for bone sarcomas are similar to those for soft-tissue sarcomas (like retinoblastoma, Li–Fraumeni syndrome, radiation, and others) ( Table 4.1 ). Paget disease, bone infarction, and fibrous dysplasia may also represent risk factors for bone sarcomas.
The most common type is the osteogenic sarcoma, which has a predilection for the metaphyses around the knee in about 50% of cases. It is the third most common cancer in the young ( www.nhs.uk ) with a second peak around age 60. The male to female ratio is almost 2:1 in large studies, and for this specific tumor the median age at diagnosis is 17 years. Only 6.4% present initially with pathologic fractures, whereas the majority are detected in the workup of a painful mass or swollen extremity. It commonly arises in the medulla, but as a juxtacortical osteogenic sarcoma it arises from the external surface – most commonly the posterior aspect of the femur.
The spindle cell mesenchymal sarcoma group contains chondrosarcomas, intraosseous malignant fibrous histiocytomas (MFHs), and fibrosarcomas. The tumors of this group only have an incidence of about two-thirds of the incidence of osteogenic sarcomas and primarily occur in an older population. Chondrosarcomas are slow growing and relatively resistant to adjuvant therapy.
Ewing sarcoma is classically located in the femur diaphysis in teenagers, and only 20% occur in middle-aged adults. If found extradiaphyseal, it is very common in the pelvis. It is the most common primary bone malignancy of the fibula. The Ewing sarcoma is very sensitive for radiation therapy.
Sarcomas in the extremity may spread locally by continuous expanding growth irrespective of anatomic borders. In many cases it mistakenly seems that the tumor has developed a bordering capsule to surrounding “healthy tissue”. However, this capsule is part of the tumor, and soft-tissue satellite-like or intraosseous skip-lesion tumor manifestations are beyond this capsule. This fact represents the main justification for a modern wide resection concept in sarcoma surgery.
Hematogenic spread is most common in soft-tissue and bone sarcomas. For lower extremity tumors, the primary site for metastasis is the lung. Lymphatic metastases are present in less than 5% of all soft-tissue sarcomas (rhabdomyosarcoma, angiosarcoma, and epithelioid-like sarcoma).
A detailed history and physical examination is the first initial and very important step to professional tumor surgery. In sarcomatous lesions, the patient often relates the tumor causally to an – often minor – traumatic event, bringing the lesion into clinical attention to the patient. Acute trauma, however, is not a proven predisposing factor for sarcoma development. Because of this, there is often a considerable time lag between this initial recognition and the first presentation of the lesion to a medical professional. Furthermore, the rationale of the lesion is often erratically misinterpreted and then causes a variety of inadequate treatments by both lays and physicians, further delaying proper diagnosis. The average duration of any symptoms before seeing a physician is 6 months in all soft-tissue sarcomas, but possibly shorter in extremity manifestation. So in adults, lesions that (1) have not disappeared after 4 weeks, (2) are located subfascially or in the popliteal or groin flexion creases, (3) continue to grow or are symptomatic (i.e., pain and paresthesias), or (4) are already larger than 5 cm on detection should generally be biopsied as they are highly suspicious for malignancy.
It is not unusual that sarcomas are found by physicians in the context of a workup for a completely different medical problem (i.e., chronic venous insufficiency in the leg). Coincidental findings like articular pain and joint effusions are common especially with osseous sarcomas, whereas clinically manifest neurovascular symptoms are relatively rare at initial presentation. Two-thirds of sarcoma patients present with a painless mass during their first clinical examination, and only one-third have current pain or have had a history of pain in the affected region.
The thorough physical examination is not only focused on the affected extremity but includes the complete body. The pertaining lymph node stations should be examined as well, even though lymphatic spread is uncommon in the majority of all sarcoma types. The general health status should be assessed and optimized by all relevant medical specialties. This is especially important in multimorbid patients with concomitant acute and chronic comorbidities in the context of the planned operative procedures. Terminal illnesses and comorbidities have to be taken into consideration for the extent of both resection and reconstructive surgery.
Clinical assessment and staging of the patient must be completed by adequate imaging diagnostics for evaluating local and generalized tumor manifestations. Any imaging of the tumor region must be performed before any surgical biopsy as the latter may confound the picture to a considerable extent.
Gadolinium contrast-enhanced magnetic resonance imaging (MRI) is currently the diagnostic mainstay to define exact tumor location, its relation to neighboring neurovascular structures and muscular compartments, to determine its homogeneity, integrity, and vascularization, and its presumed main tissue component. MRI is specifically useful for detecting skip lesions. It allows 3D planning of the resection and helps to assess the necessary reconstruction procedures preoperatively.
Modern spiral computerized tomography (CT) scans are indispensable for clarifying the detailed anatomy of osseous sarcomas, determining the extent to which skeletal structures are affected by neighboring soft-tissue tumors, and aiding in operative planning of these sarcomatous entities. Thoracic and abdominal CT scans are the diagnostics of choice for staging of high-grade sarcomas of the extremities and detect intrapulmonary and abdominal metastases. In recurrent disease, positron emission tomography (PET) CT can augment the information about suspicious lesions in selected cases, though not accepted as a standard instrument for the preoperative workup (see Chapter 7 ).
CT angiography with 3D reconstructions is a valuable tool in determining the overall vascular status of the affected leg, the underlying generalized vessel disease, and the vascularity of the tumor, and showing vascular displacements, collateral perfusion systems, vessel invasion, and tumor-related occlusion. They also provide valuable information about the feasibility of microvascular anastomoses and the presence of suitable recipient vessels, especially in elderly patients.
Plain X-ray films demonstrate specific periosteal or cortical signs, osteolysis, and paraosseous calcifications in diaphyseal and metaphyseal bony lesions. Even today, a plain radiograph remains the diagnostic method of choice for primary bone sarcomas ( Fig. 4.2 ). A plain chest radiograph is still considered the standard for clinical staging in low-grade extremity lesions.

Ultrasound with or without contrast media is a cheap, fast, and painless adjunctive diagnostic measure that may be especially helpful in highly vascularized tumors. Ultrasound was often the diagnostic device of coincidental tumor findings but is also used for getting an initial overall picture of the lesion.
A 99m-Tc-pyrophosphate bone scan is essential to bone tumor staging and screening for multicentric disease or metastases.
A special laboratory workup for soft-tissue sarcomas does not exist, whereas elevated alkaline phosphatase and lactate dehydrogenase over 400 U/L are independent predictors of an unfavorable outcome in bone sarcomas.
The term sarcoma was first used by Abernethy in 1804 and was based on the gross characteristic of the tumors. Codman founded the first Bone and Soft Tissue Sarcoma Registry in 1909, containing information on the diagnosis and treatment of bone. In 1829 Jean Cruveilhier published a two-volume work on pathologic anatomy, containing a substantial amount of information about sarcomas as they are understood today.
Since then, the classical treatment of a sarcoma in the lower extremity was amputation, accounting for relatively low recurrence rates, but with a severe impact on the integrity of the patient. In 1879 Samuel W. Gross published his experiences with 165 sarcoma cases of the long bones, in which he advocated early amputation despite the prevailing operative mortality rate of 30%. Based on his study, limb-salvaging resection inevitably led to local recurrence, metastasis, and death. Following this study, an even more aggressive approach to bone tumors was popularized, but survival rates did not improve significantly. This stimulated the first adjuvant radiation treatment of bone tumors.
However, the mortality rate of radiated patients equaled the mortality rate of patients who underwent amputation. The first neoadjuvant protocol was developed in 1940 by Cade and Ferguson, who combined preoperative radiation followed by amputation 6 months later in metastasis-free patients. The aim of the protocol was to avoid unnecessary amputation.
The transition between amputation surgery and limb-sparing surgery was less of a plastic surgical issue than an oncologic–orthopedic development: reconstructive procedures after sarcoma resection were very uncommon until the number of limb-preserving resections increased.
Episodic anecdotes reporting on limb salvage appear as early as 1895, when Mikulicz described two resection arthrodeses of the knee for distal femoral lesions in Europe. Sauerbruch in Germany described his “Umkippplastik” in 1922 as the precursor of today’s rotationplasty. A first systematic approach to limb salvage was suggested in 1940 by Phemister in his article “Conservative Bone Surgery in the Treatment of Bone Tumors”.
After WWII more surgeons began to explore limb-salvaging resection instead of amputation. It became clear that obtaining adequate surgical margins is a key issue for cases with resectable tumors according to their pathologic characteristics. Their work established the principles of today’s limb-salvaging surgery despite the limited reconstructive modalities at that time.
The surgical treatment of malignant bone tumors was revolutionized in the early 1970s by the development of chemotherapy, improved diagnostic radiology by more accurate CT and MRI scanners, advances in reconstructive surgery, improvements in orthopedic oncologic surgery, and, eventually, the establishment of multidisciplinary tumor centers. These advances are mainly responsible for the reduction in local recurrences after limb-salvaging procedures by allowing a better patient selection and a more accurate preoperative planning.
During these developments, many sophisticated plastic surgical techniques were developed in a fascinating history that is covered in a different volume of this textbook. Most of the techniques were focused on soft-tissue reconstruction, but later composite tissue transplants and grafts were improved as well. Many new techniques were derived from trauma surgery, the treatment of congenital disorders, or tumor surgery elsewhere in the body and did not specifically relate to the development of sarcoma surgery, but were quickly adapted to limb-preserving tumor reconstruction. Sophisticated pedicled reconstructive methods like cross-leg flaps, tubed pedicled flaps, or fibula pro tibia transfers were standard procedures in early LSS until reconstructive microvascular surgery was integrated into the plastic surgical armamentarium.
Modern reconstructive approaches integrate the latest advances in orthopedic surgery, such as modular and custom-made tumor prostheses for long bone and joint replacement, with the full spectrum of the plastic surgical reconstructive ladder or elevator including chimeric multi-tissue-type free flaps in limb-sparing lower extremity sarcoma reconstruction.
The goals of surgery in sarcoma reconstruction in the lower extremity depend on the individual case profile, which is composed of personal factors and the available reconstructive options. The most important personal factors that need to be taken into consideration are age, size, and weight; concomitant chronic diseases relevant to general health and operability; medications; social status; functional and aesthetic conceptions; previous operations; and tissue quality of the affected extremity.
The pertinent reconstructive options that need to be discussed with the patient are the relevant operative methods according to the applicable steps of the reconstructive ladder, counterweighing their advantages and disadvantages for the actual tumor stage, location, oncologic safety, and potential adjuvant procedures (i.e., irradiation).
Above all, the prime goal should be an R 0 -resection with tumor-free and adequately wide margins, which provides the best chance of complete surgical cure of the disease. This might create a considerable surgical defect and can imply major surgical reconstructive procedures for the patient. The extent of adequate wide tissue resection is almost never realized by the patient presenting with a palpable mass and has to be explained to him or her in detail.
If surgical cure is not possible, resection of as much tumor mass as possible (tumor debulking) is paramount (R 1 /R 2 ) and usually followed by adjuvant radio- and (less frequently) chemotherapy according to the recommendations of a multidisciplinary tumor board. At this point, the reconstructive goal should aim for a functional lower extremity capable of full weight-bearing that appears as aesthetically pleasing as possible in the given case and circumstances. The surgical therapy should create a status for the patient to be integrated in social life, allowing him or her to wear normal clothing and having a closed skin envelope. In selected cases, creating a stable open chronic wound is the only remaining palliative option; however, it should be free of copious discharge and secretions and avoid any olfactory nuisances. For example, a stable open wound producing minimal drainage that can be treated by daily dressing changes at home may offer a higher quality of life than performing another resection and reconstructive effort that may force the patient to stay in the clinic during his or her last days.
Each case should be discussed in the multidisciplinary tumor board with all relevant medical disciplines involved in the setup of a treatment plan (tumor surgeon, medical oncologist, orthopedic surgeon, plastic surgeon, internal medicine, psychologist, radiologist, oncologic radiotherapy specialist, prosthetic technician, etc.). For optimal planning and strategy development, all diagnostic procedures, the radiologic imaging, and the definitive histology should already be present (see below). Even during the worst pandemic period of SARS-CoV-2, some sarcoma centers were able to implement pathways and structures to keep this important multidisciplinary approach.
A thorough and complete discussion of the tumor board treatment recommendations are explained to and discussed with the patient including all operative options (including amputation) and neoadjuvant or adjuvant chemo- or radiotherapy. It is important for many patients to have an outline of the timeframe for the various surgical or multimodal therapeutic options.
Finally, tumor staging is done according to the current staging systems for soft-tissue sarcomas. The American Joint Committee on Cancer (AJCC) eighth edition system is designed for extremity sarcomas, including most but not all histologic subtypes. The major changes in the eighth edition of the AJCC staging for bone and soft-tissue sarcomas are the following four points:
Tumors are described separately according to the primary sites. For bone sarcoma, three tumor locations are described: (a) appendicular skeleton, trunk, skull and facial bones; (b) spine; and (c) pelvis. Meanwhile, four tumor locations are described for soft-tissue sarcoma: (1) trunk and extremity; (2) retroperitoneum; (3) head and neck; and (4) visceral sites.
Histologic grading system in bone sarcoma is changed to three-grade classifications.
For soft-tissue sarcoma, any TN1M0 tumor in the trunk and extremity is classified as stage IV, whereas for the retroperitoneal tumor, any TN1M0 remains as stage IIIB.
For soft-tissue sarcomas in the trunk, extremity, and retroperitoneum, tumor size was classified into four categories: (a) ≤5 cm; (b) >5 cm and ≤10 cm; (c) >10 cm and ≤15 cm and (d) >15 cm. In addition, the notation about the depth of the tumor (superficial or deep from the superficial fascia) has been eliminated. Dermatofibrosarcoma protuberans (DFSP) and angiosarcoma, among others, are exempt from staging with the AJCC.
For primary bone sarcomas like the osteogenic sarcoma, the Musculoskeletal Tumor Society (MSTS) ( Table 4.2 ) staging system is used. This classification was established in 1980 by Enneking. For bone sarcomas, orthopedic surgeons frequently refer to the MSTS system for bone tumors, and it is still the primary staging system taught in many training programs despite major evidence-based updates to the AJCC system, including demarcations based on the tumor size, anatomic site of a primary tumor, and location of metastases.
| Stage | Characteristic |
|---|---|
| IA | Low-grade, intracompartmental |
| IB | Low-grade, extracompartmental |
| IIA | High-grade, intracompartmental |
| IIB | High-grade, extracompartmental |
| IIIA | Low- or high-grade, intracompartmental with metastases |
| IIIB | Low- or high-grade, extracompartmental with metastases |
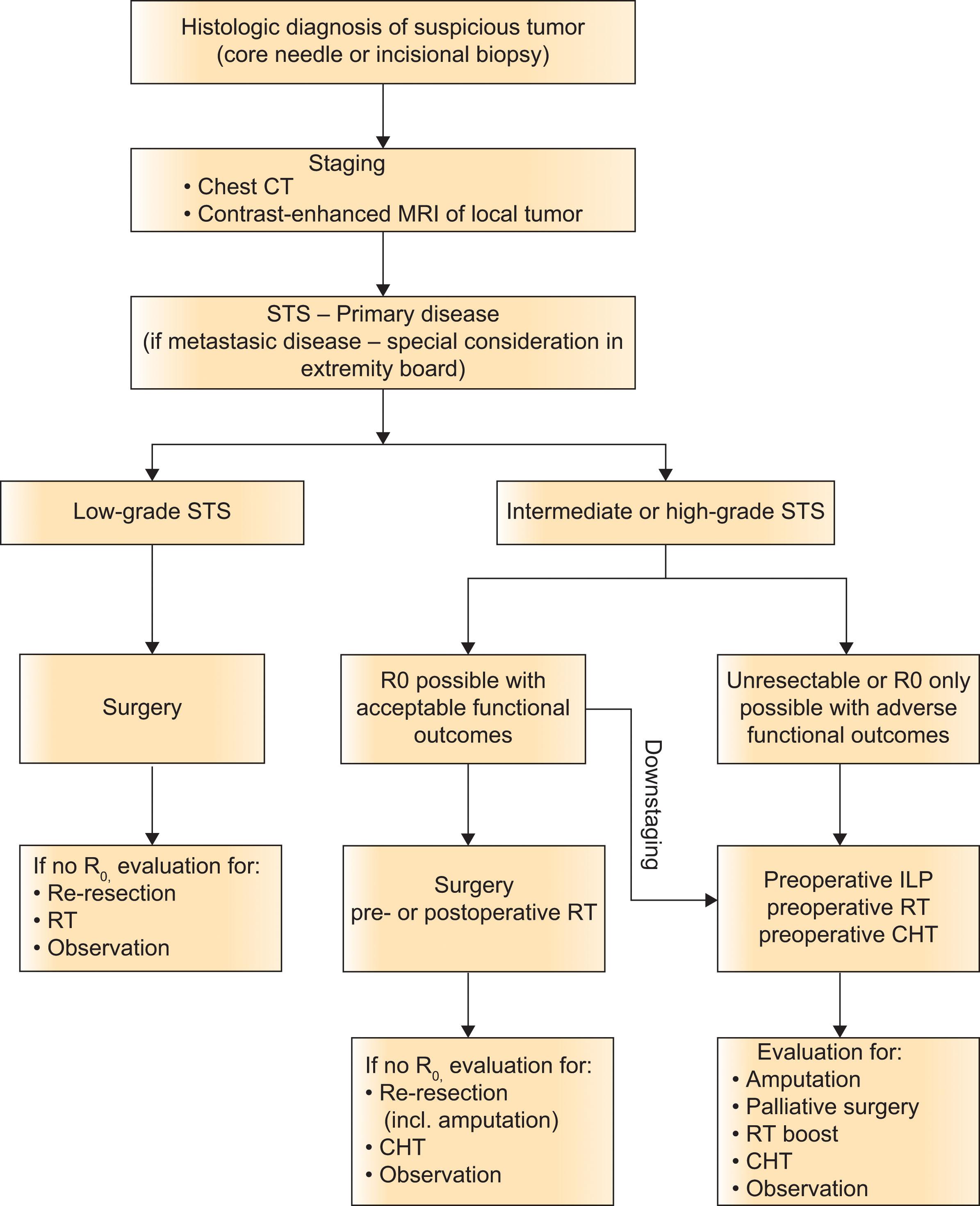
If complete tumor resection is possible (R 0 ) with acceptable functional outcome, no other treatment modality provides better cure for sarcomas than adequate surgery. Oncologic safety is paramount, but preservation of the leg or foot should be achieved to preserve patient integrity, which is usually possible. Isolated limb perfusion, chemotherapy, or radiotherapy should be preoperatively considered if complete tumor resection is not possible (R 1 ) or if R 0 is only possible with adverse functional outcomes. This could avoid the need for prosthesis adaptation and use and prosthesis-related problems.
Several considerations in sarcoma-related defect reconstruction need to be mentioned that differ from sarcoma-related surgery at the upper extremity. The capability for stable weight-bearing is more important than joint mobility in the lower extremity, whereas preservation or restoration of sensitivity is less important on the leg and foot than on the arm or hand. While sensitivity should be preserved as much as possible, in selective cases, asensitive “stilt-legs” are considered superior to amputations, especially in elderly patients that would have problems adapting to prosthesis handling. Not being able to preserve the main nerves and thereby sensitivity is not an indication for amputation by itself!
Radiotherapy is the primary adjunctive treatment method in sarcoma management today. Neoadjuvant radiation in large sarcomas uses external beam irradiation that helps in tumor shrinkage and thickening of the tumor capsule, which facilitates adequate resection and the achievement of negative margins during wide resection and reduces potential surgical tumor seeding. The disadvantages of preoperative irradiation are a higher rate of wound healing complications compared to postoperative radiotherapy and the creation of necrotic tumor material for the pathologist. However, preoperative radiotherapy did not increase the risk of acute wound or microvascular complications when combined with free flap reconstruction, and was associated with fewer late recipient-site complications than adjuvant irradiation.
The European Society for Medical Oncology (ESMO) recommendation favors adjuvant radiotherapy when tumor size is above 5 cm or deeply located or high grade and when R 1 resection occurs. In the context of neoadjuvant radiotherapy, NBTXR3 is a new class of radioenhancer and shows efficiency in localized sarcoma in a phase 1–2 study. NBTXR3 follows by radiotherapy improved responses rate, with correct tolerance in comparison with radiotherapy alone.
Intraoperative radiation comprises a single dose electron radiation and has indications for use in the lower extremity for locations around the groin and foot. It is especially effective when the tumor dose is increased relative to the normal tissue dose. However, its availability is limited even in modern tumor centers.
Postoperative irradiation is done with brachytherapy and electron beam therapy both used in solitary and combination regimens. Brachytherapy is especially useful after resection of local recurrences in a previously irradiated field.
To date, any adjuvant or neoadjuvant chemotherapy for sarcomas should only be conducted in clinical studies (EORTC, COSS, EURO-Ewing, etc.). The role of perioperative chemotherapy remains controversial in both neoadjuvant and adjuvant settings. Adjuvant chemotherapy can be proposed as an option to the high-risk individual patient for a shared decision-making with the patient. Analysis by subgroups in meta-analysis revealed benefit preferentially to the soft-tissue mass located in extremities and chest wall. If the decision is made to use chemotherapy as upfront treatment, it may well be used preoperatively. A local benefit may be gained, facilitating surgery, in addition to the systemic one. Neoadjuvant chemotherapy with anthracyclines plus ifosfamide for at least three cycles can be viewed as an option in the high-risk individual patient.
The various protocols are beyond the scope of this chapter and are changing rapidly. The reader is therefore advised to consult the pertinent most recent literature on that matter.
Isolated limb perfusion (ILP) can be proposed in selected locally advanced marginally resectable soft-tissue sarcoma of extremity. A meta-analysis for isolated limb perfusion of extremity soft-tissue sarcoma demonstrated overall response rate of 73.3% and complete response rate of 25.8%. The procedure mainly involves a 60 min perfusion with melphalan and TNF-α under mild hyperthermia, achieving a limb preservation rate of 72%–96%, with an overall response rates from 72% to 82.5% and an acceptable toxicity according to the Wieberdink scale. The local failure rate is 27% after a median follow up of 14–31 months compared to 40% of distant recurrences after a follow-up of 12–22 months. Currently there is no consensus regarding the benefit of ILP per histotype, and the value of addition of radiotherapy or systemic treatment.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here