Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Femoral neck fracture—minimally displaced.
Femoral neck fracture—inadequate assessment of the lateral radiograph.
Pubic ramus fracture.
Apophyseal injuries in the young.
AP of whole pelvis.
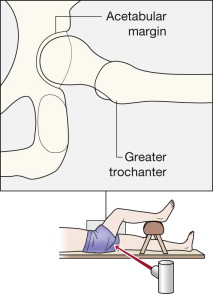
Lateral projection of the painful hip.
AIIS, anterior inferior iliac spine;
ASIS, anterior superior iliac spine;
CT, computed tomography;
MRI, magnetic resonance imaging;
RTA, road traffic accident;
THR, total hip replacement.
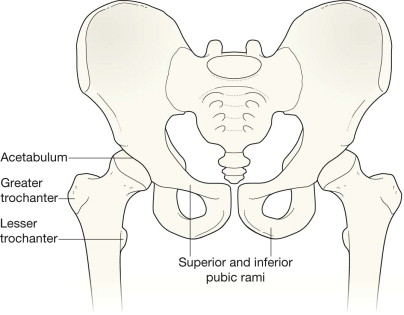
The femoral neck should:
Have a smooth and intact cortex—no buckle, no step, no ridge.
Not show any transverse areas of sclerosis.
The intertrochanteric region should:
Have an appearance identical to the same area on the opposite femur.
Not show any black or lucent line crossing the intertrochanteric bone nor any interruption in the cortical margin of the greater trochanter.
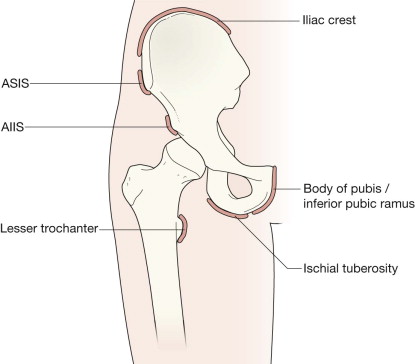
The femur and pelvis of an adolescent will show several small secondary centres (the apophyses).
These should be radiographically identical on the two sides.
An apophysis contributes to the eventual shape and contour of the bone but not to its overall length. Muscles originate from/insert into the apophyses.
Each apophysis has a physis. The physis (ie the growth plate) is a particularly weak part of the developing skeleton.
Detailed inspection should focus on the specific clinical history. Thus…
Check for:
A black line—a displaced fracture—across the femoral neck.
A white line—impacted fracture—in the subcapital region.
A fracture line through the subcapital region, through the trochanteric region, or through the subtrochanteric region.
A fracture of a pubic ramus.
A few fractures are very difficult to detect. If the radiographs appear superficially normal it is important to check again and answer the following questions:
Are the cortical margins of the femoral neck smooth and continuous, or is there a slight step?
Have I checked the lateral radiograph carefully?
Check that:
The femoral apophyses are similar on the painful and unaffected sides.
Check the iliac apophyses.
Check all of the features described above and also check:
The acetabulum: is it fractured?
The femoral head: is it dislocated?
For multiple fractures of the femur and/or the pelvis.
Age 4–10 years: consider Perthe's disease of the femoral head.
Around the age of puberty: consider slipped capital femoral epiphysis.
Age 13–25 years: assess all of the femoral and iliac apophyses. Chronic repetitive stress can affect the tendinous or muscle attachment at an apophysis and produce soft tissue calcification or an apophyseal irregularity.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here