Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Poland syndrome includes a wide range of anomalies that are relevant to the plastic surgeon. From a surgical point of view, priority is given here to discussing the management of the absent pectoralis major muscle, as the associated breast and congenital hand disorders are discussed in detail in other chapters.
Ulnar dimelia is an extremely rare congenital disorder and is usually associated with the mirror hand deformity. The goal of treatment is to improve the global function of the affected limb. The unique features encountered in the hand, wrist, elbow, and shoulder, and present a framework to manage such conditions are discussed.
Congenital radioulnar synostosis is a condition in which an abnormal connection exists between the radius and the ulna, typically in the proximal third of the forearm. Severe cases of hyperpronation or hypersupination are very rare. In most cases, the condition often remains unrecognized until later childhood. Surgical intervention, when indicated, involves osteotomy of the fusion mass or the forearm bones, with the goal of improving severe deformities. Most patients are able to compensate for the absence of forearm rotation through wrist hypermobility and shoulder positioning.
Madelung deformity is a rare condition that results in a characteristic deformity of the distal radius, lunate and distal radioulnar joint. Patients typically present with concerns over the appearance of the wrist, though pain and limitations in wrist range of motion are present in many cases. Management is not well defined and several surgical techniques have been described. For the skeletally immature patient, release of Vickers’ ligament and epiphysiolysis of the distal radius may prevent future need for formal osteotomies. In skeletally mature patients, management may involve osteotomies of the radius, the ulna, or both.
 Access video content for this chapter online at Elsevier eBooks+
Access video content for this chapter online at Elsevier eBooks+
Poland syndrome includes a wide range of anomalies that are relevant to the plastic surgeon. From a surgical point of view, in this section priority is given to discussing the management of the absent pectoralis major muscle, as the associated breast and congenital hand disorders are discussed in detail in other chapters.
Poland syndrome is a non-progressive, rare (Rare Diseases Act 2002) developmental disorder in which one or more components of the upper limb are underdeveloped or absent. Significant deficiency or absence of the sternal head of pectoralis major is the sine qua non of Poland syndrome. The disorder is also referred to as Poland anomaly, Poland’s syndrome, Poland sequence, and unilateral defect of pectoralis muscle and syndactyly of the hand (National Organisation of Rare Disorders).
The common eponym of “Poland” was attached to the disorder by the British surgeon Patrick Clarkson. In 1962 Patrick Clarkson, in his research after having a patient present with Poland syndrome, discovered a similar disorder described in an article from 1848 by Alfred Poland. Alfred Poland’s description itself was based on the autopsy of a convict by the name of George Elt. As is often the case with eponymous disorders, it seems likely that “Poland syndrome” was observed well before Poland described it, for example Lallemand in 1826 and Froriep in 1839.
The pathogenesis of Poland syndrome is not clear. There are various theories that have been proposed as to the mechanism by which it develops, the three most widely held being that there is a genetic basis, an event causing vascular compromise during embryogenesis, and/or that Poland syndrome is a result of teratogenic exposure. While these three causes are often spoken of independently, it should be borne in mind that they are not mutually exclusive. For example, one could hypothesize that teratogen exposure could result in vascular occlusion.
Most cases appear to be sporadic. However, a minority of cases seem to have a familial predisposition. In general, in these cases (though not always), it appears to behave in an autosomal dominant fashion.
The vascular interruption theory suggests that the arterial supply to the upper limb via the subclavian artery is reduced at around the 6th to 7th week of gestation – a critical moment during upper limb embryogenesis as differentiation of the extremity shoulder musculature, vascular tree, and hand are occurring. Interestingly, a vascular interruption hypothesis was postulated by Alfred Poland.
Teratogens have been implicated in the development of Poland syndrome. These include the ergot alkaloids, misoprostol, cocaine, and the biproducts of tobacco smoking.
Poland syndrome may present at birth, but because of the neonate and infant’s habitus, in type 1 or 2B cases ( Table 33.1 ), where there are no upper limb anomalies, it can be missed. In type 2A and 3 cases, neonates and infants, as it is often not obvious, it can often picked up secondarily either by virtue of the associated upper limb anomalies, or associated syndromes such as Moebius, which have led the mindful clinician to check for presence of the sternal head of pectoralis major. Very rarely, there can be associated cardiorespiratory compromise as a result of the associated thoracic anomaly, but these are very much the exception rather than the rule.
| Type | Number | |
|---|---|---|
| 1 | Normal hand (isolated pectoral anomaly) | 3 |
| 2 | Form fruste deformity (the hand appears smaller only when compared to the contralateral side) | 1 |
| 3 | The classic deformity (brachysyndactyly with five potentially functional rays) | |
| A | Mild to moderate hypoplasia of the hand | 8 |
| B | Severe hypoplasia of the hand | 2 |
| 4 | Some functional rays still present | |
| A | Radial club hand with floating or absent thumb | 0 |
| B | Adactyly of the index | 1 |
| C | Adactyly of the index and long fingers | 0 |
| D | Adactyly of the central rays creating a cleft hand | 2 |
| E | Adactyly of the ulnar rays | 0 |
| 5 | All digits are functionless or absent | 2 |
| 6 | Transverse deficiency proximal to the metacarpophalangeal joints | 1 |
| 7 | Phocomelia-like deficiency | 0 |
Cases that have not come to the clinician’s attention at an early stage are often not identified until the child has become self-conscious about the appearance of the chest wall or upper limb. Very often this occurs around 10 years of age, but is highly variable. While the disorder is not progressive, the morphological anomalies may become more obvious as the child and family may notice failure of development of chest wall musculature or breast tissue compared to the contralateral side. In the very rare bilateral cases, the symmetry of the disorder may make it extremely difficult to make the diagnosis.
Diagnosis of Poland syndrome is by clinical demonstration of underdevelopment or absence of the sternal head of pectoralis major, rarely requiring confirmatory imaging. Thereafter, ultrasound imaging can help confirm the absence of any associated thoracic or visceral (particularly renal) anomalies ( Figs. 33.1 & 33.2 ).
, mammary hypoplasia, and a relatively small and superiorly displaced nipple areolar complex.")

In general, the diagnosis is made clear by absence or significant deficiency of the sternal head of pectoralis major. However, with regards to the chest, differential diagnoses may include any developmental or acquired disorder in which there is unilateral hypoplasia. Soft tissue examples are amastia or amazia with a normal underlying pectoralis, rare forms of Parry–Romberg, localized lipoatrophy and following trauma, and disorders of the morphology of the diaphragm. Disorders of the thoracic skeleton may also appear similar to Poland syndrome, for example severe scoliosis or costal dysplasia, as can proximodistal failures of formation and differentiation.
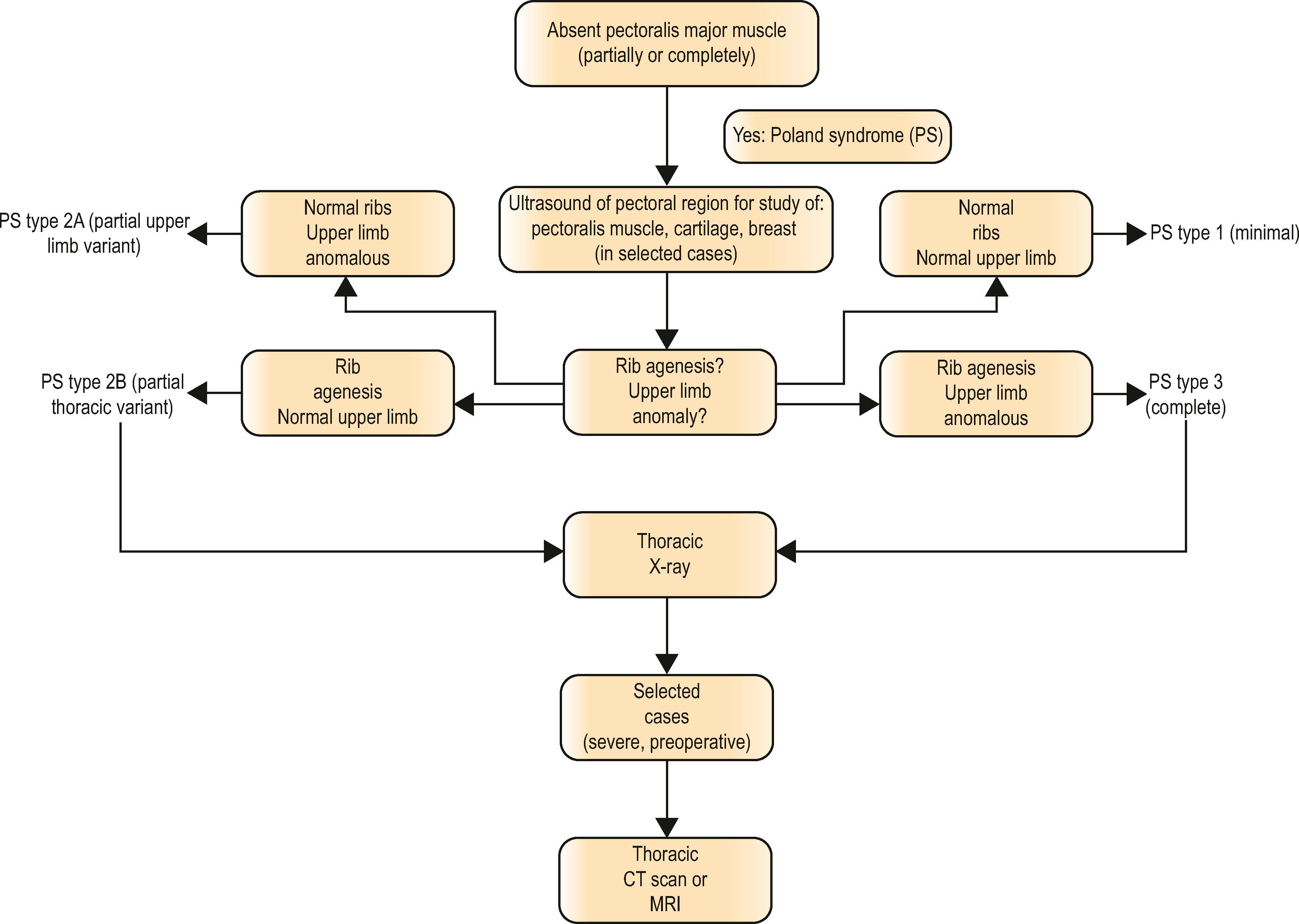
With regards to the chest wall, imaging should be performed to check for the presence and severity of any chest wall anomalies. Initially the same ultrasound that was used to check for associated visceral or internal organ anomalies is ideal. Thereafter, if anomalies are detected, radiographs and computerized tomography (CT) may be used to further classify them (see Algorithm 33.1 ). In general, unless a pressing clinical need for CT evaluation exists, the authors prefer to wait until the child is over the age of 5, in order to mitigate the risks of radiation and potential discomfort in the scanner.
Given the links to hematological disorders, a blood panel can be performed as well.
The management of Poland syndrome can be divided into the management of emergent complications, possible psychosocial concerns, and functional and aesthetic problems.
It is very rare to have cardiorespiratory compromise requiring emergent intervention. This may occur, for example, in the presence of severe chest wall hypoplasia causing an incomplete thoracic “ring” that results in respiratory compromise and paradoxical breathing comparable to having a flail chest and mandating mechanical ventilation. In such situations, urgent surgical completion of the thoracic deficit by spanning the sternum and the vestigial hypoplastic ribs with a polytetrofluoroethylene or titanium implant may be necessary.
Among the greatest concerns for patients and children with limb anomalies is physical appearance and self-perception. Appearance-related distress may influence how they interact with their peers. The child’s and parents’ anxieties about social functioning should be addressed early on in the consultation process, for example with input from a clinical psychologist, and information about support groups; for example in the UK, the Pip-UK Support Network. Empirically, the authors also find that making families aware of high-functioning positive role models (such as the actor Ted Danson, Olympic boxer Jerome Thomas and Formula One driver Fernando Alonso) can help reassure the patient and parents about the condition and future prospects.
The management of the functional and aesthetic aspects of Poland syndrome can be broken down into the following anatomical categories:
Management of the thoracic chest wall anomalies
Management of the pectoral deformity
Management of the breast
Management of the limb anomalies
Management of the thoracic wall anomalies, breast and limb anomalies, variations of which can also be present without Poland syndrome, are described in detail in the relevant chapters. In this chapter, focus is given to management of the underdeveloped or absent pectoralis major muscle.
The authors have found that the most common reason for patients to seek surgery for the underdeveloped sternal component pectoralis major is to improve the appearance of symmetry, specifically: (1) to recreate the anterior axillary fold and (2) to cover the visible ipsilateral ribs. Interestingly, rarely do patients request surgery for functional reasons. While there is a received wisdom that absence of the pectoralis major muscle has little functional effect, studies that have quantitatively analysed the strength of shoulder function in Poland syndrome patients have found reductions in the strength of both internal rotation and adduction. Despite that, research also suggests that there is little practical functional limitation to the absence of the pectoralis muscle, with people functioning, for example as high-level athletes (e.g., Jerome Thomas and Fernando Alonso, as mentioned above) and infantrymen. These two apparently conflicting observations are reconcilable by considering that people with the disorder often find various ways to comfortably compensate.
Surgical decision-making with regard to reconstruction of the pectoralis major should be made in a multidisciplinary environment, with engagement from the family, psychological support services and therapy services. While it has been postulated that surgery by functional muscle transfer of the latissimus dorsi muscle can improve strength, the authors feel that the main benefit is in general not functional but aesthetic, with a view to improving self-image, and should be discussed as such with the family (children will generally overcome the functional deficit). The functional merits should be seen as secondary. Inclusion of psychological support services into discussions with the family is therefore vital, and other extraneous factors that may be contributing to their decision-making, such as bullying, should be explored. It must be made clear that while improvement can and should be expected, complete symmetry is very unlikely. Timing is also crucial. Given that this is not an essential reconstruction, and that many people function extremely well physically and socially without the pectoralis major, the authors feel that surgery should be undertaken when there is clear engagement and desire for it from not just the family, but from the patient. The age at which a child is mature enough to be involved in these decisions is obviously variable, but in the authors’ experience, this is rarely before the age of about 8 years. While there is merit in performing surgery following adolescence, as the morphological changes associated with puberty can deleteriously effect results, often the issues of self-confidence and social functioning that precipitate the seeking of intervention may mean that delaying till after puberty is not practicable. However, the authors caution against reconstruction of the breast mound in females early on, to mitigate against multiple surgeries.
If surgery for pectoral reconstruction is deemed appropriate, there are three basic commonly used choices:
Autologous fat transfer: This has the advantage of minimal donor site morbidity and the avoidance of alloplastic material, and the flexibility of the process enabling cosmetic fine-tuning. The downside is that it usually requires multiple operations, is not dynamic, and as it has no intrinsic structural integrity, creation of an anterior axillary fold is difficult.
Custom-made prosthesis . This solution works well for patients not also requiring a separate prosthesis for mammary reconstruction. In general, these are made using computer tomography to design a custom digitally designed prosthesis. The advantages of the prosthesis are that in a patient who has reached maturity, it can be used as a single-stage procedure with a relatively accurate and predictable result. The disadvantages are those inherent with placement of alloplastic material (such as infection, and extrusion). Furthermore, there is a lack of dynamism, and it does not alter with body habitus or developmental changes (meaning a high likelihood of requiring later revisional procedures if placed before physical maturity). Older reports suggest a relatively high complication rate (displacement, extrusion), although more recent reports less so.
Latissimus dorsi flap: In this procedure, the muscle is harvested from an axillary approach, and transferred anteriorly to recreate the anterior axillary fold and provide soft-tissue bulk to cover the affected thoracic skeleton. The primary disadvantage of this procedure is the donor site morbidity, both cosmetically and functionally. The advantages are that it can create a good anterior axillary fold, that it can potentially improve strength at the shoulder, it can avoid alloplastic material and can provide good quality coverage where alloplastic material is required for mammary or thoracic reconstruction. Occasionally, the ipsilateral latissimus dorsi is too underdeveloped, or absent, and so cannot be transferred. In these cases, a free contralateral latissimus may be used.
The author’s preferred procedure is the latissimus dorsi flap, which can itself be supplemented with fat grafting to fine tune thereafter or used in conjunction with a prosthesis. Access is through an axillary incision. A muscle flap is raised on its thoracodorsal pedicle from its chest wall origin. The authors prefer not to divide the humeral insertion, though sometimes this is necessary to give adequate mobilization. Although functional improvement is not the primary reason for surgery, it is a useful secondary benefit, and in order to allow this, heavy non-absorbable anchoring sutures to the sternum are used. To prevent issues of postoperative muscle spasm, botulinum toxin may be used into the latissimus dorsi muscle that has been transferred.
In Poland syndrome, the congenital differences seen in the affected hand ranges from completely normal appearance to varying forms of brachydactyly and symbrachydactyly. Management of symbrachydactyly follows the same algorithms for management of syndactyly, with prioritization of first webspace reconstruction and elimination or reconstruction of hypoplastic central ray digits ( Fig. 33.3 ; ).
 A 5-year-old girl with Poland syndrome affecting development of the left chest wall and left-hand development (symbrachydactyly). (B,C) Appearance of the same patient’s left hand at 2 years of age. (D,E) Appearance of hand at 5 years of age, after reconstruction of 1st and 4th webspaces and removal of 3rd ray. (F,G) X-rays of affected hand corresponding to clinical pictures.")
A postoperative collar and sling preventing abduction for 3 weeks is advisable. Muscle atrophy is common thereafter, particularly with the use of botulinum toxin, and a postoperative strengthening regimen should be undertaken.
Outcomes following surgery are variable, reflecting variations in severity of the condition, and social support networks of the affected patients. In general, the aesthetic outcomes for the surgical management of the soft-tissue chest wall deformity in Poland syndrome are good, whether looking at the use of prostheses, fat transfer or latissimus dorsi muscle transfer. There are, however, few papers that compare the outcomes of the different types of reconstruction. One study assessing Poland reconstruction combined with breast reconstruction suggested better outcomes following procedures involving latissimus dorsi transfer. A similar finding is presented by Seyfer et al . ; the authors of this study advised against custom-made prosthesis given relatively high rates of displacement and extrusion, though the study dates from 1988.
Interestingly, the study by Papadopulos et al . also showed higher subjective satisfaction in patients with Poland syndrome who had undergone reconstruction than in normal control subjects who had not had operations. A study of 28 patients by Schippers et al ., with long-term follow-up (mean 25 years) found that patients with Poland syndrome – most of whom had undergone reconstructive surgery – had higher than average satisfaction-with-life scores, and also rates of marriage, educational level and employment that met or exceeded those of the general population.
Finally, given the previously described physically high-functioning groups of patients previously mentioned, it must be considered that it is perfectly possible to have an excellent quality of life without having reconstruction of the pectoralis major. That being said, what is currently lacking is good outcome data comparing non-operated patients with operated patients for Poland syndrome.
As mentioned previously, reconstruction of the pectoral can be augmented by fat grafting if required. Furthermore, reconstruction of the pectoralis major can be performed primarily by free tissue transfer or as a salvage procedure after other reconstruction. Reconstruction of the nipple areolar complex can be performed if needed with prosthesis, or combination of nipple reconstruction and tattooing. Particularly in younger children, if growing, a prosthesis is often preferable as it mitigates against the risk of asymmetrical developmental changes between the unaffected and affected sides. If chest wall reconstruction is required, this can be performed in conjunction with latissimus dorsi transfer, or as a staged procedure. Finally, hand reconstruction, e.g., symbrachydactyly, syndactyly reconstruction, should be addressed per usual for a child with the given congenital hand anomaly. In general, these will typically be addressed prior to consideration of chest wall symmetry procedures.
Advances in our understanding of the possible genetic basis of Poland syndrome have recently been described in familial cases, which may help us understand the developmental pathogenesis of the anomaly. For example, Vaccari et al . recently described monozygotic twins with Poland syndrome who shared the same chromosomal deletion (11q12.3). The affected genes are involved in cell growth, differentiation and programmed cell death, potentially implicating failures of these processes in the disorder. However, no study has yet concretely demonstrated a specific genetic causal link for Poland syndrome.
On the surgical front, new developments with custom-made implants show great promise for reconstructing the chest wall deformity with limited incisions and no donor site morbidity. To date, these techniques have required CT scans of the thorax, followed by three-dimensional (3D) computer-aided design model of the defect/implants, creation implant prototypes, and ultimately a permanent implant made from solid rubber silicone that is highly flexible, tear-resistant, and gas-sterilized. To date, this custom implant-based technology is not yet available in the United States.
Dissection of the muscle flap and the pocket is greatly facilitated by the use of a Tebbett’s lighted retractor, as used in breast augmentation. The authors’ preference is the disposable plastic Tebbett’s retractor.
During surgery, initially a postoperative local anesthetic supraclavicular block and botulinum toxin can be used in the transferred muscle to reduce the risk of muscle spasm/contraction and subsequent rupture of anchoring sutures. A low dose of benzodiazepines may be also used to prevent this and for comfort to bridge the time between the effects of the supraclavicular block and the effects of the botulinum toxin (in general) for no more than a few days.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here