Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Currently most Asian patients want aesthetic improvement with ethnic preservation.
Asian blepharoplasty deals with widening of the eye from all quarters, not just creating a supratarsal fold.
Asian rhinoplasty is revolutionized with various new concepts and techniques, such as quadripod theory, septum-based nasal tip plasty, and various extension graft techniques.
Asian facial bone contouring is evolving from simple bony resection to relocation and balanced facial bone resection. Aesthetic orthognathic surgery aims to balance the facial proportion based on occlusal plane changes and maxillomandibular rotations.
In Asian facelifts, the soft tissue and underlying skeleton should be considered to ensure successful facial rejuvenation.
Everything is in the face.
Access video and video lecture content for this chapter online at Elsevier eBooks+ 

The face, while only a single part of the body, is the icon of self-identity and easy recognition. Facial cosmetic surgery is becoming increasingly popular among Asians. Although many countries use the term “Asia” referring to land masses where more than half of the world’s population resides, the word actually refers to people of East, Southeast, and South Asia with a Mongoloid ancestry (e.g., Koreans, Japanese, Chinese, Vietnamese, Filipinos, Indonesians). Asian and Caucasian faces each have unique features. Asians generally have small and puffy eyes with an epicanthal fold, shallow orbits, low-profile nasal dorsum with thick skin, flat faces with large cheekbones, and broad widths. This is especially true for East Asians. However, as the largest continent, Asia has numerous ethnic groups. Southern Asians have darker, thicker skin, larger eyes with double folds, and smaller, narrower facial skeletons compared to northern Asians, whereas Western Asians have unique features. Despite some constants, standards of beauty vary among countries. Anatomic characteristics and cultural differences, including ethnic trends, should be considered before performing facial cosmetic surgery.
Populations of Asian and non-Asian ethnicity have both similarities and differences in facial skeletons and soft tissues. However, regardless of origin, the face, including the eye, nose, and facial contour, consists of three-dimensional structures, which should be familiar to all surgeons to get an ideal of facial aesthetics. Facial projection, width, and height are important considerations in all facial aesthetic procedures ( Fig. 15.1 ) The understanding of this three-dimensional concept is essential for plastic surgeons. For example, the nose is also a three-dimensional structure. The rhinoplasty adds a significant dimension in the sagittal profile, but also gives a change in coronal and axial plane. Approaching Asian facial aesthetic surgery with an understanding of the three-dimensional concept and multiple contour planes allows for easier selection of the ideal treatment.
Facial projection may be enhanced by forehead augmentation with implant or fat grafting, augmentation rhinoplasty, orthognathic surgery, bimaxillary anterior segmental ostectomy (ASO), or advancing genioplasty. Given that most Asians tend to have brachycephalic features, aesthetic procedures often focus on enhancing anterior projection.
Malarplasty and mandibuloplasty are popular in Asian countries because these procedures help balance facial widths. While facial bone contouring is aimed at narrowing the facial width, blepharoplasty, including medial and lateral canthoplasty, widens the eye to create a balance between the eye and the face.
Forehead narrowing plasty, blepharoplasty, rhinoplasty, orthognathic surgery, and genioplasty are being performed in many Asian countries to improve facial vertical balance. Contemporary Asian blepharoplasty aims at four-directional widening, which includes vertical widening based on subclinical ptosis correction and horizontal widening based on medial and lateral canthoplasty.

It is incorrect to assume that Asians seek to “Westernize” their faces. Most Asian patients now want to preserve their ethnic background, aside from enhancing their appearance ( Fig. 15.2 ). Based on cultural differences among races, the perception of attractiveness, or beauty, seemed to be different between Asian and Western subjects. Advances in facial anthropometry have clarified the ideals that Asian subjects seek from their facial cosmetic surgery. Certain studies using 3D photogrammetry have documented differences in facial proportions between attractive Asian and Western women. Overall proportions of attractive women’s faces were found to be similar between the two ethnicities, but several differences were identified in terms of facial proportions. Attractive Asian women have a longer midface than the lower face, while attractive Western subjects tend to have thicker lips, longer chins, and relatively shorter midfaces. In general, Asians consider prominent appearance of zygomas and mandibles as unfavorable, leading to numerous techniques focusing on bony reduction and contouring. As the concept of attractiveness is constantly evolving, surgeons should be aware of recent trends and be familiar with anthropometric data regarding what is considered attractive and normal ( Fig. 15.3 and Table 15.1 ).


| Facial height ratio (upper : middle : lower) | ICW (%) | PW (%) | LW (%) | NW (%) | NH (%) | LH (%) | CH (%) | |
|---|---|---|---|---|---|---|---|---|
| Anthropometry in ordinary young females | ||||||||
| Farkas et al . | ||||||||
| North American | 35.6 : 27.5 : 36.9 | 24.3 | 23.6 | 38.3 | 24.2 | 27.5 | NA | NA |
| German | 35.9 : 27 : 37.1 | 23.2 | 25.8 | 39.1 | 25.1 | 27 | NA | NA |
| Thailand | 34.7 : 29.1 : 36.2 | 26 | 20.9 | 32.8 | 29.1 | 29.1 | NA | NA |
| Singaporean Chinese | 34.8 : 27.5 : 37.7 | 26.5 | 20.9 | 34.7 | 27.3 | 27.5 | NA | NA |
| Japanese | 37.8 : 27.9 : 34.3 | 24.8 | 20.7 | 32.9 | 26.3 | 27.9 | NA | NA |
| Choi, Kim et al . | ||||||||
| Korean | 53.6 : 70.8 : 62.6 | 28.4 | 20.5 | 34.8 | 31 | 27.8 | 8.8 | 22.2 |
| Anthropometry in attractive young females | ||||||||
| Rhee | ||||||||
| East Asian (Korean, Japanese, Chinese) | 31.5 : 36.3 : 32.2 | 20.7 | 16.1 | 28.6 | 28.2 | 23.0 | 8.4 | NA |
| Caucasian | 31.5 : 35.6 : 32.8 | 17.3 | 15.7 | 27.4 | 26.1 | 21.5 | 8.5 | NA |
| Burusapat and Lekdaeng | ||||||||
| Thailand | 33.4 : 33.3 : 33.4 | 21.7 | 20.2 | NA | NA | NA | NA | NA |
| Diverse ethnicity | 35.8 : 31.5 : 32.6 | 22.3 | 23.9 | NA | NA | NA | NA | NA |
| Galantucci et al . | ||||||||
| Caucasian | 36.4 : 28.7 : 34.9 | 23.2 | 21.1 | 34.7 | 24.0 | 28.7 | 10.3 | NA |
| Choi, Yi et al . | ||||||||
| Korean | 29.3 : 38.5 : 32.1 | 24.3 | 19.8 | 31.1 | 26.9 | 29 | 9.2 | 22.2 |
| Paraguayan | 27.9 : 37.4 : 34.7 | 23 | 21.4 | 33.6 | 28.5 | 28.2 | 10 | 23.5 |
Blepharoplasty does not appear to be the most commonly performed cosmetic operation in North American and European countries, whereas it is the most popular plastic surgery procedure in East Asian countries, with about 30%–60% of Asian women from metropolitan areas undergoing this procedure. The patient demographics are also significantly different. In the West, older patients often desire to undergo rejuvenation surgery, while in the East, it is increasingly younger patients who are paying attention to aesthetic procedures.
In general, Asian women tend to have relatively wide-set eyes, puffy upper eyelids, slanted canthal angles, and low-set or absent eyelid creases. Periorbital beauty standards in Asians have changed. It is affected by Western influences and socio-cultural trends. Facial attractiveness depends on certain relationships between periorbital structures. Given that blepharoplasty is a common operation in Asian women, surgeons should be familiar with the spatial relationships between periorbital structures.
Recent studies have examined the anthropometric differences in periorbital structures between attractive persons of different ethnicities. Attractive Asian women have certain proportions in periorbital structures, with 10%–20% greater intercanthal width ratios as palpebral width ratios and 2.4 times greater palpebral width-to-height ratios. Western women have a narrower intercanthal distance, with 5%–10% greater intercanthal width as palpebral widths, and 2.6 times greater palpebral width-to-height ratios ( Fig. 15.4 ).

Historically, plastic surgery literature from Western countries has described Asian individuals as having puffy creaseless eyelids and epicanthal folds, both of which obscure the visual field. This stereotypic generalization has received scrutiny in the past four decades, and we now understand that about half of East Asian women have clear supratarsal folds without strongly conspicuous epicanthal folds. The post-World War II surgeons from the US and Europe reported that Asian patients wanted to have Caucasian “round eyes”. However, this perception of “Western” norms has shifted or has been rejected in East Asian countries. Most contemporary Asian patients do not favor Caucasian eyelids. Large deep-set eyelids with high creases do not compliment the overall harmony of the Asian face. Therefore, blepharoplasty should reflect the ethnic identity ( Fig. 15.5 ).
 The differences in skeleton and levator attachment make Oriental eyes look different (B) . Multiple theories exist regarding the formation of the supratarsal crease or fold. First theory: expansions of the levator palpebrae superioris muscle penetrating through the septum and orbicularis oculi muscle to the overlying dermis were thought to be more present in Caucasian eyelids. Second theory: supratarsal crease formation is the level of fusion of the orbital septa and the levator aponeurosis. The level of adhesion defines the superior palpebral crease in most Caucasian eyelids, whereas lower fusions results in a low-lying or absent crease in the Asian eyelid. Third theory: the skeletal differences cause eyelid differences.")
Surgically created supratarsal fold or “double eyelid” was first described by Mikamo in 1896 for a patient who lacked an upper eyelid fold. Shirakabe et al . made a historical review of 32 surgical techniques reported in Japan. Sayoc also considered anatomic upper eyelid differences between Caucasian and East Asian populations in terms of blepharoplasties. Hawaii served as the first testing ground, with surgeons such as Fernandez and Flowers publishing a series of studies and essays on blepharoplasty in Asian patients. Subsequent developments in blepharoplasty include further aesthetic refinements and minimally invasive approaches.
Blepharoplasty should be performed while respecting the anatomical differences between Asian and Caucasian eyelids. Decades ago, Asian patients just wanted to form visible supratarsal creases. More recently, Asian blepharoplasty has evolved not just to create the supratarsal fold but also to reduce eyelid puffiness, and increase the palpebral fissure width. Reducing eyelid puffiness does not equate to sunken or deflated upper eyelids.
Height, depth, adhesion, power, and volume should be considered in natural double eyelid formation ( Fig. 15.6 ), with each factor contributing to making a “favorable fold”. A favorable fold cannot be created if one factor is inappropriate; therefore, these factors should be considered in detail.
Height : In Asian blepharoplasty vernacular, the lower border of the supratarsal fold is called the “double eyelid line”, and the distance between this line and the eyelid margin at primary gaze is termed “pretarsal exposure” or “show”. Asian plastic surgeons have previously created high double folds owing to the influence of Westernization. Nowadays, the height of the fold is reduced to create a natural double fold.
Depth : Depth is defined as the distance between the anterior and posterior lamellae at the primary gaze. Higher lower flaps indicate deeper-formed double fold.
Adhesion : Appropriate adhesion is required for double fold maintenance. During incisional double-eyelidplasty, any soft tissue interfering with the connection between the anterior and posterior lamellae should be adequately removed. However, if excess pretarsal tissue is removed, the fold line easily becomes unnatural, and a depressed scar may be formed.
Power : The levator function is the most fundamental factor for creating a natural double fold. Impaired levator function releases the double fold, thereby it looks unnatural.
Volume : Adequate upper eyelid volume helps create a natural double fold. If this volume is insufficient, the fold line may not form well. Conversely, high volumes may leave unnatural appearance of the line.
 Height: a , double eyelid line, lower border of fold; b , upper lid margin; c . pretarsal exposure; d , lower lid margin. (B) Depth: the black line represents the fixed anterior lamellar height. Higher heights indicate longer lines and deeper double folds. (C) Adhesion: depending on the degree of removal of the pretarsal soft tissue, a linear adhesion (left) and a planar adhesion (right) are formed. (D) Volume, which is proportional to the height.")
The shape of the desired crease should also be considered. Typically, the Caucasian eyelid crease has a semilunar shape, as the central third is farthest from the lash line. This semilunar shape appears unnatural to Asian patients, who prefer a parallel crease to the lid margin. Laterally, the ideal crease has slightly less curvature such that the crease is farther from the lash line than the central third. This lateral flare gives an uplifted upper eyelid appearance, minimizing the bunching of skin flaps that commonly occurs over the lateral canthus. Medially, the crease may taper toward the medial canthus (i.e., “tapered fold”) or run outside the epicanthus (i.e., “parallel fold”) ( Fig. 15.7 ).

The desired double eyelid shape varies according to the individual. Preoperatively, the surgeon and patient should agree regarding the height and shape of the fold. The fold height and shape can be simulated using a bent paper clip or a similar instrument, or the patients may bring model images.
The surgery involves creating a supratarsal crease by forming a connection between the anterior (dermis, orbicularis oculi muscle [OOM]) and posterior (levator complex, tarsal plate) lamellae of the upper eyelids. Double blepharoplasty techniques can generally be categorized as “non-incisional” or “incisional”.
The advantages of the non-incisional method are minimal scarring and a short recovery time. However, the fixation may be looser than with the incisional method. Therefore, this method is not suitable for Asian individuals with conditions that may increase the risk of double fold loosening, such as thick eyelid skin or excess orbital fat ( Fig. 15.8 ).

The non-incisional method creates a mechanical connection between the anterior and posterior lamellae by introducing a suture through a pinpoint access incision formed by a needle or scalpel tip. Numerous non-incisional techniques have been previously described. Currently, the most common technique is the single-knot continuous buried method ( Fig. 15.9 ), by using 5–6 pinpoint incisions to insert stitches. The stitches are then tied to create a single knot, resulting in a double-fold line.

During this technique, local anesthetic is injected into the skin and conjunctiva, and 5–6 pinpoint incisions are made along the marked fold line. The stitch is then inserted through the incisions from the skin side to the conjunctival side and then back to the skin side. With this, a single stitch passes through the entire fold line, connecting the dermis and levator complex. The surgery is complete when a knot is created at the incision where the stitch is initially inserted. Surgeons should tie the knot well to avoid creating an excessively loose or deep double eyelid ( ).
The incisional method is often preferred for Asian individuals because of the anatomical characteristics of their eyelids ( Fig. 15.10 ).
Dermatochalasis
Thick eyelid skin
Excessive orbital fat
Moderate-to-severe blepharoptosis

Traditionally, fixation using a simple tarsodermal suture is the most common method. Currently, double-eyelidplasty has evolved to enable careful manipulation of more diverse tissues to create more natural and dynamic double folds ( Box 15.1 ). Because there is no gold standard for incisional double-eyelidplasty, surgeons select the best technique based on their experience while considering the previously mentioned five factors. In general, the following steps were performed during the incisional method.
Incision: A skin incision is made along the marked fold line after surgical preparation and injection of a local anesthetic agent.
Dissection: An incision is made to the exposed layer of the OOM and the orbital septum.
Fat removal: If a puffy eyelid is present, the septum is opened to remove an adequate septal fat. If additional debulking is required, the retro-orbicularis fat can also be removed.
Exposure of tarsal plate: After making an incision to the pretarsal area, the upper border of the tarsal plate is dissected and exposed. For optimal fixation, some pretarsal tissues should be preserved.
Pretarsal preparation: Pretarsal soft-tissue removal is the most important step in incisional double-eyelidplasty. An adequate amount of soft tissue should be removed to connect the anterior and posterior lamellae without tension. Conservative removal is critical here to avoid depressed scar formation. In most cases, removal of the pretarsal soft tissue is sufficient, but OOM removal can also be performed ( ).
Fixation: The dermis, OOM, or musculocutaneous junction, is fixed to the posterior lamellar tissues to make a double fold. The posterior lamella tissue used may vary according to the surgeon’s preference. For example, tarsal plate, levator aponeurosis, tarsus-aponeurosis, or septo-aponeurotic junctional thickening (SAJT) can be used; alternatively, several tissues may be simultaneously used ( Fig. 15.12 ). Usually, 5–8 fixation points are used ( ).
 Tarsodermal fixation. (B) Tarsus–dermis–aponeurosis fixation. (C) Dermis–aponeurosis fixation. (D) Septo-aponeurotic junctional thickening fixation.")
Check double fold: The depth of the fold is checked by lid eversion. It is generally appropriate to fix the double fold enough to induce a mild outward turn of the eyelash to prevent double fold loosening.
Skin excision: The presence of remnant skin was estimated by spreading the upper flap to the incision site. The skin should be excised without tension to prevent scar widening on the double fold.
In a naturally occurring double fold, the double fold line is either not visible or only a shallow crease is noted when the eyes are closed. As soon as the eyes are opened, the double fold line begins to crease and appear due to the connection between the levator complex and dermis. This is called a dynamic double fold, which is the surgical goal of double-eyelidplasty. However, depressed scars are likely after incisional double-eyelidplasty due to various causes. Consequently, this results in an unnatural double eyelid and a visible depressed double fold line upon eye opening and closing. This is called a static double fold and commonly causes secondary double-eyelidplasty.
 Static double fold. When the eyes are closed, a deeply depressed scar is observed, and when the eyes are opened, a very unnatural double eyelid is observed. (Below) Dynamic double fold. The scar was almost invisible with the eyes closed, and a natural double eyelid was observed with the eyes opened.")
In decreased levator function, double eyelids easily become loosened and will not fold well, creating an unnatural result. Therefore, Asian patients should be precisely evaluated to correct the blepharoptosis.
Patients of both Asian and non-Asian origin share similarities in causes and related anatomy of blepharoptosis. However, Asian individuals desire to have larger and more attractive eyes. Therefore, subclinical ptosis is often corrected simultaneously with double blepharoplasty.
Non-incisional ptosis correction has become popular in East Asia since its introduction by Shimizu, as it is able to correct subclinical ptosis without incision or dissection. However, relapse can occur postoperatively. Furthermore, repeat procedures may cause scar contractures, complicating re-operations. The procedure can be performed anteriorly or posteriorly, and a Müller tucking suture is created on the conjunctival side ( Fig. 15.13 ).

The incisional method can correct any degree of ptosis with a lower recurrence rate. Levator complex advancement and shortening are the basic principles of ptosis surgery. In this procedure, the mass effect is proportional to the degree of advancement and shortening ( Box 15.2 ) Therefore, the surgical approach varies according to the degree of ptosis.
The principle of levator complex plication surgery is to fold the levator complex to shorten its length. This method is performed without separation of the tarsus and levator complex. Therefore, as the amount of folding of the levator complex increases, the volume of the folded levator complex increases and the effect of shortening by folding gradually decreases. This is called the mass effect. Therefore, for ptosis of more than a moderate degree that requires significant levator complex shortening, surgical methods that reduce the mass effect are required.
Levator resection produces the least mass effect. However, a lot of dissection is required. For moderate-degree ptosis requiring moderate correction, a proper combination of levator complex plication and levator resection can be used ( Fig. 15.14C ).
Levator plication, a relatively simple method, is commonly used. In conventional levator plication, only the levator aponeurosis is used; therefore, recurrence is common. Plication of the entire levator complex is often performed, greatly reducing the recurrence rate ( Fig. 15.14A ). The levator resection method is suitable for severe ptosis requiring a large amount of levator complex shortening ( Fig. 15.14B ).
 Levator complex plication. The thread is passed between the Müller muscle and the conjunctiva with dissection between the levator aponeurosis and the tarsal plate but without dissection between the Müller muscle and the conjunctiva. The posterior levator complex is advanced, folded, and fixed to the tarsus. The adhesion established between the posterior part of the Müller muscle, the tarsal plate, and between the layers of Müller’s muscle itself is stronger. (B) Levator resection method: after dissection between the Müller muscle and the conjunctiva, the levator complex is pulled and fixed to the tarsal plate. Since the levator complex is advanced without folding, the mass effect is minimal. Therefore, use of the levator resection method is suitable in cases of severe ptosis requiring significant correction. (C) Combined levator complex plication and levator resection: the tarsus and levator complex are separated to slightly dissect between the Müller muscle and conjunctiva. Then, levator complex advancement is performed to reduce the mass effect.")
With the increase in Asian blepharoplasties, the need for secondary double-eyelidplasty has also significantly increased. There are various causes for this, such as asymmetry, looseness, abnormal shape, or most commonly, a high and deep location of the double eyelids, giving an unnatural appearance.
This section focuses on secondary double-eyelidplasty for unnatural double eyelids. The process involves identifying the problem among the factors for natural double eyelid formation, completely releasing the existing adhesion, and creating a new natural double eyelid.
Since secondary double-eyelidplasty is indicated due to a combination of the problems, it releases all existing adhesions and corrects each of these problems.
The double eyelid height is determined through preoperative consultation with the patient. Asians generally prefer a double eyelid line height of 5–10 mm from the lid margin, but patient preferences may vary. Double eyelids were previously designed highly because it was expected to make the eyes look bigger. Nowadays, people prefer naturally appropriate double eyelids. Therefore, the double eyelid height is surgically reduced ( Fig. 15.15 ).

The surgical procedure is as follows:
A double eyelid line is designed lower than the existing line.
All preaponeurotic and preseptal plane adhesions are released after incision.
The lower flap is fixed at the appropriate height.
The scar is excised if there is sufficient skin ( Fig. 15.16A ). Otherwise, the scar tissue is used as part of the upper flap to reduce the pretarsal show ( Fig. 15.16B ).
 Skin sufficient. If the skin is sufficient, the existing scar can be excised. (B) Skin insufficient. If the skin is insufficient, an incision is made under the existing scar to release the adhesions.")
Double eyelids look deep and unnatural if the lower flap (anterior lamella) is fixed at a point that is significantly higher than the incision line, even if the double eyelids are designed at an appropriate height ( Fig. 15.17 ). The principle of deep double eyelid correction is to release all adhesions and lower the lower flap fixation ( Fig. 15.18 ). Many patients with deep double eyelids also have coexisting high double eyelids. In such cases, the correction principle is the same as that for height reduction. However, fixation of the lower flap should be performed at a point lower than the previously fixed point.


When excessive pretarsal soft tissue is removed during the first operation, it leads to the formation of static double eyelids. These patients present with depressed scars due to excessive adhesion formation, making the double eyelids look unnatural. This is especially noticeable when the eyes are closed ( Fig. 15.19 ). Correction aims to completely release the adhesion between the anterior lamella of the lower flap and tarsus. The lower flap should be fixed without tension to prevent excessive adhesions.
 and after (below) re-operation of a patient with double eyelid adhesion problem.")
Most patients who require secondary double-eyelidplasty are accompanied by ptosis for the following reasons:
Ptosis misdiagnosis or neglect: If only double-eyelidplasty is performed without ptosis correction, the double eyelid is easily loosened and an unnatural double eyelid is created. In addition, ptosis may become more severe.
Adhesion on the levator gliding plane: If adhesions were previously made to the gliding plane of the levator, ptosis occurs.
These unnatural double eyelids should be addressed with appropriate adhesiolysis and ptosis correction. Ptosis correction in secondary blepharoplasty does not differ from primary surgery, but the previous adhesion between the tarsal plate and levator complex should be released to prevent recurrence.
The unnatural double eyelid has a sunken upper eyelid, mostly because of an insufficient upper flap volume. If accompanied by ptosis, ptosis correction is performed, and the orbital fat is repositioned to the sunken area. In most cases, this problem is addressed without resorting to fat injections. Conversely, for puffy eyelids, despite an appropriate double eyelid height, they appear unnatural; therefore, the height should be reduced.
Asian blepharoplasty has a high demand for expansion of the palpebral fissure. Thus, surgery to expand the area of the white scleral triangle in all four directions of the eye has been developed. These can be performed alone or combined with double blepharoplasty to maximize the effect ( Figs. 15.20 & 15.21 ).

.")
Asian eyelids have an epicanthal fold, which is a medial extension of the upper eyelid skin covering a portion of the lacrimal lake and shortening the eye length. In addition, it inhibits the formation of double eyelids. Therefore, numerous medial epicanthoplasty methods have been established.
Most traditional methods leave a noticeable scar in the intercanthal area; hence, they are not commonly used. The skin redrape method, first introduced by Dr. Oh, is currently the most popular method, and results in barely visible scars because the incision follows the subciliary line of the lower lid, and the tension is sufficiently released ( Fig. 15.22 ).

The Caucasian upward canthal slant gives a youthful and attractive impression. On the other hand, Asians perceive the upward canthal slant to provide a sharp impression with smaller eyes ; therefore, they prefer otherwise. As Asian individuals commonly have elevated canthal slants, various canthal slant-lowering and length-increasing methods have been developed. Currently, lateral canthal lengthening is divided into two categories: (1) moving the lateral canthus after lateral canthotomy to control the canthal slant and the canthal length, and (2) elevating the rotation flap in the lateral canthus for lower lid extension ( Fig. 15.23 ) (  ).
).
 Rotation flap method. (B) Lateral canthotomy method. (C) Canthal angle-preserving lateral canthotomy method.")
In reverse ptosis, in which the lower limbus is obscured by the lower lid, lowering the lower lid to expand the palpebral fissure enlarges the eyes. In addition, lowering of the lower lateral eyelid can have a similar effect as lowering the canthal slant. The surgery is performed by suturing the tarsus to various tissues of the lower lid, such as the capsulopalpebral fascia, arcuate expansion, and arcus marginalis, via the transconjunctival approach ( Fig. 15.24 ).

The aging process does not differ between those of Asian and Caucasian ancestry; however, Asian lower blepharoplasties focus on three-dimensional shaping. It aims to create pretarsal fullness, a flat preseptal area, and a volumetric mid-cheek beyond creating a flat eyelid.
Specifically, restoring pretarsal fullness is crucial. Anatomical and cultural differences play a significant role in pretarsal fullness. “Western” patients do not favor pretarsal fullness, whereas Asian patients often undergo procedures to augment this area ( Fig. 15.25 ).

The following six factors are essential in shaping a three-dimensional lower eyelid:
Pretarsal fullness: The pretarsal OOM tone is maintained and its volume reinforced using the preseptal muscle.
Adequate fat treatment: Adequate fat removal, replacement, or reinforcement enhances pretarsal fullness, but avoids overtreatment because of the risk of a sunken eyelid.
Orbital height shortening: The orbital height, which may have increased from aging, by lifting fat in the midface or using a fat graft, is reduced.
Canthal restoration: The lower eyelid will never become three-dimensional in cases of lateral canthal distortion. Therefore, restoration of the normal canthal appearance is essential to shape the lower eyelid.
Rejuvenation: The lower lid is lifted through a suborbicularis oculi fat (SOOF) lift and orbicularis muscle suspension, while fine wrinkles are improved by excision of the remnant skin.
Volume replacement: Even if the lower blepharoplasty was properly performed, the area that was partially lacking in volume could be reinforced with a fat graft or filler injection to create a more three-dimensional shape.
A three-dimensional lower eyelid is created when all of the aforementioned elements are harmonized intraoperatively ( Fig. 15.26 ). Surgically, the steps are as follows:
Incision: A subcilliary incision is made in the mobile skin further below the eyelash, not in the tight skin just below the eyelash, to prevent scar contracture.
Musculocutaneous flap elevation: The skin flap is elevated to expose the pretarsal OOM. The incision should be made in the preseptal portion, not in the pretarsal portion. The facial nerve branch that innervates the OOM is usually located medially ( Fig. 15.27A ). Therefore, when making an incision in the OOM, the medial one-third should be preserved to avoid pretarsal flatness due to denervation ( Fig. 15.27B ).
 Pathway of zygomatic nerve’s branch to medial OOM. AN , Angular nerve; LPB , lower palpebral branch; UmPB , upper medial palpebral branch. (B) Preservation of medial one-third of OOM during lower blepharoplasty.")
SOOF elevation: Dissect from the preseptal area to the level of the inferior orbital rim, and then release the OOM and orbital retaining ligament from the inferior orbital rim. Continue the dissection into the prezygomatic and premaxillary spaces for a SOOF lift.
Fat treatment: After SOOF dissection, fat treatment is performed using fat repositioning, septal reinforcement, or fat removal to correct the orbitomalar groove. At that time, excess removal or repositioning of orbital fat from the orbital cavity can result in a sunken lower eyelid. In contrast, excessive conservative treatment results in insufficient correction and recurrent fat bulging. An adequate amount of fat should be used based on the patient’s upper eyelid status, amount of orbital fat, midface volume, and maxillary protrusion. This process requires a learning curve.
SOOF lift: The fully dissected SOOF is fixed to the inferior orbital rim to reduce orbital height and improve infraorbital hollowness.
OOM suspension: The OOM suspension is a key shaping procedure, which aims to lift, shape, and provide lateral canthal support by lifting the preseptal OOM and suturing it to the lateral orbital rim at the canthal level.
Skin excision: Skin remnants are conservatively excised because adequate skin coverage is important in three-dimensional eyelid shaping. The amount of skin to be excised is measured when the lower lid is tightest (during wide mouth opening while looking upward).

Similar to non-Asian individuals, the following techniques are used to treat aging eyelids in Asian patients:
Brow lift
Suprabrow lift
Infrabrow lift
Upper blepharoplasty
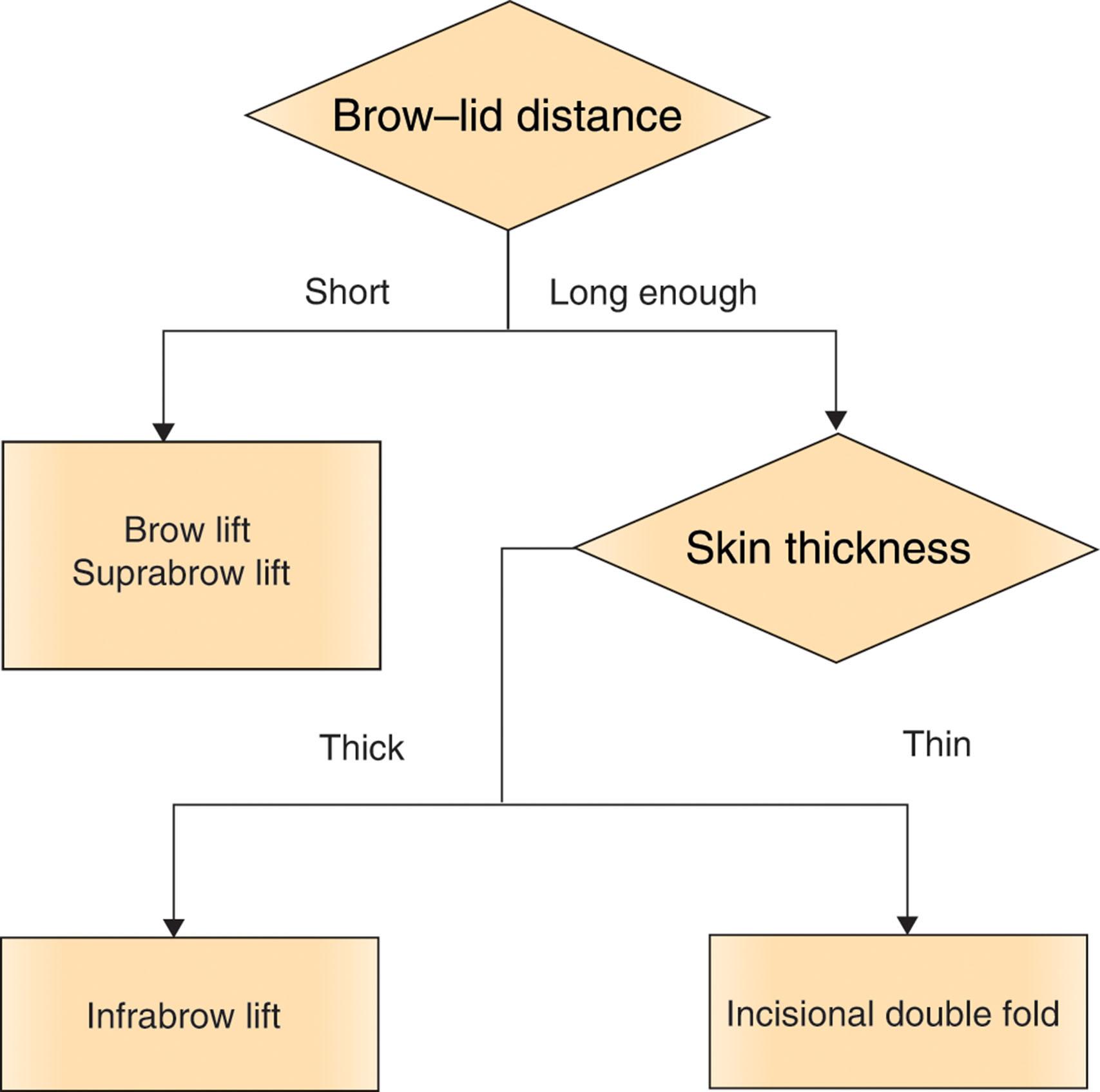
The brow–lid distance and eyelid thickness should be considered when selecting the surgical method ( Algorithm 15.1 ). Rather than using any numerical value as a reference point in the evaluations, determining the appropriate surgical method for each patient through consultation is recommended.
First, the brow–lid distance should be evaluated. Performing upper blepharoplasty in patients with short brow–lid distance results in a shorter brow–lid distance and thicker eyelids, creating strong and stuffy impressions. Therefore, in such cases, brow lift or suprabrow lift is considered first, regardless of eyelid thickness.
If the brow–lid distance is within sufficient dimensions, the method of upper blepharoplasty is determined by evaluating the skin thickness. Incisional double-eyelidplasty can be performed if the skin is thin. The surgical principle of aging double-eyelidplasty is not different from that of general blepharoplasty. It is noteworthy that the sagging skin should not be extremely excised, and fat removal should be performed conservatively. An infrabrow lift is appropriate for thick skin. In this chapter, only the infrabrow lift, which is commonly used as a method of Asian aging upper blepharoplasty, is described in detail.
The upper eyelid thickness varies, depending on the region, with thicker regions closer to the eyebrow. When performing upper blepharoplasty with skin excision, this difference must be considered.
When skin excision is performed during double-eyelidplasty, the thin skin close to the eyelash is excised. Subsequently, the relatively thicker skin forms the upper flap of the double eyelid. In patients with thick upper eyelid skin, this creates a very unnatural and strong-looking double eyelid. Therefore, in patients with thick eyelid skin, skin excision inferior to the eyebrows is more ideal ( Fig. 15.28 ).

However, the infrabrow lift may reduce the brow–lid distance postoperatively, potentially decreasing the effectiveness of the procedure.
Patients with a lot of brow action: Brow action compensatory to saggy skin almost disappears after the surgery, causing brow ptosis.
With simple skin excision only, the upper flap could be pulled lower, causing postoperative brow ptosis.
Thus, to minimize postoperative brow ptosis, techniques that sling the lower flap to the periosteum or frontalis muscles are performed after infrabrow excision ( Fig. 15.29 ).

The goals of Asian rhinoplasty are usually quite different from those of “Western” rhinoplasty. Relative to its Caucasian counterpart, the Asian nose is smaller and shorter, has less tip projection, and a wider nasal base ( Fig. 15.30 ) These differences involving the nasal framework and soft tissue on the nose dictate a unique approach when performing rhinoplasty in most Asian patients. On the other hand, the principles of rhinoplasty apply to all ethnicities when dealing with entities such as the dorsal hump or crooked nose.

In general, the appearance of the nose is quite different between women of Asian and Caucasian origin. Asian nasal skeletons are generally smaller and more delicate ( Fig. 15.31 ). As Asian women have a flat forehead and weak chin, the relationship of the nose with the chin and forehead forms a more obtuse angle. From an aesthetic standpoint, certain geometric characteristics of the nose appear to be present in attractive women. Anthropometric studies have reported the ideal value of the nose in women of different racial origin. Although the general nasal skeleton is bigger in those of Caucasian ancestry, they share certain angular and proportional relationships of the nose with other facial structures. The geometric features of an attractive face should be considered to obtain an aesthetic nasal appearance in Asian patients ( Fig. 15.32 and Table 15.2 ).


| NFrA (%) | NFaA (%) | NMA (%) | NLA (%) | LMA (%) | |
|---|---|---|---|---|---|
| Anthropometry in ordinary young females | |||||
| Choi, Kim et al . | |||||
| Korean | 145.6 | 29.1 | 135 | 88.3 | 143.6 |
| Anthropometry in attractive young females | |||||
| Rhee et al . | |||||
| East Asian (Korean, Japanese, Chinese) | 141.5 | NA | 129.1 | 109.5 | NA |
| Caucasian | 137.9 | NA | 125.6 | 101.8 | NA |
| Burusapat and Lekdaeng | |||||
| Thailand | 142.82 | 39.76 | NA | 104.57 | NA |
| Diverse ethnicity | 138.58 | 43.79 | NA | 112.46 | NA |
| Galantucci et al . | |||||
| Caucasian | NA | NA | 131.12 | 123.12 | NA |
| Choi, Yi et al . | |||||
| Korean | 147.2 | 28.8 | 134.7 | 108.4 | 147.2 |
| Paraguayan | 142.3 | 33.2 | 128.9 | 98.8 | 139.1 |
Rhinoplasty in Asian patients was first reported in 1964 by Khoo Boo-Chai. Following this, Furukawa summarized the important aspects of Asian rhinoplasty in 1974. He reported anthropometric data for the Japanese population, identified the optimal nasal profile for Asian patients, and described unique Asian rhinoplasty techniques. Moreover, he introduced a morphologically diverse set of dorsal silicone implants. In 1986, McCurdy put a convincing argument for aesthetic goals of rhinoplasty that applied to both non-Caucasian and Caucasian noses. Parsa reported nasal augmentation with split calvarial grafts in Asian patients in 1991. Columella lengthening for nasal tip remodeling was reported by Shin and Lee in 1994, and Watanabe studied the alar anatomy of Asian patients in 1994. In 1996, Han and Kang reported prefabrication of nasal implants via curing of silicone adhesive, with satisfactory results in Asian patients. These advancements in our understanding of nasal anatomy and surgical techniques specific to Asian patients allowed for an ever-expanding list of rhinoplasty techniques in the ensuing decades. Many mainstream techniques have been fine-tuned to further improve aesthetic outcomes and decrease complication rates. The management of complicated and/or difficult rhinoplasty cases is now finding consensus among a larger group of rhinoplasty surgeons practicing in high-income East Asian countries.
Surgeons should keep in mind some differences in the desired aesthetic purpose of the patient and surgeon to satisfy Asian patients undergoing rhinoplasty.
Patient’s perspective: Most Asian patients undergoing rhinoplasty desire an augmented dorsum and improved tip projection while controlling tip rotation. As discussed in the Introduction of this chapter, the brachycephalic facial skeletal shape requires anterior projection in terms of facial balance. For this purpose, forehead augmentation, augmentation rhinoplasty, anterior segmental setback ostectomy (ASO), and advancing genioplasty are popular in Asian countries.
Surgeon’s perspective: The surgeon seeks to augment the nasal dorsum and improve tip projection while controlling the tip rotation. The surgeon is challenged by the relatively thick skin and weak nasal framework, which is often seen in Asian individuals. L-shaped silicone implants have often been used in the past but are associated with multiple complications in the long term. Therefore, contemporary Asian rhinoplasty has evolved into the use of autogenous cartilage for nasal tip work, while silicone implants still prevail for dorsal augmentation.
Current trends in nasal tip remodeling in Asian countries are at odds with the classical understanding of nasal tip biomechanics. The tripod theory was first suggested by Anderson in 1969 and is based on the three legs of the paired lateral crus on pyriform apertures and conjoined medial crus on the columella base ( Fig. 15.33A ). However, the use of a septal extension graft and/or derotation grafts suggests that a fourth tensor-stress vector might play a role in determining the position and orientation of the nasal tip. This additional element was discussed in detail by Lamson, who reasoned that the caudal septum provides major mechanical support to the nasal tip. As rhinoplasty is currently practiced in Asian countries, an increasing number of rhinoplasty surgeons appear to be following the “quadripod” concept of the nasal tip, with the anterior caudal septum as the fourth leg, as suggested by JW Choi, who would rather call it “septum-based nasal tip plasty”. These would be the basic steps in Asian nasal tip plasty based on the quadripod theory, which are different from “Western” rhinoplasty ( Fig. 15.33B ).
 Traditional nasal tip tripod theory suggested by Anderson in the 1960s. (B) Contemporary Asian nasal tip quadripod concept based on the septum as a major supporting structure.")
The patient interview and physical examination of the nose should not vary across ethnicities. Nasal analysis is the same for all patients.
Most Asian patients who wish to undergo rhinoplasty have a relatively low nasal dorsum. In recent years, patients have been requesting augmentation of the dorsal contour with a simultaneous increase in tip projection. The height of the nasal dorsum in such patients must be assessed in the context of the entire lateral profile from the forehead to the lip and chin. The thickness of the nasal skin must also be considered, especially if the augmentation requires alloplastic material. The thick soft-tissue envelope offers a robust separation between the implant material and the outside world. However, the thickness of the skin envelope correlates with resistance to tissue expansion, and patients should be counseled on the limitation that thick skin places on implant size and, subsequently, on dorsal profile augmentation.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here