Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

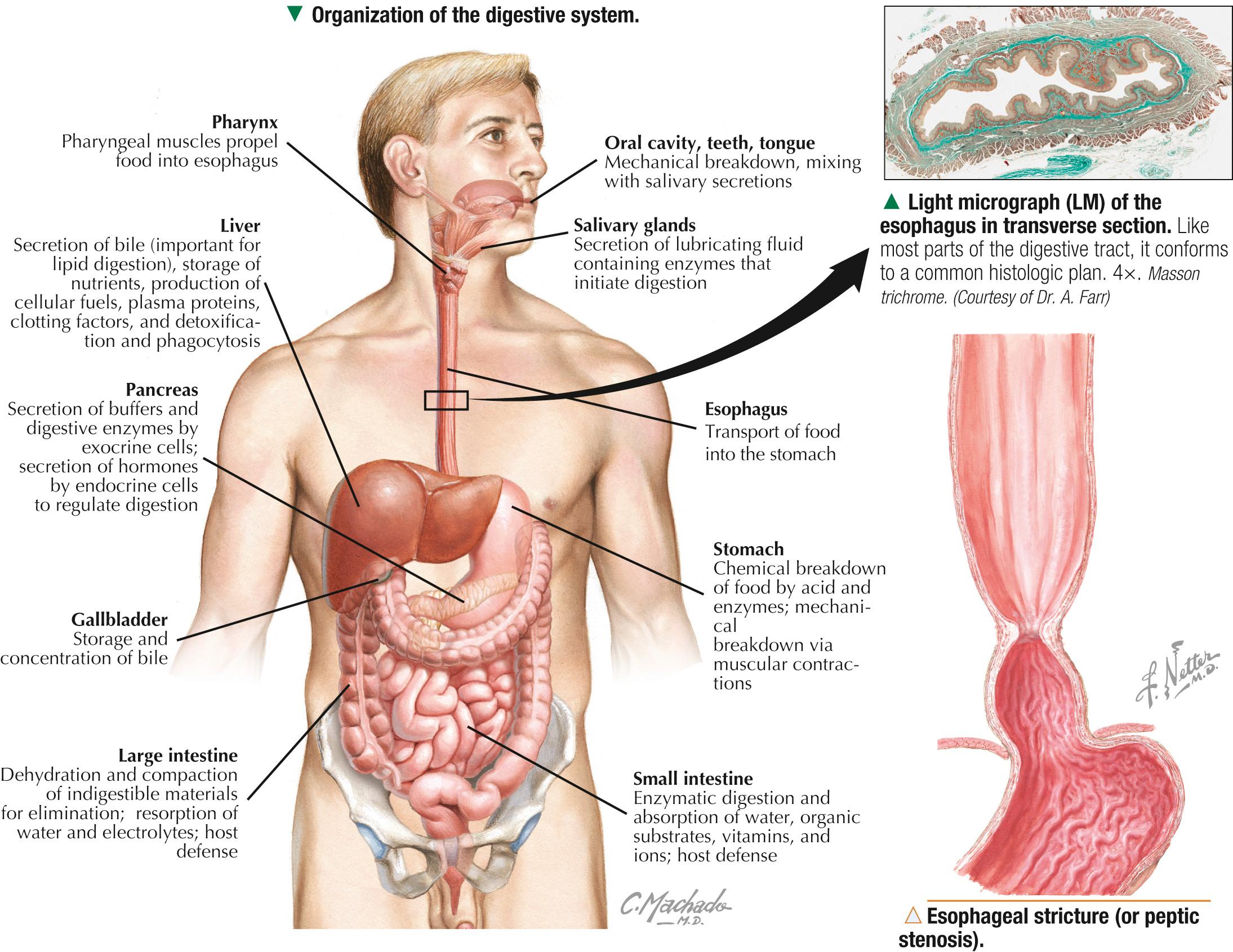
The digestive system—a long, tortuous, hollow tube—comprises the mouth (or oral cavity ), pharynx, and digestive tube or tract (also called the alimentary canal ). Associated with this tract are accessory glands of digestion: salivary glands, liver, gallbladder, and pancreas, which lie outside the wall of the tube but are connected to it via ducts. The digestive system engages in many functions such as propulsion, secretion, absorption, excretion, immunologic protection, and hormone production. For convenience, this system can be divided into upper and lower tracts. The upper digestive tract facilitates ingestion and initial phases of digestion. It includes the oral cavity and associated structures (lips, teeth, palate, tongue, cheeks), pharynx, and esophagus. The lower tract deals mostly with digestion, absorption, and excretion. It includes the stomach, small and large intestines, and anal canal. The microscopic structure of each part of the tract, which is lined internally by mucous membrane, is adapted to reflect functional changes. Mucosa forming the inner lining of the mouth and pharynx is mostly nonkeratinized stratified squamous epithelium and an underlying lamina propria. Submucosa and a subjacent supporting wall, which attaches superficial tissues to skeletal muscle or bone, lie deep to the mucosa. Other parts of the upper and lower tracts conform to a common histologic plan involving four concentric layers (or tunics). A mucosa (or mucous membrane) is adjacent to the lumen. Underlying submucosa is made mostly of highly distensible connective tissue. A prominent muscularis externa consists mainly of smooth muscle oriented in different directions. An outer tunic, the adventitia, is fibrous connective tissue and is known as a serosa in areas in the peritoneal cavity, where this outer tunic is covered externally by peritoneal mesothelium.
Dysphagia —difficulty in swallowing—can occur at any age but is most common in elderly adults. It has many causes; disorders leading to it may affect oral, pharyngeal, or esophageal phases of swallowing. Two major types are cervical ( oropharyngeal ) and thoracic ( esophageal ) dysphagia. Esophageal stricture (or peptic stenosis ) is a common diagnosis in patients with esophageal dysphagia, often resulting from scar tissue formation. Usually a complication of gastroesophageal reflux disease, it may also be caused by esophagitis (inflammation of the esophagus), hiatus hernia, or dysfunctional motility. Diagnostic tests include upper endoscopy , fiberoptic evaluation of swallowing, and barium esophagography .
Lips guard the entrance to the digestive tract as a mucocutaneous junction between the body exterior and digestive system. Each lip has three surfaces: an outer cutaneous part, red ( vermilion ) border, and inner oral mucosa. The outer thin skin is richly innervated with sensory nerves. Like thin skin in other parts of the body, it consists of an epidermis and an underlying dermis with hair follicles, sebaceous glands, and sweat glands. A transitional zone between skin and oral mucosa is the free edge, or vermilion border. Its stratified squamous epithelium is thick and either lacks a superficial layer of keratin or is lightly keratinized. Under the epithelium are tall connective tissue papillae that are close to the surface. The vermilion border is pinkish-red because of the relatively translucent epithelium and the blood in capillaries in the papillae. This border lacks hair follicles and, because it has no glands, is dry.
Carcinoma of the lip is the most common oral cavity malignancy, with almost 95% of cases being squamous cell carcinoma. The lower lip is prone to these neoplasms, usually caused by chronic sun exposure, and middle-aged and elderly men are more susceptible to them than women. Compared with other head and neck cancers, lip carcinoma is readily curable, but sometimes regional metastasis, local recurrence, and death may occur. Treatment involves equally effective surgical excision or radiation therapy, the choice depending on tumor size.
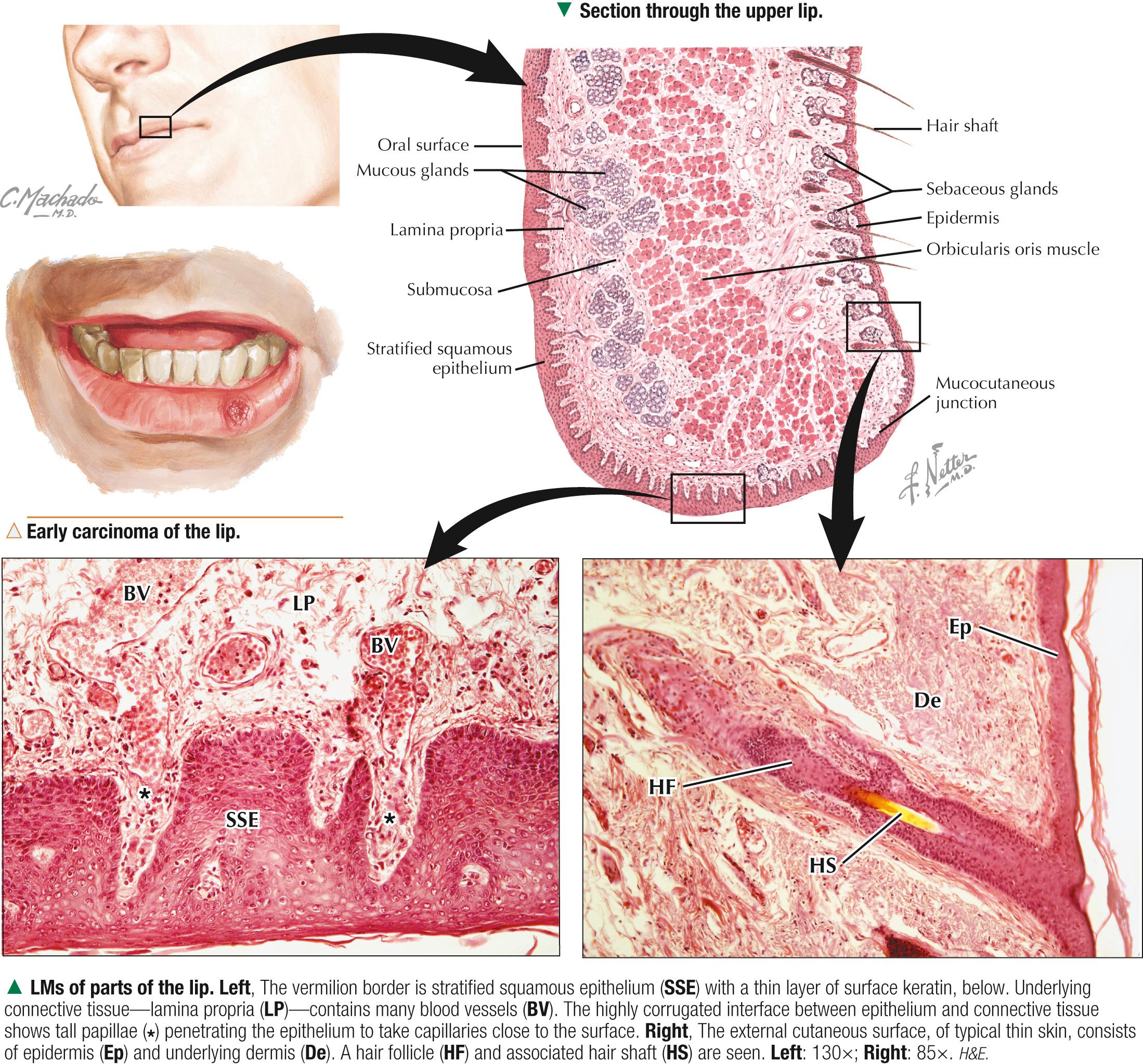
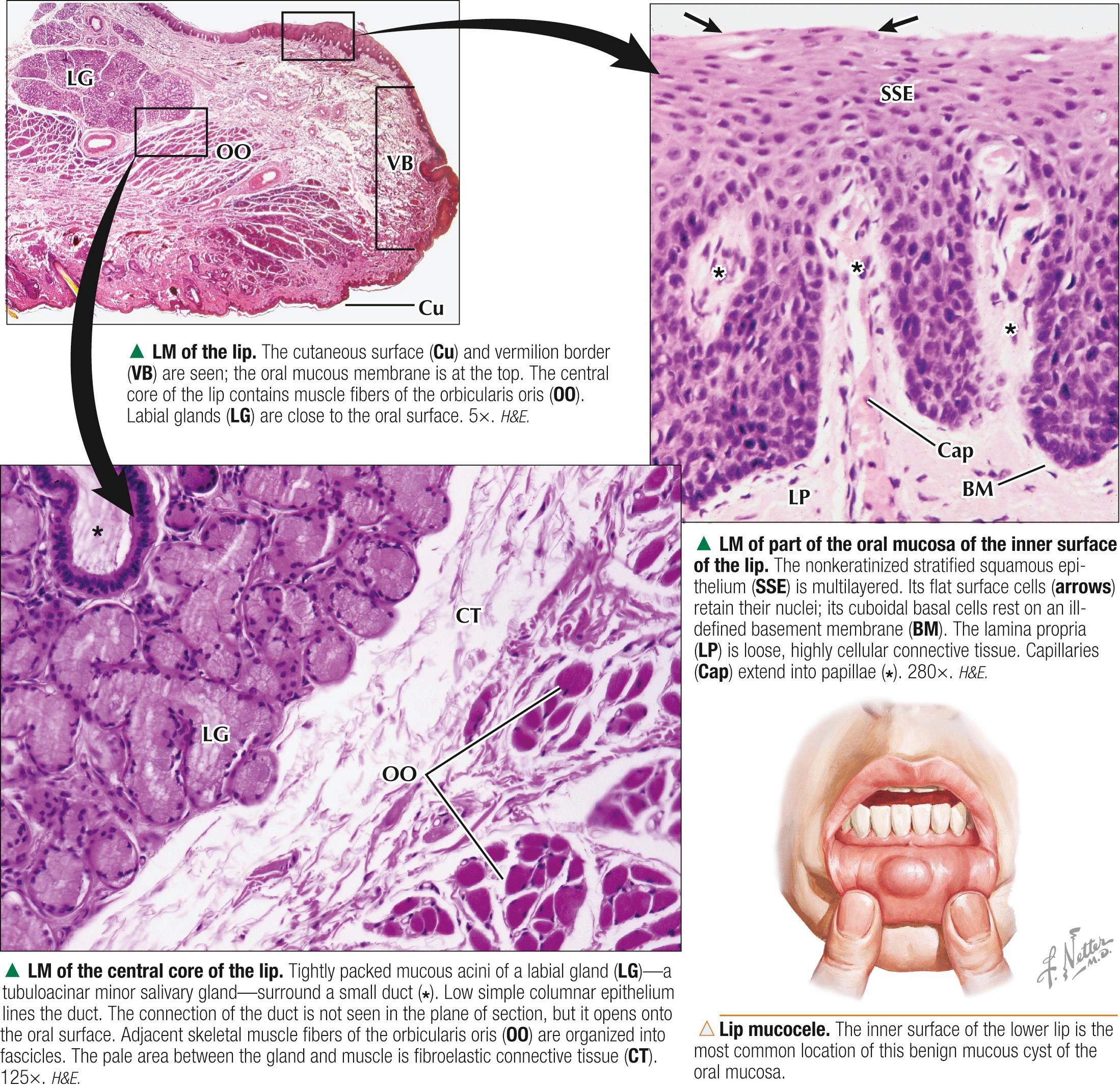
The inner side of the lip is lined by an oral mucous membrane consisting of thick nonkeratinized stratified squamous epithelium and underlying lamina propria of loose, richly vascularized connective tissue that indents the epithelium with papillae. These papillae resemble those under the epidermis but are thinner and more delicate. The highly corrugated interface between epithelium and lamina propria firmly anchors these tissues against mechanical forces such as friction. The lamina propria contains collagen and elastic fibers, which permit distensibility over underlying tissues. It also harbors capillaries and lymphatics plus many lymphocytes and other cells, which aid in immunologic defense against pathogens and irritants in the external environment. Sensory nerve fibers (branches of cranial nerve V) are also abundant. The mucous membrane forms part of the wall of the oral cavity. Surface cells of the epithelium are continuously shed into the oral cavity lumen, the renewal rate of these cells being 12-14 days. As in other epithelia, a basement membrane separates its basal aspect from the lamina propria. Small groups of minor salivary glands, the labial glands, are deep to the lamina propria in the submucosa. Secretions of these mainly mucus-secreting exocrine glands drain onto the oral surface via small ducts, thereby providing moisture and lubrication. The bulk of the lip is made of a central core of skeletal muscle, the orbicularis oris muscle, whose fibers are surrounded by fibroelastic connective tissue.
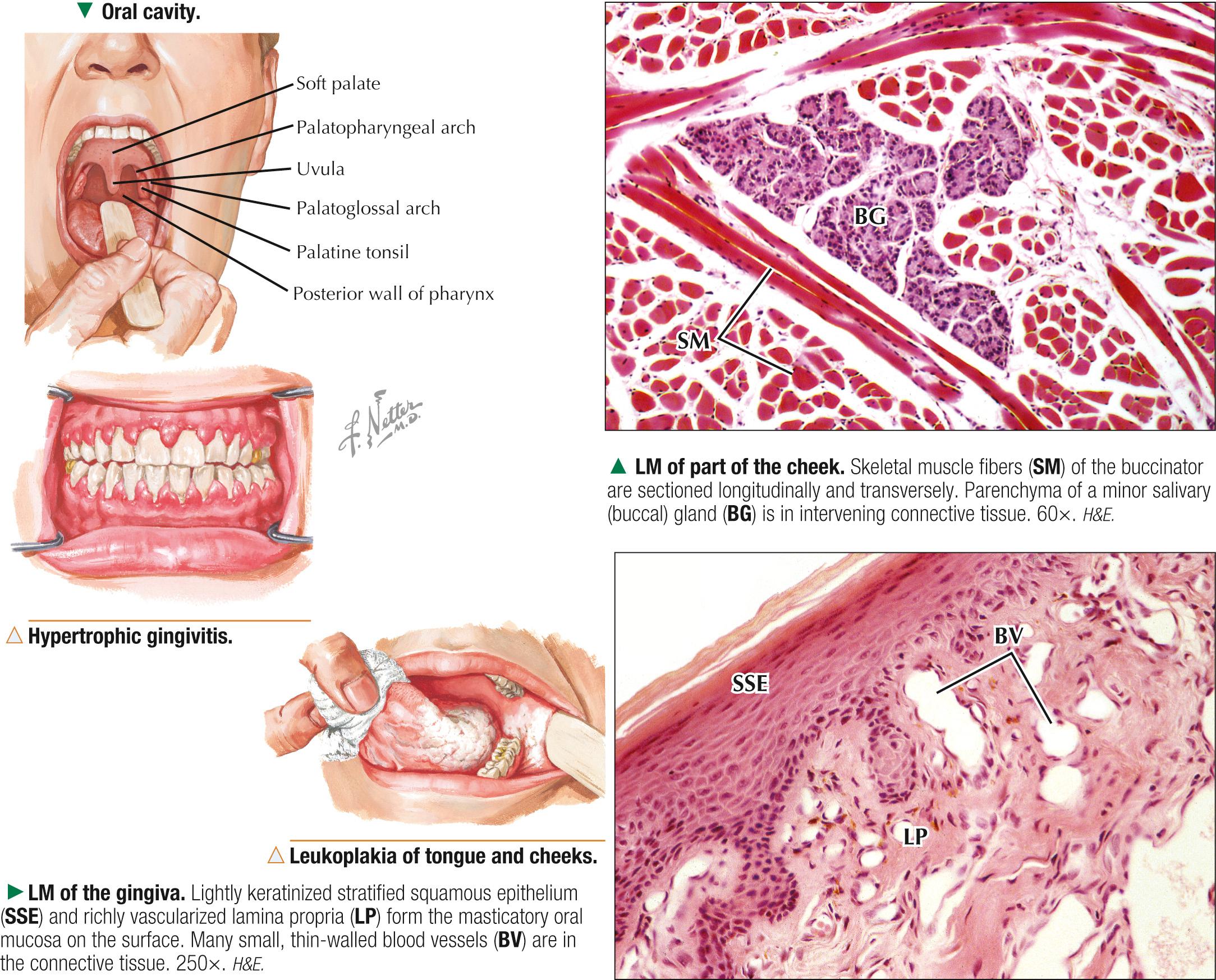
The oral mucosa is regionally modified to reflect differences in function and ability to withstand friction and is classified into three types. Lining mucosa forms the inner lining of the lips, cheeks, soft palate, floor of the mouth, and undersurface of the tongue. It is mainly nonkeratinized stratified squamous epithelium with underlying, supportive lamina propria. Masticatory mucosa consists of stratified squamous epithelium that is lightly keratinized (cells in the stratum corneum retain nuclei). This relatively immobile mucosa is found in gingivae (gums) and hard palate. Specialized mucosa on the dorsal surface of the tongue has many papillae and taste buds. The cheek resembles the lip in histologic features. Stratified squamous epithelium of its mucosa is nonkeratinized. The lamina propria, with short papillae and abundant elastic fibers, attaches at intervals to underlying skeletal muscle fibers of the buccinator. These fibers are arranged into fascicles that mix with minor salivary (buccal) glands. The gingiva, a mucous membrane that lacks glands, covers outer and inner surfaces of the alveolar processes of the maxilla and mandible and surrounds each tooth. Its stratified squamous epithelium overlying a thick, fibrous lamina propria is lightly keratinized on its surface and lacks a stratum granulosum. The lamina propria is firmly anchored to underlying periosteum of the bone, which makes the mucosa immobile and inelastic. The lamina propria extends into deep papillary projections into the base of the epithelium. As in other areas of the oral cavity, papillae contain a large network of capillaries. The epithelium may also be lightly keratinized. It is subject to abrasion during mastication.
Poor or inadequate oral hygiene may lead to inflammation of the gums called gingivitis, the most common dental pathology in children and adults. Gingivitis is usually caused by accumulation of plaque or calculus (tartar), containing large numbers of bacteria. Bacterial invasion of the oral mucosa leads to swelling, irritation, bleeding, and redness of gums. Features of chronic gingivitis include accumulation of plasma cells and B lymphocytes in the lamina propria, plus destruction of collagen. Untreated, gingivitis may lead to more serious complications such as periodontitis. This often involves destruction of the periodontal ligament and alveolar bone, and ultimately tooth loss.
The tongue sits in the floor of the oral cavity. This mobile, muscular organ covered externally by a mucous membrane is divided into two parts. An anterior (oral) two thirds is separated from a posterior (pharyngeal) one third by a V-shaped groove called the sulcus terminalis. The epithelium of the anterior part derives from oral ectoderm, and that of the posterior part, from foregut endoderm. The tongue engages in mastication, swallowing, speech, and taste. Innervation is by four cranial nerves (V, VII, IX, and XII). Smooth nonkeratinized stratified squamous epithelium covers its undersurface and dorsum, except over filiform papillae on the dorsum, where epithelium is parakeratinized. A central mass of intrinsic and extrinsic skeletal muscle consists of interlacing bundles of muscle fibers oriented in three planes. A roughened dorsal surface characterizes the anterior two thirds of the tongue. Three main types of surface vertical projections— lingual papillae —are seen, called filiform, fungiform, and circumvallate papillae because of differences in form. A fourth type— foliate papillae —is not well developed in humans. When present, they are found posteriorly on lateral tongue borders. The posterior third of the tongue lacks lingual papillae, but its dorsal surface is studded by 35-100 irregular mucosal bulges that correspond to lingual tonsils and thus has a cobblestone appearance.
The oral mucosa is the point of entry for pathogens and irritants from the outside into the digestive and respiratory tracts. The clinician must recognize its normal appearance because changes in it are often related to systemic diseases, hormonal states, nutritional deficiencies, and immunologic disorders. Oral candidiasis, presenting as white plaque-like lesions, is a fungal infection in healthy adults. Epstein-Barr virus causes hairy leukoplakia , which consists of white mucosal lesions on the tongue. HIV-positive patients often have these lesions. Repair of oral mucosa in response to disease or infection is much more efficient than that of skin, as there is almost no scar formation after injury.
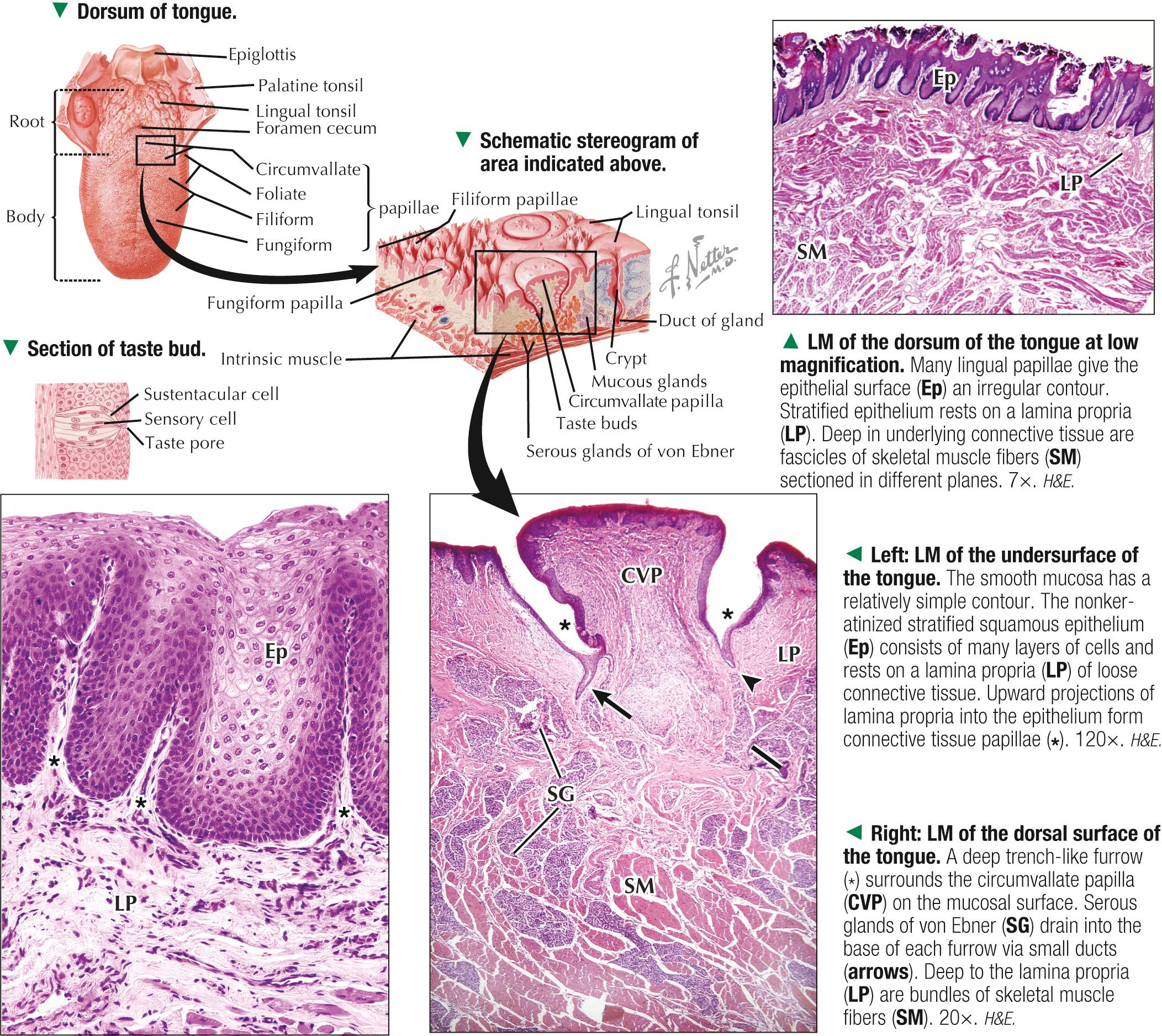
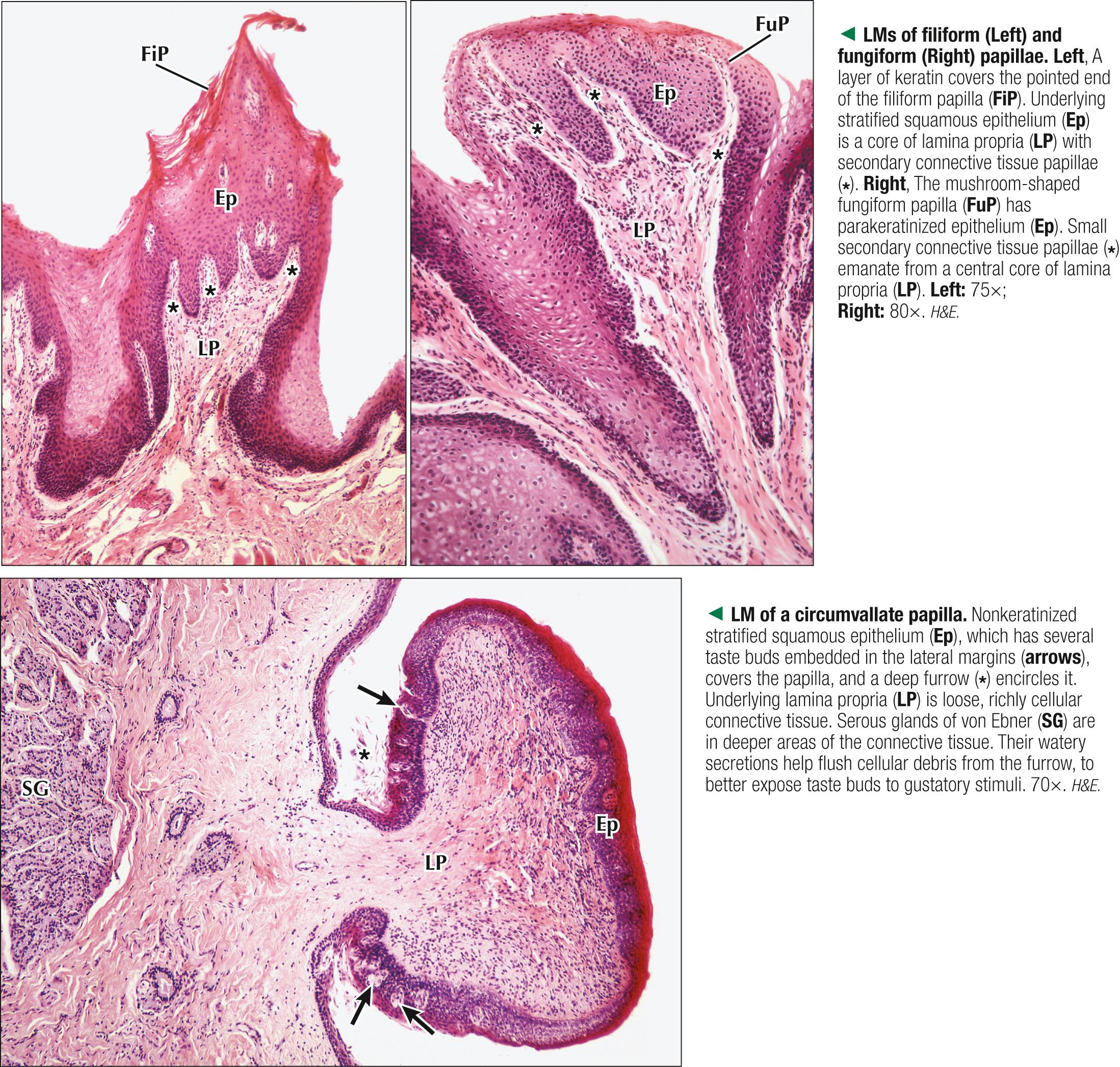
Cone-shaped filiform papillae, the most numerous papillae, are 2-3 mm long and help manipulate food and increase friction with it during mastication. Keratin that covers their pointed ends makes the tongue gray. The primary connective tissue core in each papilla may have small secondary connective tissue papillae. Less numerous, mushroom-shaped fungiform papillae are poorly keratinized and are scattered singly or in small groups between filiform papillae. Most are near the tip of the tongue. Fungiform papillae have connective tissue cores with primary and secondary branches, which are richly vascularized, thus appearing as red spots (visible macroscopically) on the tongue surface. One row of 8-12 circumvallate papillae lies just anterior to the sulcus terminalis. These largest papillae have a diameter of up to 3 mm and are either nonkeratinized or incompletely keratinized. Each is countersunk beneath the surface and is surrounded by a trench-like circular furrow. Serous glands of von Ebner deep in the lamina propria drain via ducts into the base of each furrow, their watery secretions clearing it of debris. Taste buds —small intraepithelial organs—are embedded on lateral surfaces of the epithelium of fungiform and circumvallate papillae (up to 5 and 250 taste buds on one of each type, respectively). Humans have about 5000 taste buds on the tongue plus about 2500 on the soft palate, 900 on the epiglottis, and 600 in the larynx and pharynx. These special sensory receptors transduce chemical stimuli into nerve impulses, which the brain perceives as gustatory sensations.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here