Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

The goals of secondary facial reconstruction span from simply closing a wound to restoring facial function while achieving as close to a normal appearance as possible both in repose and during animation.
To reconstruct a missing part, the “best” option should be employed, and the sequential thought process of a “reconstructive ladder” should be discarded for a “reconstructive elevator” to find the appropriate option.
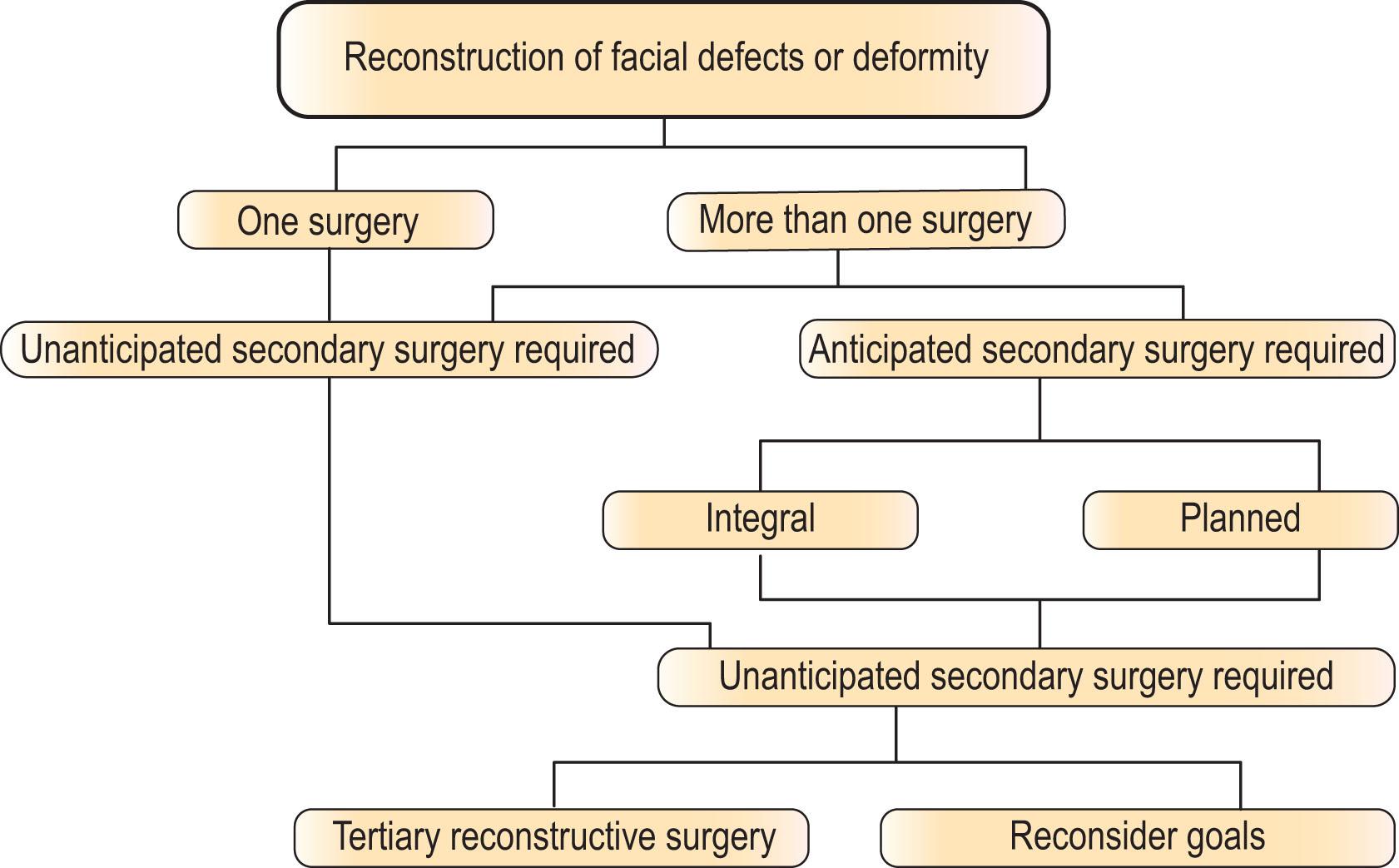
Complex secondary reconstructions are multistage and performed over years and can be divided into anticipated and unanticipated procedures.
Anticipated secondary procedures can be subclassified as integral to the operation or planned to achieve optimal results.
Unanticipated secondary procedures would be having to do an operation to correct a complication or to correct an unanticipated poor or less than ideal result or outcome.
Complex secondary facial reconstruction requires careful assessment and planning, ongoing communication and alignment with the patient, and anticipation and treatment of unanticipated events or complications.
In this chapter we discuss key principles of secondary facial reconstruction and demonstrate them with three clinical case examples.
Facial reconstruction is one of the plastic and reconstructive surgeon’s biggest challenges due to the unique function of the associated anatomy. The face is the interface through which people interact with the world. It provides orifices for stimulation of cranial nerves that allow for the sense of smell, sight, taste, hearing, balance, and equilibrium. It also serves several critical functions including eye protection, airway patency, ability to swallow and speak, and perhaps most importantly, to look human, with the capacity to show expressions of mood and emotions. The goals of facial reconstruction may span the spectrum from simply closing a wound to restoring the functions listed above while achieving as close to a normal appearance as possible both in repose and during animation. The ideal goal would be for the casual observer not to notice that there was ever a defect, deformity, or reconstructive surgery. It is difficult to be able to achieve this goal, and rare to be able to do it in one operation, especially if the defect or deformity is complex and requires transfer of distant tissue.
In this chapter, we discuss principles of secondary facial reconstruction, broadly dividing procedures into anticipated and unanticipated secondary procedures. Anticipated procedures can be subclassified as integral or planned. “Integral” procedures would be techniques that require more than one operative stage to complete. Placing a tissue expander, by definition is at least a two-stage procedure with the second stage fundamental to the process. Another classic example of where a second stage is vital to success is the transfer of a paramedian forehead flap, where the division and insetting of the pedicle is integral to the initial transfer. “Planned” secondary procedures would be recognizing subsequent steps that may be required to obtain an optimum result and, although desirable, are not absolutely linked to it. An example of a planned secondary operation is closing a wound with a flap and then secondarily thinning or resurfacing it. “Unanticipated” secondary procedures would be having to do an operation to correct a complication or to correct an unanticipated poor or less than ideal result or outcome. Sometimes unanticipated secondary procedures are performed because of a misdiagnosis or unforeseen deformity that was only unmasked or became obvious after the initial procedure.
Patients may present prior to extirpative surgery in anticipation of a defect that will likely require multistaged reconstruction to re-establish form and function. Alternatively, patients may present after a traumatic injury or after having undergone reconstructive procedures that, whether from complications or just poor outcome, were unable to satisfy patients goals and expectation.
Patient complaints vary and may include, among others: contour deformity, asymmetry, color mismatch, diplopia, ectropion, oral incompetence, trismus, nasal obstruction, or chronic infection of soft tissue, bone, foreign body, or spaces (such as sinuses or “dead space”).
Reconstructive goals vary depending on the patient’s defect and deformity, comorbidities, psychodynamics, and their goals and expectations. A distinction should be made between closing a wound and reconstructing a part. In certain instances, the goal of a procedure is to close a wound, such as in the case of trying to minimize operative time on a patient with severe medical comorbidities, or to temporize until definitive reconstruction can be planned and executed. In these cases, the simplest and fastest option should be utilized by ascending the wound closure ladder. In other cases, however, the goal is to reconstruct a part. In these instances, the “best” option should be employed, and the sequential thought process of a ladder should be discarded. Rather we should utilize the “reconstructive elevator” to take us to the most appropriate option, no matter how complicated, to allow us to reach our reconstructive goal. When this involves transferring distant tissue, it invariably requires planned secondary surgery. Analogous to a master chess player anticipating multiple moves in advance, or the builder who always builds the foundation before the walls and roof of a building, the reconstructive surgeon should anticipate and plan forward. In his foreword to Gillies and Millard’s textbook The Principles and Art of Plastic Surgery , Webster aptly quotes Aristotle, who says “art, indeed, consists in the conception of the result to be produced before its realization in the material”. He then goes on to explain that the reconstructive plastic surgeon, as the artist, must not only be able to conceive the end result to be produced, but they must also be able to visualize all the necessary steps leading to that end and must have the imagination, intelligence, and dexterity to bring about that result.
Depending on the circumstance, secondary facial reconstruction may need to start with controlling any infection, debriding compromised tissue, and recreating the defect before closing the wound and building a foundation during the first steps. Planned soft-tissue contouring or resurfacing is generally performed at subsequent operations.
When patients present for consultation to discuss unplanned secondary, revisional surgery, it is important to allow them to clearly articulate what they do not like, their concerns, and their personal goals of reconstruction. As plastic and reconstructive surgeons, it is often easy to identify and point out deviations from an ideal aesthetic and suggest improvements. A seemingly unsightly scar or asymmetry may be glaringly obvious to the plastic surgeon, but the patient may not be bothered by it or vice versa . So, allowing a patient to vocalize their thoughts and goals up front both helps identify areas to be addressed and continues to build the physician–patient relationship. Taking standardized pre- and postoperative photographs is recommended both for documentation and as a visual aid when discussing surgical plans with patients. Asking to view (or being asked to view) photographs of patients’ normal appearance prior to their deformity or previous surgery can be a double-edged sword. On one hand it may be helpful to the surgeon in planning, but on the other one must be careful that the patient does not infer that by viewing old photos the surgeon is implying that they can recreate the patient’s pre-deformity state. The expectations of the patient should be synchronized with what the surgeon believes they can realistically accomplish. The key is getting the patient to incorporate their new look (or anticipated look) positively into their body image.
Patient evaluation should include a thorough and systemic assessment of any defects or deformities present or anticipated. This should include:
Extent (or anticipation) of defect or deformity and determination if it crosses aesthetic units
Anatomical layers missing or deformed (skin, fat, muscle, cartilage, mucosa, and/or bony support)
Distortion of mobile parts
Location and quality of any scars
Location of natural boundaries between subunits and rhytids in repose and animation
Comparison to normal unaffected side (if available) and comparison to midline (point out that no face is symmetrical)
Full facial nerve exam, including evaluation of symmetry in repose and animation and notation of any functional deficits
Skin characteristics of patient (including color, texture, quality, pliability, contour, composition, and hair distribution)
Location and any loss of hair-bearing areas, including hairline, sideburns, eyebrows, and mustache/beard areas
Deeper tissue characteristics, including subcutaneous volume, muscular function, and bony structure and contour
Any defects in specialized lining, including eyelids, nasal or oral mucosa, lips
Radiation changes – soft tissue or bone.
This evaluation should include an evaluation of the patient’s mental attitude and emotional state. This should include:
Assessment of level of anxiety
Ability to have realistic expectations
Acknowledgement and acceptance that the process will take a long time and will frequently require multiple stages
Acknowledgement that their deformity may look worse during the intermediate stages
Acknowledgement and acceptance that perfection is rarely accomplished.
Secondary facial reconstruction may be indicated for a variety of possible reasons. These can fall into two broad categories: anticipated procedures and unanticipated procedures. Within the category of anticipated procedures, we can further categorize procedures as those that are integral to the surgical plan (e.g., a second-stage division of a pedicled forehead flap) versus those that are unplanned due to complications, new findings, or less than ideal outcomes (e.g., ectropion repair after lower eyelid reconstruction) ( Algorithm 14.1 ).
For patients presenting after extirpative surgery, or with an existing deformity, one must counsel patients on the reconstructive options available to them based on what is seen on physical examination. However, for many patients presenting with recurrent cancer, the final extirpative surgery has not yet been performed. In these cases, one must counsel patients on what we anticipate the defect or deformity may be and what reconstructive options are available. This discussion is inherently limited as the final deformity may be much smaller or larger than initially anticipated, so it is important to have counseled patients on this and have thought through reconstructive plans for a range of options.
When discussing revisions, it is critical to be frank and grounded in describing anticipated postoperative outcomes. This can be difficult, particularly for the young reconstructive surgeon, especially when keeping realistic expectations for both patient and surgeon. Overpromising results and likely changes can lead to disappointment for both parties.
One must also consider the psychology of both patient and surgeon when embarking on secondary facial reconstruction. Patients’ self-perception can vary widely from feeling completely disfigured to feeling close to normal, regardless of the magnitude of their defect or deformity. Surgeon psychology can also vary depending on level of training and comfort with certain procedures, and whether the patient presenting is a surgeon’s original patient or another surgeon’s patient presenting for revisions. Taking care of one’s own complications or less than ideal outcomes is humbling and can make a surgeon feel defeated. One should remember that facial reconstructive cases are incredibly challenging, and most patients will require repeat surgery at some point, even if unanticipated. On the other hand, operating on a patient who had their index reconstructive procedure with another surgeon poses different and additional challenges. Prior operative reports are not always available, and one may need to rely on what is seen on physical examination to deduce what was previously done.
Having candid discussions about expectations can help keep the patient and surgeon on the same page. Secondary facial reconstruction can often span several stages and is pursued over months and years, so open communication between patient and surgeon is critical to maintain a healthy relationship and help both achieve their reconstructive goals.
By the mid-nineteenth century reconstructive surgeons had mastered numerous local flaps and grafts to close wounds and reconstruct parts of the face. Other than the ancient forehead flap of Sashruta (brought to Europe at the end of the eighteenth century), and the arm flaps of the Branca family and Gaspare Tagliacozzi in the fifteenth and sixteenth centuries, there was no means to bring a large volume of tissue to the face until the latter half of the nineteenth century when the multistaged (waltzing) pedicle flap was developed to transfer distant tissue to the head and neck. Although one-stage island flaps were described by Gersuny in 1887 and Monks in 1898, the multistaged tubed-pedicle flap became popular after independent descriptions by Filitov and Gillies in 1917. Their modification of “tubing” the pedicle of the multistaged (waltzing) pedicle flap decreased inflammation and infection and improved the reliability of this transfer technique. The tube pedicle flap went on to be the workhorse for reconstruction for more than three to four decades. It was not until the 1950s that the initial description of a musculocutaneous flap became popularized for head and neck reconstruction. In 1963, Bakamjian describes a single-stage reconstruction of a palate with a sternocleidomastoid flap. Two years later, he described the versatile multistaged deltopectoral flap that revolutionized head and neck cancer reconstruction. In 1967, Fujino, in studying the circulation of the skin, describes the importance of perforator vessels for flap viability, a concept that seemed to go unnoticed for two decades. The next major advance in pedicle flap development for head and neck reconstruction was Ariyan’s description of the pectoralis myocutaneous flap. Meanwhile, the 1960s and 70 s witnessed the birth of clinically relevant reconstructive microsurgery for head and neck reconstruction throughout the world. These newer concepts and techniques mostly relegated the tube pedicle flap to the history books.
It is interesting that in the early twentieth century there were admonitions by Esser of those that would transfer a tubed pedicle flap and not perform secondary procedures to refine it. Similarly, in the latter part of the twentieth century, McDowell admonished microsurgeons for transferring “indistinguishable globs and blobs of transported tissue” to the face without appropriate secondary procedures. Fortunately, this era of amazement (that the flaps lived) advanced to the era of refinement.
Later in the twentieth century, facial reconstructive techniques and concepts such as aesthetic subunits and use of cartilage and bony framework were developed by plastic surgery giants including Gilles, McIndoe, Gonzalez-Ulloa, Burget and Menick. As improvements continue to be made in the understanding of various soft tissues of the body in terms of color, texture, pliability and three dimensional structure, the breadth of techniques available to facial reconstructive surgeons continues to grow. Today, a variety of techniques may be employed to achieve patient and surgeon’s goals.
More recently with advances in immunosuppression, vascularized composite allograft face transplant has emerged as a possibility for select patients with devastating facial injuries, typically from trauma or burns, that would otherwise not be possible with autologous options. The same principles continue to govern all reconstructive efforts including restoring facial form and function.
Specific technical procedures are individualized to each patient and their reconstructive needs. In 1957 Sir Harold Gillies described the principles of plastic surgery. Many of these original key principles continue to guide reconstruction today, and the overriding principle that “plastic surgery is a constant battle between blood supply and beauty” is as relevant today as it was 100 years ago. Below is a modern interpretation of many of these concepts and principles and a few added thoughts:
Observation is the basis of surgical diagnosis . It is important preoperatively to point out to patients that the shape of most faces is not symmetrical and that there is typically a straight side and a rounder side. That being said, it is important to strive to restore symmetry and maintain three-dimensional contours of facial parts such as the eyes, nose, and lips.
Diagnose before you treat . Determine if tissue is missing, mispositioned or distorted. Is the existing tissue compromised by scar or radiation? Is there an underlying infection of soft tissue or bone? Do you have a quantitative tissue biopsy culture if concerned about infection? Be careful to not be misled by modern technological rendition of anatomy such as three-dimensional computed tomography (CT). While this technology is a very helpful aid for reconstructive planning, it is generally not detailed enough for most diagnostic purposes.
Make a plan and then a pattern for the plan . Utilize templates whenever possible. Ideally templates should be three-dimensional with the approximate thickness of tissue required. With pedicled perforator-based flaps, plan where the pivot point of rotation will be as you consider the design of the flap. With free tissue transfers think about location of recipient vessels, the length of pedicle, and potential need for vein grafts.
Make a record . Take standardized pictures preoperatively and postoperatively and publication-quality pictures intraoperatively. Be sure get a written consent for your photos as publishers require them even if there are no distinguishing features in the image.
Mark patients while awake and upright when possible . Mark the midline and borders of aesthetic units as well as any rhytids and lines of animation. Mark the contralateral normal side (if available) in addition to the operative side.
Tattoo key landmarks . Use methylene blue to temporarily tattoo important landmarks, delineate sinus tracts and facilitate debridement of complex wounds.
Always have a lifeboat . Assume something may always go wrong and have a back-up plan. Pedicled perforator flaps can be limited in movement by the key perforator, flaps may not fit the entirety of a defect, vessels clot, tissue dies, etc.
Replace what is normal in normal position and retain it there . Release scar contractures that distort adjacent tissue. Utilize Z-plasties to break up lines of tension.
Hide scars within aesthetic lines between subunits or within existing rhytids . If this is not possible, break up the scar with an irregularly irregular closure or utilize micro Z-plasties in series to help camouflage them.
Create early structural support . Use structural support (ideally vascularized) early in the sequence of reconstruction to build from a stable foundation to support soft tissue and prevent its collapse.
Losses must be replaced in kind . Replace “like with like” whenever possible. Replace missing thin pliable soft tissue with thin pliable soft tissue; replace thick skin with thick skin; replace bone with bone; replace hair-bearing skin with hair-bearing skin, etc. Gonzalez-Ulloa exploited this principle with his description of the aesthetic units. This concept was not only to define the best location to put seams between grafts or flaps, but also pointed out that the skin of each unit was unique with different qualities, thickness and composition.
Never throw anything away – until you are sure you do not want to use it for fill, support, or resurfacing. That being said, consider reconstructing entire aesthetic units or subunits when able, even if that means excising some normal tissue to complete the unit or subunit defect.
Free flaps are frequently easier to do than local flaps . Typically, they can be harvested simultaneously with extirpation or preparation of the recipient site. Size, shape, and composition of tissue types can be individually tailored to that which is lost. Insetting is almost always easier with a free flap.
Do not hesitate to use vein grafts . There is no negative impact on success if planned preoperatively.
Never let routine methods become your master . Chimeric flaps provide customizable tissue components with more precise inset into complex defects.
Consider color match . When skin is included in a distant (free) flap, the color is invariably different from the recipient site. Avoid having a patch of skin with different characteristics (color, texture, composition) on the face. Use local flaps for the best color match. If no local options are appropriate or available at the initial reconstructive stage, think about improving the color match by secondarily resurfacing with a local/regional flap or regional skin graft at a subsequent procedure.
Surgical aftercare is as important as the planning . Gillies’ admonition of “how futile it is to lose a flap or graft because of inadequate or the lack of postoperative monitoring or care especially during the first 48 hours after operation” rings true today, particularly for free flaps.
Expect revisions . To obtain a satisfactory contour, optimize outcomes, and minimize unfavorable results, one must be prepared to perform minor revisions, such as hardware removal, soft- or hard-tissue contouring, local tissue rearrangements, or use of liposuction or fat grafting to thin or augment areas as needed (fat can be added or taken away).
Beware of thinning too aggressively or too soon . Swelling may take up to 2 years to resolve after which the tissue typically tightly adheres to the contours to the underlying structural support – a phenomenon that we call “shrink wrap”.
Beware of delayed secondary elastic recoil of tissue-expanded flaps, particularly when used near mobile parts . Consider the use of tissue expanders in areas adjacent to a flap rather than under the flap itself. This utilizes the expanded area for flap donor site closure and eliminates the secondary contraction that frequently occurs with expanded flaps.
Palliative treatment frequently requires more extensive surgery than primary reconstruction . To ensure primary healing and minimize postoperative wound healing problems, ideally all radiated, infected, and/or scarred tissue needs to be removed, often leading to a large complex wound. This then requires transfer of very large flaps. Trying to limit the surgery for palliation often leads to wound breakdown and a more symptomatic patient then prior to initial surgery.
You cannot fix an asymptomatic patient . If a deformity does not bother a patient, do not try to improve it.
There is no risk like no risk . Virtually all patients undergoing secondary surgery have complications. The risk-averse patient should think twice about “elective” surgery.
Most patient negative satisfaction issues stem from missed perceptions and unrealistic or inaccurate expectations . It is incredibly important to try to understand the patient’s psychodynamics, particularly regarding perception of themselves (how they look, how they perceive others see them) and their expectations. In multistaged reconstructive planning, the patient needs to understand that during the intermediate stages, they may look worse before you can make them look better.
Describing the multitude of techniques that may be employed for secondary facial reconstruction is beyond the scope of this chapter. Instead, we present some representative cases that highlight some of the principles of secondary reconstruction and issues that may arise.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here