Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

The maxilla may be thought of as a six-walled geometric box.
Most extensive midface defects require free flaps for reconstruction.
Complex structures such as nose, eyelids, and lips should be reconstructed separately, usually with local flaps.
Understanding the defect, especially the bony structure and soft-tissue elements that need to be restored, is key to successful midfacial reconstruction.
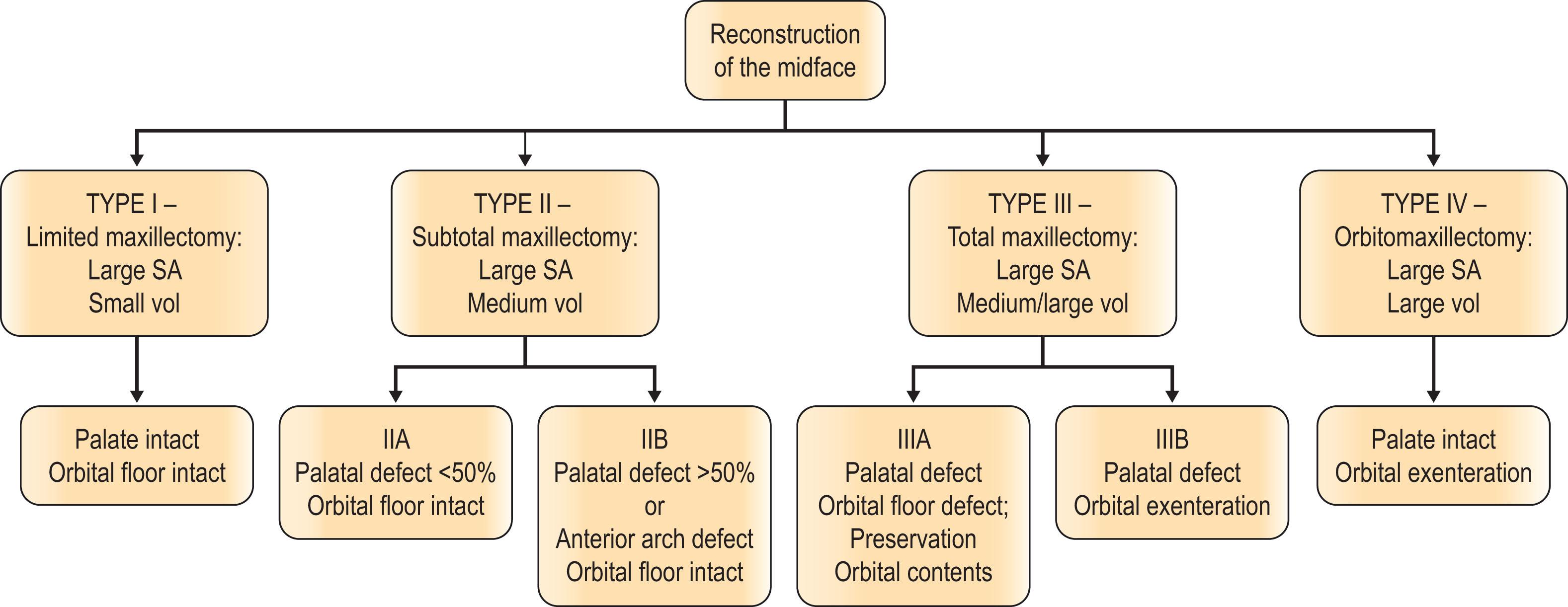
The classification of midface defects is based on the extent to which the maxillary bone has been resected.
Those defects that approach or exceed 50% of the transverse palate and alveolus usually need osteocutaneous free flap reconstruction for dental implant placement.
Accurate orbital floor reconstruction is necessary to avoid visual complications, and grafts and alloplasts should be covered by well-vascularized flap tissues to prevent infection and exposure.
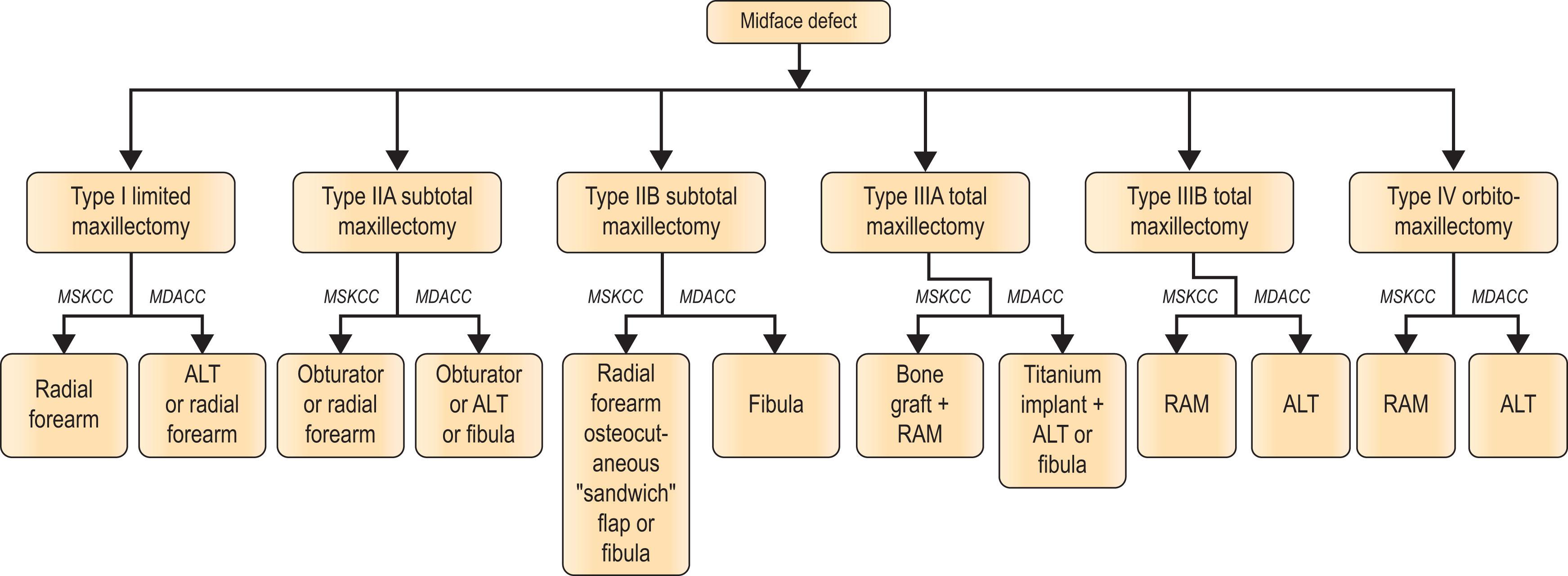
We present treatment algorithms of our two centers that are based on understanding the flap surface area to volume ratio needed for optimal reconstruction.
Access video lecture content for this chapter online at Elsevier eBooks+ 
Reconstruction of the midface starts with a clear understanding of the complex three-dimensional anatomy of the maxilla. In basic terms, the maxilla may be thought of as a six-walled geometric box that includes the roof of the box, which is the orbital floor, the floor of the box, which is half of the anterior hard palate and alveolar ridge, and the medial wall of the box, which forms the lateral wall of the nasal passage ( Fig. 9.1 ). The maxillary antrum is contained within the central portion of the maxilla. The cranial base overlies the posterior pterygoid region of the maxilla. The two horizontal and three vertical buttresses provide facial height, width, and projection. The overlying soft tissues, including the muscles of facial expression and mastication, insert on the maxilla and are responsible for individual facial appearance and function.

The goals of reconstruction are functional and aesthetic. Most extensive midface defects require free flaps for reconstruction, with flap selection dependent on the amount of resected skin, soft tissue, and bone. Complex structures such as nose, eyelids, and lips should be reconstructed separately, usually with local flaps.
The classification of midface defects is based on the extent to which the maxillary bone has been resected ( Algorithm 9.1 ). Once the bony defect is assessed, the soft-tissue defects, including cheek skin and palate, are addressed. If facial structures such as the nose, eyelids, and lips are involved, they are reconstructed separately, usually with local tissues using methods described elsewhere in this text. A treatment algorithm based on flap preferences of the authors (Peter G. Cordeiro, Memorial Sloan-Kettering Cancer Center and Matthew M. Hanasono, MD Anderson Cancer Center) is summarized in Algorithm 9.2 and discussed in detail below. By following an algorithm based on a clearly delineated classification system of midfacial defects, even patients with very large, complex defects can be restored to good function.
Type I, or partial, maxillectomy defects are those that involve one or two walls of the maxilla, most commonly the anterior and medial walls ( Fig. 9.2 ). Both the palate and the orbital floor remain intact. The resection may include the soft tissue and skin of the cheek, and even the lips, nose, and eyelids. Occasionally, the orbital rim will be resected and non-vascularized bone grafts will be necessary for reconstruction. Type I maxillectomy defects are small-volume deficiencies with large surface area requirements, often needing one or two skin islands. Our flap of choice is the radial forearm fasciocutaneous free flap, as it provides good external skin coverage and minimal bulk while allowing multiple skin islands that can be de-epithelialized to improve contour, wrap around bone grafts, and supply lining for the nasal cavity ( Fig. 9.3 ).


Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here