Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Fingertip and nail bed injuries are the most common injuries of the hand.
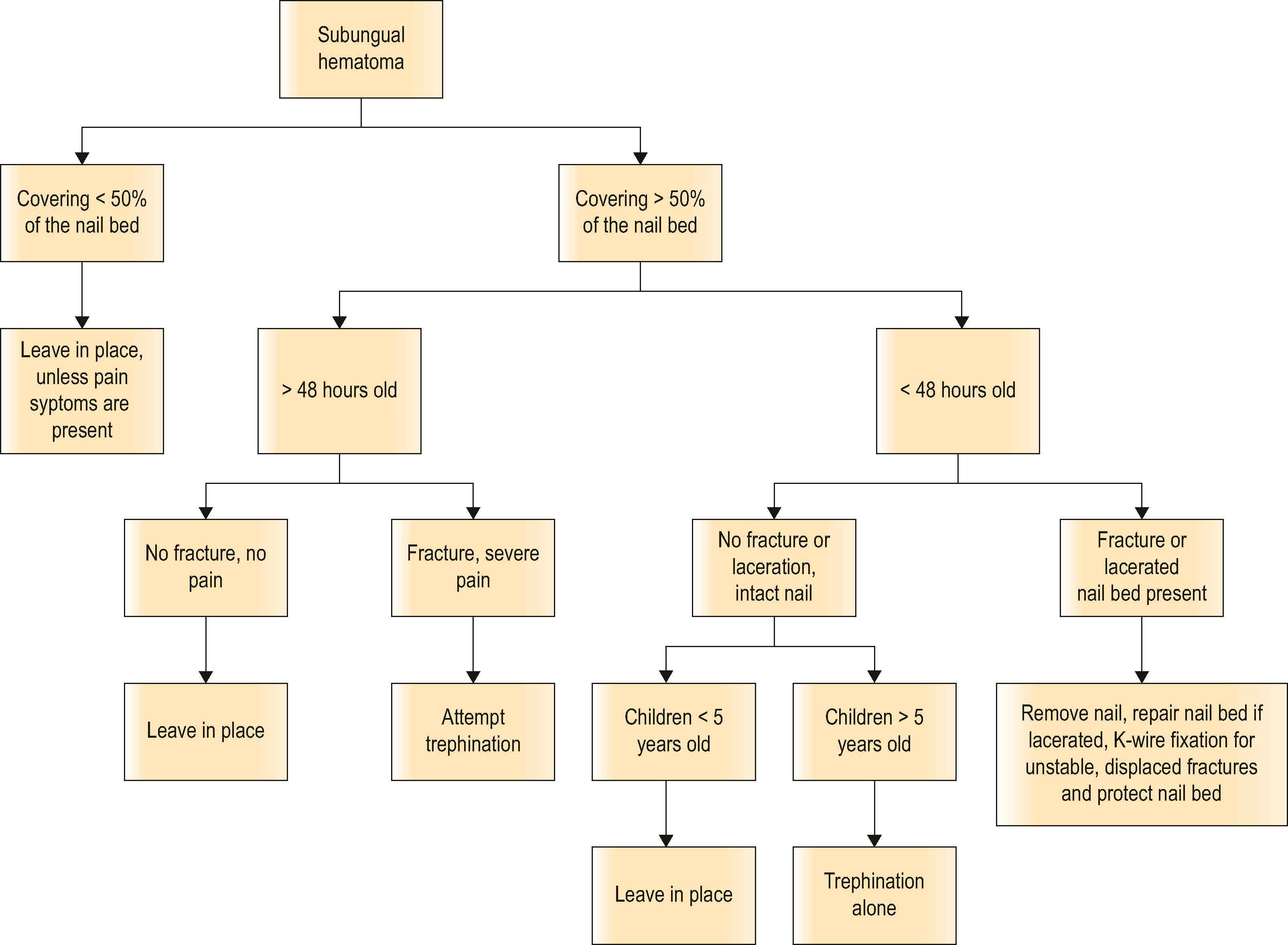
Large subungual hematomas should be drained to relieve pressure and pain; small and asymptomatic hematomas (<50%) can be observed. Trephination of a subungual hematoma is performed to relieve the throbbing pain associated with this injury.
When the nail plate is intact, not all nail bed lacerations need to be repaired.
Common secondary nail deformities seen after nail bed injury include nail ridging, splitting, nonadherence, absence, cornified nail bed, hook nails and spikes, or nail cysts.
Knowledge of the anatomic arterial branching patterns of the fingertip allows creation of flaps to preserve length after distal fingertip amputation injuries, including the volar and lateral V-Y advancement flaps.
In the appropriate patient, subungual melanoma in situ can be safely treated without amputation.
The purpose of the current chapter is to provide the reader with a comprehensive review of the pathophysiology, diagnosis, and treatment of nail and fingertip injuries and their management.
The fingertip serves many functions in our everyday interactions with the world. The sensation provided by the complex unit of the highly specialized immobile, glabrous skin and soft-tissue pulp with the rigidity and counter pressure created by the distal phalanx, nail plate and nail bed produce tactile feedback allowing detailed sensation, proprioception, and fine object manipulation. The perionychium consists of the nail bed, nail fold, eponychium, paronychium, and hyponychium. The perionychium is the most frequently damaged region of the hand due to the prominence of the nail on the tip of the finger. Embryologically, these structures develop near the end of the first trimester as a thickened area of epidermis on the dorsal distal phalanx of each finger and toe that proximally invades the underlying dermis to form the nail groove. The deep layer of epidermal cells proliferates to form the nail matrix. Cells within the superficial layer of the nail matrix differentiate into hard keratin, forming the nail. At approximately 14 weeks, proliferation of the deeper layers of the nail matrix pushes the nail distally across the nail bed while firm attachment is maintained between the nail and nail bed. Folds of epidermis lateral and proximal to the developing nail form the nail folds. Nails reach the tips of the fingers and toes at about 32 and 36 weeks of intrauterine life, respectively.
The topography of the nail was first described by Zaias in 1963. In this landmark study, fingers and toes of human embryos from 9 weeks to full term were sectioned and examined, and the development of the human nail was detailed. This paper began to clarify terminology of nail structures and embryology with a glossary of various fingernail structures. Later, in 1980, a standardized nomenclature for the anatomy of the nail was proposed by Zook et al . to improve communication between physicians regarding nail pathology, injury, and treatment ( Fig. 6.1A,B ). The entire nail structure, including the nail fold, paronychium, hyponychium, nail bed (germinal and sterile matrices), and nail, is referred to as the perionychium. The paronychium refers to the lateral skin surrounding the nail bed and nail. The skin over the dorsum of the nail fold is referred to as the nail wall. Extension of the nail wall distally onto the dorsum of the nail forms the eponychium. The eponychium is attached to the nail by a cornified material known as the nail vest, or cuticle. The white, convex opacity extending distally from beneath the eponychium is the lunula, which is the distal visible extent of the germinal matrix. The white color remains after removal of the nail and is thought to be secondary to retention of nuclei of the germinal cells to this level in the nail. The mass of keratin beneath the distal aspect of the nail and at the distal edge of the nail bed is the hyponychium ( Fig. 6.1C ), which forms from a thickening of stratum intermedium known in the embryo as the distal ridge.
 The nail, the sterile and germinal matrices, and the surrounding tissue marked in blue compose the perionychium. (B) A lateral view of the nail bed showing the ventral floor (germinal matrix), the nail bed (sterile matrix), and the dorsal roof of the nail fold. (C) Histologic section of the keratinous plug at the hyponychium.")
The nail bed consists of the germinal and sterile matrices. The germinal matrix makes up the ventral floor of the proximal nail fold. The sterile matrix consists of the soft tissue immediately beneath the nail distal to the germinal matrix.
The nail unit is supplied by branches of the common volar digital arteries. As described by Flint, the digital arteries form three arterial anastomoses over the dorsal surface of the distal phalanx. A superficial arcade supplies the nail fold, and proximal and distal arcades wrap around the waist of the distal phalanx to supply the sterile matrix and the pulp space. On dissection of 10 amputated digits, Zook et al . found two consistent dorsal arterial branches of the digital arteries. The first branch was seen at the base of the nail fold and the second branch at the level of the lunula. Venous drainage of the perionychium coalesces laterally and dorsally, proximal to the nail fold, drains in a random fashion over the dorsum of the digit, and becomes large enough for vessel anastomosis at the level of the distal interphalangeal joint.
Lymphatics roughly parallel the veins and are most numerous at the free edge of the nail (hyponychium). The density of hyponychial lymphatics is greater than in any other dermal area of the body. This explains the low subungual infection rate, considering the heavy exposure of the hyponychial region to pathogenic organisms with use of the nails and fingertips to scratch frequently contaminated areas ( Fig. 6.2 ).
 A swollen, inflamed paronychium known as a paronychia. (B) The side of the nail, which is undermined by the infection, is separated from the nail bed and the lateral aspect of the dorsal roof of the nail fold. (C) This fragment of nail is removed, giving adequate drainage to the infection. (D) A piece of water-soluble gauze is placed as a drain.")
Knowledge of the anatomic arterial branching patterns allows creation of fingertip flaps to preserve length after distal fingertip amputation injuries. These local flaps will be discussed in detail later in the chapter.
The common volar digital nerves branch dorsally, just distal to the distal interphalangeal joint, to supply the perionychium. Zook et al . reported the most common distribution of branching (70%) to be a proximal fascicle into the deep nail bed at the level of the lunula and a distal branch to the hyponychial area. Wilgis and Maxwell reported innervation by three nerve branches, including two dorsal branches as well as a branch to the pulp.
The hard and elastic structure of the nail plate is produced continuously by the nail matrix. The nail is transparent, however it appears pink due to the presence of vessels of the underlying nail bed. Keratinization of nail matrix cells occurs along an oblique axis. As a result, the proximal part of the nail matrix produces the dorsal portion of the nail plate and, when damaged, gives rise to the development of nail plate surface abnormalities, whereas the distal part of nail matrix produces the ventral portion of the nail plate. The nail plate is firmly attached to the nail bed and it detaches at the hyponychium, where its color becomes white due to the presence of air underneath.
Nail growth continues throughout life. The speed of growth increases with age until 10–14 years, at which point it becomes similar to adults, which averages about 0.1 mm a day, which is a rate 4 times faster than toenails. The rate of growth changes by season, with growth increased during summer months and by age. Nail growth is twice as rapid before the age of 30 years than after 80 years. Nail growth is also affected by comorbid conditions of the individual, including endocrine, vascular, infectious, and nutritional disorders. The rate of complete nail progression from the nail fold to the free margin has been reported to be between 70 and 140 days. Baden described a 21-day delay in growth after injury, during which time the nail thickens proximally but does not grow distally. Distal growth of a thicker than normal nail proceeds for the next 50 days, followed by growth of a thinner than normal nail for 30 days. Therefore, it is normal for an injury-induced lump to be present on the growing nail. Nail growth is not normal for approximately 100 days after injury. The nail is fixed to underlying tissues by virtue of being a continuous chain of cells from the germinal layer into the nail, each cell attached to the one in front, behind, and beside it.
The nail is produced by cells from three areas of the perionychium: the germinal matrix, the sterile matrix, and the dorsal roof of the nail fold ( Fig. 6.3  ). The germinal matrix produces the majority of the nail volume (90%) by gradient parakeratosis. The sterile matrix and the dorsal roof of the proximal nail fold produce the remaining nail cells. The sterile matrix adds cells to the volar surface of the nail, accounting for the attachment of the nail to the matrix. The addition of ventral nail during distal growth usually results in a thicker nail distally and compensates for the dorsal wear. There are longitudinal ridges in the sterile matrix increasing the surface for attachment and accompany the rich, longitudinally oriented vascularized capillary network. The dorsal roof of the nail fold adds flattened cells to the dorsal surface of the nail, producing the shine of the nail. Loss of the dorsal roof causes a dull-appearing nail. Proximally and laterally, the nail plate is surrounded by the nail folds that are responsible for the protection of the nail matrix. An injured germinal matrix leads to absence of the nail, while an injured sterile matrix leads to nail deformity. The growth of a cosmetically normal nail requires a flat and smooth surface, and the nail bed’s unique structures can make reconstruction challenging.
). The germinal matrix produces the majority of the nail volume (90%) by gradient parakeratosis. The sterile matrix and the dorsal roof of the proximal nail fold produce the remaining nail cells. The sterile matrix adds cells to the volar surface of the nail, accounting for the attachment of the nail to the matrix. The addition of ventral nail during distal growth usually results in a thicker nail distally and compensates for the dorsal wear. There are longitudinal ridges in the sterile matrix increasing the surface for attachment and accompany the rich, longitudinally oriented vascularized capillary network. The dorsal roof of the nail fold adds flattened cells to the dorsal surface of the nail, producing the shine of the nail. Loss of the dorsal roof causes a dull-appearing nail. Proximally and laterally, the nail plate is surrounded by the nail folds that are responsible for the protection of the nail matrix. An injured germinal matrix leads to absence of the nail, while an injured sterile matrix leads to nail deformity. The growth of a cosmetically normal nail requires a flat and smooth surface, and the nail bed’s unique structures can make reconstruction challenging.

The function of nails was described in 1724 as “weapons to defend us from trouble … from small creatures, that often make their habitation upon our bodies and to allay the uneasy titillation by scratching.” Accordingly, fingernails are used for scratching and in defense. The nail protects the fingertip and contributes to tactile sensation. Counterforce between the nail and the volar skin and pulp aids in delicate and precise touch. Picking up small objects is difficult if the nail is absent. Two-point discrimination will frequently double when the nail is lost. However, incompletely attached, or split nails are often painful, especially in individuals who work with their hands, and may be worthy of removal in select situations.
Injury to the fingertip and nail bed is the most common injury of the hand because of its prominent position. The long finger is most commonly injured, followed by the ring, index, small finger and the thumb, with equal frequency bilaterally. The majority of injuries occur between the ages of 4 and 30 years, with 75% occurring in males. Fractures of the distal phalanx are present in 50% of nail bed injuries, and most injuries occur to the middle or distal third of the nail bed.
The mechanism of injury generally constitutes a deforming force, which compresses the nail bed between the nail and the distal phalanx. A subungual hematoma results from injury to the nail bed, causing bleeding beneath the nail ( Algorithm 6.1 ). Most commonly, injury to the nail bed is a simple laceration ( Fig. 6.4A  ), especially when the object causing the injury is small or sharp. A stellate laceration ( Fig. 6.4B ) occurs after compression with larger objects causing a bursting injury. Severe crush of the nail bed ( Fig. 6.4C ) is commonly caused by a wider, greater force of compression. Avulsion injuries ( Fig. 6.4D ) are the least common.
), especially when the object causing the injury is small or sharp. A stellate laceration ( Fig. 6.4B ) occurs after compression with larger objects causing a bursting injury. Severe crush of the nail bed ( Fig. 6.4C ) is commonly caused by a wider, greater force of compression. Avulsion injuries ( Fig. 6.4D ) are the least common.
 36% are classified as simple lacerations; (B) 27% as stellate lacerations; (C) 22% as crushing injuries of the nail bed; (D) 15% as avulsions of the germinal or sterile matrix.")
Fingertip avulsions are most commonly result from being crushed in a house door. Most avulsions are partial avulsions of the fingertip; however, complete amputations are not unusual. Complete or partial avulsions heal exceptionally well in children, especially before adolescence, in comparison to adults. In fact, the literature suggests that children younger than 2 years are likely to show full distal tip recovery following amputation when managed without repair.
Subungual hematoma formation causes separation of the nail from the nail bed. The pressure of bleeding in this closed space frequently results in throbbing pain as pressure to the nail bed rises. Hematoma drainage is thus indicated for pain relief.
The current recommended method for drainage of an acute (less than 48 hours) subungual hematoma is trephination. Drainage is performed with a heated (red-hot), sterile paper clip, battery-operated cautery, 18-gauge needle, or 2-mm punch biopsy, or in children, an insulin-syringe needle may be used. The heated object burns a hole through the nail and is cooled by the underlying hematoma. The hole is made large enough to ensure prolonged drainage of the hematoma. A small hematoma will be incorporated into the nail and travel distally with nail growth. The decision to perform trephination is made by the size of hematoma and symptoms; not all hematomas require drainage.
The extent of underlying nail bed injury is difficult to assess with a subungual hematoma. Some advocate the use of ultrasound to detect nail bed injuries. If there is minimal disruption of the nail bed, normal nail growth is expected. However, if a significant disruption of the nail bed is present, there is higher risk of nail deformity if the nail bed is not repaired.
Therefore, whether a subungual hematoma should be drained with the nail left intact or the nail removed, and the nail bed repaired is debatable. In the past, removal of the nail for inspection of the nail bed with repair, as needed, was advocated for hematomas undermining more than 25% of the nail. Simon and Wolgin examined the nail beds of 47 patients presenting to the emergency department with a subungual hematoma and found that a hematoma >50% had a 60% incidence of laceration requiring repair. Repair of the nail bed was advocated with a hematoma >50% or an associated distal phalanx fracture.
Many studies have shown that trephination has an equivalent cosmetic outcome and comparable rate of complications in the vast majority of cases. At the University of Pittsburgh, a 2-year prospective, observational study was designed to examine the outcome of 48 patients with subungual hematomas treated with drainage alone. No complications of nail deformity were found with this treatment, regardless of the size of hematoma or presence of fracture. Roser and Gellman compared three treatment groups in a prospective study of 52 children with subungual hematomas. A total of 26 fingers were treated with nail removal and repair of the nail bed. Drainage only was performed in 11 fingers, and 16 of 27 fingers were observed. No notable difference in outcome was found between the groups, regardless of hematoma size. It was concluded that nail removal and nail bed exploration are not justified in children with subungual hematoma with an intact nail and nail margin. A systematic review in 2012 evaluated four articles comparing nail bed repair with simple decompression and concluded the outcome of nail cosmesis did not differ by the mode of treatment. Leaving the nail in place is recommended for most subungual hematomas with an intact nail. Exceptions may include children or patients with concern for an optimally aesthetic nail. If the nail is broken or the edge disrupted, removal of the nail and exploration of the nail bed are advised ( Fig. 6.5 ). The acutely painful subungual hematoma should be decompressed, whether done by trephination or nail removal.
 an avulsion injury of the nail plate with a stellate laceration of the nail bed in the sterile matrix with an intact germinal matrix. (B) The nail was taken off with a Freer elevator, the nail bed and hyponychium were repaired, and the nail plate replaced. (C) 4 months after injury and repair (left index finger) compared to the uninjured right index fingernail.")
Avulsion of the nail, or nonadherence of the nail to the nail bed, is an indication for nail removal. Any loose nail should be trimmed and only enough of the nail that allows adequate exposure and repair of the nail bed laceration should be removed. Complete removal of the nail is not always necessary. With middle to distal nail bed injuries, it may be possible to leave the proximal nail undisturbed within the nail fold.
Exploration of the nail bed is performed with digital block, anesthesia, and tourniquet (e.g., a half-inch Penrose drain or cut-out from a sterile glove). The nail plate is gently removed from the nail bed with a small periosteal elevator or iris scissors. Careful removal of the nail is important to avoid further injury to the nail bed. Once removed, the nail is scraped to remove residual soft tissue, then soaked in povidone-iodine (Betadine) solution. The nail bed is examined with loupe magnification. It is better to leave ragged edges and allow the replaced nail to mold the edges than to debride and cause tension on closure. Careful undermining of the edges may assist in reducing tension on closure. A double-armed 7-0 chromic suture on an ophthalmic needle is recommended. The suture is cut in half to provide a second stitch because the small needle is commonly bent during the repair.
Reapproximation of the more complex stellate laceration and crush injury is more difficult. In these types of injuries, it may appear to be missing fragments. However, they are often present, attached to the undersurface of the nail. Small fragments should be gently removed with a periosteal elevator and used as a nail bed graft. A split- or full-thickness nail bed graft up to 1 cm in diameter will usually survive, even when it is placed directly on the distal phalanx cortex. Blood supply to the graft is established by inosculation and vascular ingrowth from the periphery.
The scenario with nail bed fragments attached to the nail commonly occurs in avulsion type of injuries. To avoid further insult to the nail bed, leaving the large nail bed fragment on the nail is recommended. The edges of the nail are trimmed a few millimeters to expose the nail bed for suturing into the defect.
Avulsion of the bed often occurs at the level of the germinal matrix and proximal nail fold, leaving a distally based nail bed flap of germinal or sterile matrix ( Fig. 6.6A ). The nail bed remains attached to the nail, avulsing the germinal matrix off the bone and out of the nail fold ( Fig. 6.6B ). The nail and germinal matrix must be separated, and the germinal matrix replaced and sutured back into the nail fold ( Fig. 6.6C ). The nail fold is exposed with unilateral or bilateral incisions perpendicular to the lateral corners of the eponychium. The incisions should be made at a 90° angle to the eponychium to prevent a notch deformity ( Fig. 6.6D ). If the laceration occurs at the junction of the ventral and dorsal roof of the nail fold, suture approximation may not be possible. In this case, a horizontal mattress stitch is placed through the proximal end of the avulsed nail bed and brought out through the nail wall. This will secure the nail bed within the nail fold. The eponychial incisions are then reapproximated with 5–0 or 6–0 nylon after nail bed repair.
 When the proximal nail is flipped out of the nail fold and is lying on top of it, one must remove the nail and explore the nail bed. (B) There is almost always a nail bed laceration with stripping of the germinal matrix up with the nail or a Salter fracture of the distal phalanx. (C) The laceration must be replaced and repaired. (D) Radial incisions are made in the eponychium to access the nail fold. It is almost impossible to replace the nail in the nail fold without its total removal and then sliding it back.")
Loss of small areas of nail bed may be replaced with split-thickness nail bed grafts from adjacent uninjured nail bed, harvested carefully with a No. 15 scalpel blade ( Fig. 6.7A,B ). A split-thickness nail bed graft may be harvested from an adjacent noninjured finger (risky) or an amputated finger. A split toenail bed graft may also be used acutely and avoids the possible deformity of an adjacent nail ( Fig. 6.7C–H ). With exception of the great toe, the nail bed from the other toes is not large enough to supply enough graft for an entire finger nail bed.
 A crushing injury to the tip of the finger with laceration of the surrounding skin. (B) After the skin is sutured, an area of cortex is seen. (C) A split-thickness sterile matrix graft is removed from an adjoining area on the finger or toe. Back-and-forth sawing with a scalpel blade will remove a small fragment of nail bed, which is slightly curved after the nail has been removed. The white line of the sharp edge of the blade should always be able to be seen so that the graft is not taken too thick with a resultant deformity. (D) The fragment of nail bed taken . (E) If a larger piece of nail bed graft is needed, it may be taken from proximal to distal; the tip of the knife blade is used to dissect up the split-thickness layer of nail bed. (F) The large toe after removal of the split-thickness nail bed graft. (G) A split-thickness nail bed graft is sutured into place over the periosteum without any manipulation of the cortex. (H) One year later, good regrowth of the nail and adherence are shown.")
On completion of the nail bed repair, the nail is removed from the povidone-iodine solution and a hole made in the nail away from the site of injury. The hole allows drainage of the subungual space after reinsertion of the nail into the nail fold. The nail is placed within the nail fold to mold the edges of the repair, to act as a splint for tuft or phalangeal fractures, to prevent formation of synechiae between the nail fold and the injured nail bed, and to protect the tender fingertip. The nail is held in place with a 5-0 nylon suture placed distally through the nail and hyponychial region. On rare occasions with severe injury to the fingertip, a mattress suture may be placed proximally through the nail fold. If the nail is not available or is in small fragments, a piece of silicone sheeting (reinforced 0.020-inch-thickness silastic) may be shaped to fit beneath the nail fold and secured proximally through the nail fold ( Fig. 6.8 ). Unlike the nail, the silastic sheet is soft and easily slips from beneath the nail fold if it is secured only distally. Non-adherent gauze may also be placed within the nail fold if no nail or silicone sheet is available.

The fingertip is dressed in nonadherent gauze, 2-inch roll gauze, and a four-prong splint to protect the repair. At 3–7 days after repair, the holding suture is removed, especially if it is in the proximal nail fold position. The authors have observed stitch track formation in the nail fold if the stitch is left in place longer than 7–10 days. If not disturbed, the nail will frequently adhere to the nail bed for 1–3 months as the new nail forms beneath. Fingertip tenderness is usually less with the nail replaced.
Distal phalanx fractures are found in approximately 50% of nail bed injuries and result in a higher incidence of secondary nail deformities. Therefore, multiple-view radiographs of the distal phalanx are recommended. A Seymour fracture presents in children with the appearance of an elongated nail. The fracture occurs through the physis with interposed soft tissue, usually consisting of nail bed matrix but can include other tissues, like eponychial fold.
Treatment of non-displaced distal fractures consists of nail bed repair and replacement of the nail. The nail acts as an excellent splint for the fracture. Small, displaced tuft fractures and most stable distal fractures can be reduced with reapproximation of the nail bed and replacement of the nail. Larger displaced fractures or unstable fractures require longitudinal or cross K-wire fixation. Care must be taken to put the pin in the medullary cavity of the bone (see Fig. 6.9 ). K-wires traversing the nail bed can cause a painful ridging deformity.

Tuft fractures are the most common fracture seen in a patient with a subungual hematoma and an intact nail fold. Tuft fractures typically require finger splinting for at least 14 days; however, they may not require a splint at all. Zook et al . reported that distal phalanx or tuft fractures were associated with the occurrence of nail surface irregularities. Since then, it has been traditionally believed that bone continuity provides a smooth scaffold for the nail bed, which is considered necessary for natural-appearing nail bed production. Range of motion exercises should begin without delay.
The painful nonadherent, split, or hooked nail, may hinder work productivity in the laborer. For others, nail deformities, such as nail ridges, grooves, or absence of the nail may create self-consciousness or an unsightly appearance. Goals for reconstruction should be based on concerns and wishes of the individual patient. Surgical measures often improve function and appearance but often do not produce a normal nail. The best chance for restoring a normal nail is at time of the initial repair.
Most nail deformities are secondary to scarring of the nail bed with subsequent disruption of nail growth. Like other scars, it is recommended to wait at least 8–12 months after injury before consideration of reconstruction. With scar remodeling, small nail deformities may resolve significantly or completely. Common secondary nail deformities seen after nail bed injury include nail ridging, splitting, nonadherence, absence, cornified nail bed, hook and spikes, or cysts.
Nail ridges are secondary to an irregularly healed distal phalanx fracture or scar within the nail bed. Nail ridges may also occur secondary to a K-wire placed between the sterile matrix and the periosteum on reduction of a phalanx fracture ( Fig. 6.9  ). The longitudinal ridges of the sterile matrix determine the direction of longitudinal growth ; as a result, it is important to match the direction of the defect during harvesting and grafting of a nail bed to avoid the growth of ridged-appearing nails. Longitudinal irregularities result in longitudinal ridges or grooves. Transverse irregularities beneath the nail bed result in corresponding transverse grooves or ridges or distal nonadherence. Correction of this deformity requires excision of the scar or irregular bone edge to form a flat, smooth nail bed surface. A defect that cannot be reapproximated primarily requires use of a nail bed graft.
). The longitudinal ridges of the sterile matrix determine the direction of longitudinal growth ; as a result, it is important to match the direction of the defect during harvesting and grafting of a nail bed to avoid the growth of ridged-appearing nails. Longitudinal irregularities result in longitudinal ridges or grooves. Transverse irregularities beneath the nail bed result in corresponding transverse grooves or ridges or distal nonadherence. Correction of this deformity requires excision of the scar or irregular bone edge to form a flat, smooth nail bed surface. A defect that cannot be reapproximated primarily requires use of a nail bed graft.
Transverse nail ridges may develop secondary to hypoxia from ischemic injury or tourniquet hemostasis. The ridges resolve with correction of the inciting factor and subsequent new nail growth.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here