Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Societal interest in plastic surgery is increasing:
The number of plastic surgery procedures as reported by The Aesthetic Society (American Society for Aesthetic Plastic Surgery [ASAPS]) has increased 82% since 1997
Women between the ages of 35 and 50 consistently comprise the largest group of patients for both surgical and non-surgical procedures.
Understanding the patients' motivations for surgery and their expectations of the outcomes are the keys to achieving satisfied patients postoperatively:
Managing the patients' expectations requires detailed information and full patient education
Second consultations are almost always necessary preoperatively
Be sure to discuss your policy for revisional surgery during the preoperative period.
Postoperative follow-up should include detailed written instructions for appropriate activity level and wound care as well as the surgeon's contact details:
Regular follow-up visits are needed during the early postoperative period to assist the patient through the recovery
Unhappy patients or those with unsatisfactory outcomes should be seen more often to improve communication.
What is beauty? The concept of attractiveness seems to be innate and is similar across cultures and religions. While it can be influenced somewhat by social trends and advertising, research shows that subjective attractiveness is largely biological, overlaid with only a small amount of personal preference. Studies looking at the consistency of physical attractiveness ratings across cultural groups agree that facial attractiveness is species-specific, not race-specific. Research in the US has shown that the ratings provided by Asians, Hispanics, Caucasians, and African Americans correlate well for facial attractiveness overall, although features such as expression and sexual maturity influenced some cultural groups more than others. Also, Caucasians and African Americans differed on their judgment of bodies. Judgments can potentially be influenced by cultural norms; for example, the classical Roman nose is very different in size and shape to the African-American nose, so what may be considered a deformity in one person may be attractive on another. There is no simple answer to the question of what constitutes beauty, or even an attractive face.
In order to ascertain what makes an attractive face, some researchers have assessed facial features by judging individual faces, then comparing the results with computer-generated composite faces, averaging the individuals. This research showed there was a trend toward the composite face being more attractive than the faces individually, producing a claim that “attractive faces are only average”. Others have disputed this claim, saying that a mathematically averaged face is not the same as an average face. Interestingly, functional magnetic resonance imaging scanning of subjects during judgment on the facial attractiveness of strangers has shown that perceived facial attractiveness increases with eye contact rather than with increased physical attractiveness per se . These studies have also shown that facial attractiveness is a fundamental condition that a stranger can read rapidly. In fact, it takes only 150 milliseconds and no eye movement to judge a stranger's attractiveness.
Over 2000 articles on the study of facial attractiveness have been published in the past 30 years. Social and psychological literature from the 1970s and 1980s extensively studied the response to physical attractiveness and showed that physical attractiveness has a statistically significant effect on the person's self-esteem and well-being. This implies that beauty has influence which is more than “just skin deep”. Pediatric studies have revealed that parents provide better parenting to attractive children and respond more positively to cuter infants. Studies have also shown that attractive women receive more dates and are perceived to have more positive social attributes. Housman suggested that physically attractive people are offered greater opportunities for success and happiness throughout their life. Attractive individuals are more likely to be hired, promoted, and earn higher salaries than their less-attractive counterparts. As the potential benefits go far beyond improved self-esteem, it is perhaps not surprising that individuals are attending their plastic surgeons with requests for surgical and non-surgical options in an attempt to increase their perceived attractiveness or correct a deformity.
The specialty of plastic surgery is rooted in reconstructive surgery for congenital abnormalities and acquired injuries. Surgery for purely aesthetic reasons was incorporated into the field somewhat later. Research from across the US has shown that societal acceptance of plastic surgery is increasing. The 2010 American Society for Aesthetic Plastic Surgery (ASAPS) Quick Facts consumer attitudes survey found that 53% of women and 49% of men approved of cosmetic surgery, while 27% of married Americans and 33% of unmarried Americans would consider cosmetic surgery for themselves in the future. If you compared those attitudes with previous results, 20% of Americans were more favorably disposed toward cosmetic surgery than 5 years earlier. More recently, a consumer attitudes survey was commissioned by RealSelf.com (an online social media-style community for learning and sharing information about cosmetic surgery procedures) and conducted by Zeitgeist Research in December 2014. They found that more than 30% of the women surveyed would be prepared to undergo plastic surgery to change the appearance of a body part while 7% had in fact already done so.
This increased acceptance may be related to the extensive media coverage in recent years, which essentially normalizes plastic surgery and increases the perceived benefits of cosmetic surgery. This includes celebrities openly discussing their plastic surgical procedures, as well as popular television programs such as the series Nip/Tuck and reality programs Dr 90210 and Extreme Makeover , which have been on our screens since 2002. Even E! Entertainment television's latest show Botched , which focuses on cosmetic surgery gone wrong, is unlikely to negatively influence viewers' attitudes toward cosmetic surgery as plastic surgery is still portrayed as an effective method to transform the unhappy patient's body back to the ideal. The downside of making plastic surgery a form of mainstream entertainment is the misrepresentation of the significance, complexity, downtime, and potential complications of undergoing surgery. These issues increase the chance that the patient will present with unrealistic expectations, which must be clearly addressed by the plastic surgeon at preoperative consultations.
In addition to televised media, the rise in social media sites such as Facebook, Instagram, and TikTok over the past decade has meant that this field has grown rapidly in importance. According to the January 2019 We Are Social report, 3.484 billion people actively use social media – that is 45% of the world’s population. This past decade has seen a massive increase in younger patients taking regular videos or “selfies” and posting these on a social media site, often with the benefit of a built-in filter to enhance their appearance. This is also magnified by the rise of social media influencers, usually celebrities with huge numbers of engaged, enthusiastic followers whose decision making will be influenced by the behavior of the celebrity. This has led to “The Kardashian Effect”, an unofficial term for the rise in the number of young people seeking noninvasive plastic surgery treatments in an attempt to emulate their idols, in this case members of the Kardashian family who flaunt their idealized beautiful bodies and faces on Instagram. Unfortunately, many young people do not understand that the images they see online can be heavily amended by Photoshop or built-in filters. Added to this, it has been suggested that imperfections can appear magnified by the camera lens, prompting the younger generation to turn to cosmetic surgery to correct or enhance their appearance due to the perceived discrepancy between what they see in their camera lens and how they believe others look.
In addition to social media, there has been a huge increase in the use of video conferencing software such as FaceTime (Apple, Inc., Cupertino, CA) and Zoom (Zoom Video Communications, Inc., San Jose, CA). Zoom generated $2.6 billion revenue in 2020, a 317% increase year-on-year, driven in large part by coronavirus 2019 (COVID-19) disease restrictions on personal interactions. Anecdotally, some plastic surgeons have reported a “Zoom Boom” – an increase in facial cosmetic procedures fueled by patients’ dislike of their features and now seeing themselves for hours at a time on video conferencing calls. A survey analyzing respondents’ feelings about their facial appearance during video conferencing found that the majority of subjects reported a concerning facial area, with the nose being most common. Despite many respondents not having any prior facial cosmetic treatments, 40.6% of respondents planned to pursue treatments based on concerns from their video conference appearance alone, with neurotoxin and filler injections being the most common. One survey of patients who underwent facial plastic surgery procedures in Canada in 2020 concluded that patients were more aware of their nose than any other facial feature due to video conferencing during COVID-19-related lockdowns compared with before the pandemic. This was reflected in the respondents most common procedure being rhinoplasty. Those who had surgery during the 2020 pandemic noted the advantages of this, including having ample privacy from family, friends, and co-workers (77%) and not requiring extended leave of absence from work (69%) during the postoperative recovery period. This trend was echoed around the globe, with research from The Clinic in London finding an 80% increase in facial plastic surgery procedures after the lifting of nationwide lockdown measures mid-2020 compared with the same timeframe pre-pandemic in 2019. The authors agreed that both privacy at home and time to recover were contributary. They also postulated that household expenditure of holidays and outings decreased during lockdown; thus, extra disposable income may have also played a part in the rise in cosmetic procedures.
While the 2020 statistical data from The Aesthetic Society is currently available, as mentioned above it is likely to be skewed significantly by the global COVID-19 pandemic and it may not be appropriate to compare it with previous years. Therefore we have chosen to focus on the 2019 data as the most recent non-pandemic year at time of printing. Statistics for surgical procedures performed in 2019 show that the most commonly performed plastic surgery operations are breast augmentation (280,692 procedures) and liposuction (270,670 procedures) ( Fig. 1.1 ). Compared with the surgical statistics from 1997, there has been a significant increase in these procedures ( Fig. 1.2 ). This is in line with the overall almost 100% increase in plastic surgical operations performed over this period. Over this same time period there has also been a significant rise in non-surgical cosmetic procedures, such as injectables (botulinum toxin, hyaluronic acid, and so forth), laser hair removal, and skin-resurfacing techniques, which have outpaced the growth in surgical procedures. This trend also highlights the public's acceptance of cosmetic procedures overall, and the popularity of non-surgical procedures may indicate a pool of potential patients who will consider operative procedures in the future.


For many years now, the largest age group of patients undergoing surgical and non-surgical procedures is between 35 and 50 years of age, with 40% of procedures being performed in this age group in 2019 ( Table 1.1 ). The Aesthetic Society statistics show that patients in the age group younger than this (19–34 years) are undergoing surgical procedures less commonly than those in the older age bracket (51–64 years) (20.2% and 28.7%, respectively), which is a change from 2016 when these numbers were essentially equivalent in each group. Prior to its closure, a reader survey by More! magazine in the UK revealed that 72% of women in their twenties would like to have plastic surgery. However, perhaps this interest is not translating to operative procedures at present.
| 17 years and under | 19–34 years | 35–50 years | 51–64 years | 65+ years | |
|---|---|---|---|---|---|
| Surgical procedures | 0.90% | 20.20% | 40.00% | 28.70% | 10.20% |
| Non-surgical procedures | 0.70% | 15.10% | 37.10% | 32.80% | 14.30% |
Not surprisingly, the majority of surgical and non-surgical patients are female (93.0% and 90.3%, respectively) ( Table 1.2 ).
| Female | Male | |||
|---|---|---|---|---|
| Number | Percentage | Number | Percentage | |
| Surgical procedures | 1,366,914 | 93.00% | 102,838 | 7.00% |
| Non-surgical procedures | 2,818,219 | 90.30% | 303,221 | 9.70% |
| Overall | 4,185,133 | 406,059 | ||
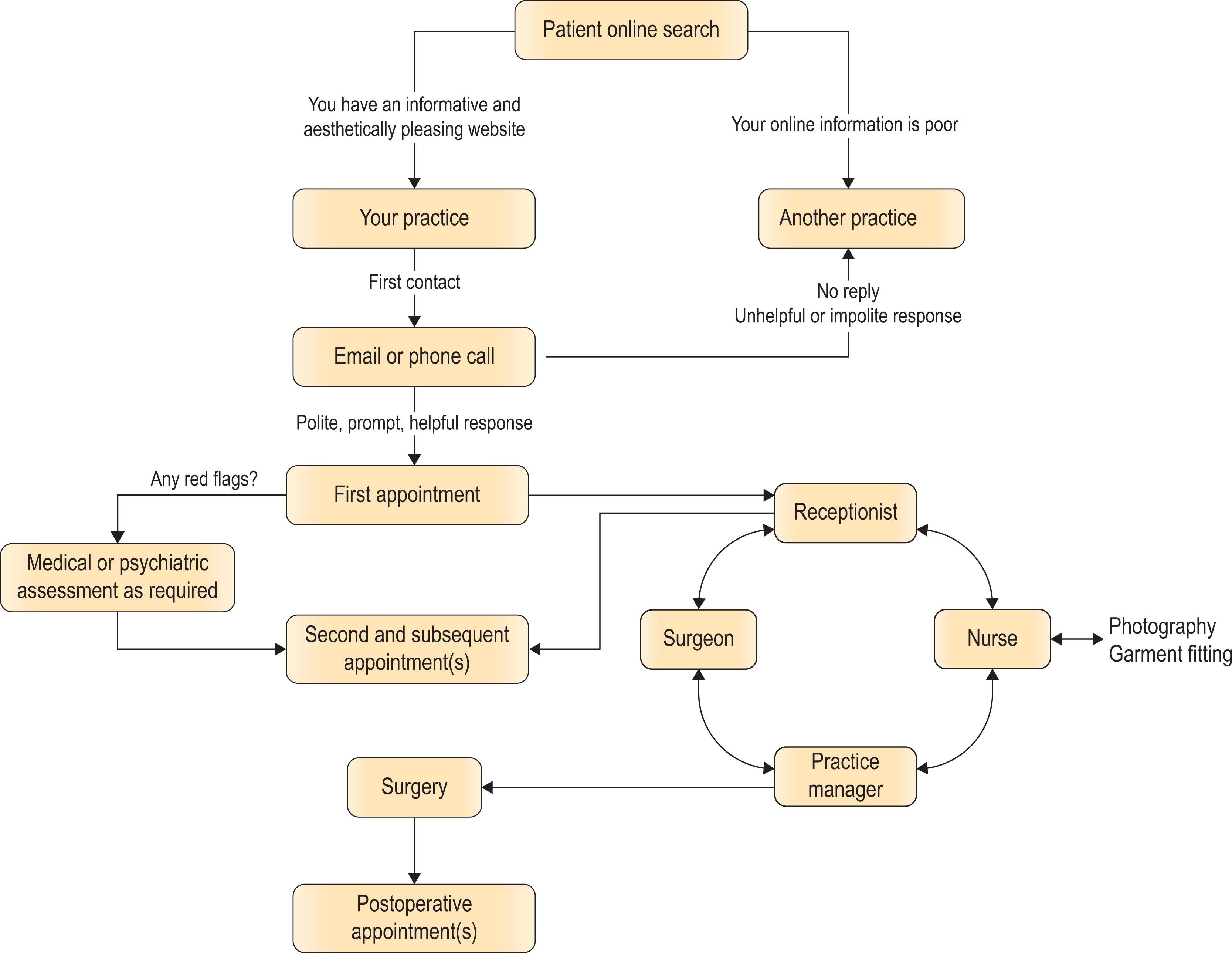
When aesthetic plastic surgery first developed, advertising the surgeon's services was considered distasteful and was frowned upon by most practitioners. However, as times have changed, advertising of services has become commonplace. In these authors' opinion, advertising should be discreet, professional, and truthful. A professional, thorough website, which can be accessed by public search engines and via links from the websites of professional bodies with whom the surgeon is affiliated, is essentially a common form of advertising. Having an informative and aesthetically pleasing website is the first step to patient engagement with your practice ( Algorithm 1.1 ).
Many patients say they wish to see “before and after” photos if possible. Some registration agencies such as the Medical Council of New Zealand (MCNZ) have specific guidelines on adverting and the use of “before and after” photographs. These Standards acknowledge that photographs have a significant potential to mislead or to convey inappropriately high expectations of a successful outcome. The MCNZ specifically states that any practitioner displaying before and after photos must ensure any photos:
Are there solely for the purpose of providing accurate and useful information to patients.
Show a realistic portrayal of the outcome that can reasonably and typically be expected.
Only depict patients who have undergone the advertised procedure while under your (or your services’) care.
Have not been altered in any way.
Use the same lighting, contrast, background, framing, camera angle, exposure, and other photographic techniques in both the “before” and “after” images.
These are well-stated standards by which all reputable surgeons should adhere. Of course, maintaining patient privacy and ensuring appropriate consent has been obtained for the use of any patient photograph in such a fashion is essential.
As a minimum, the website should cover the surgeon's personal philosophy and procedures offered, and provide contact details and a location map. Additionally, advertising in local magazines or newspapers may be appropriate. However, it is important that plastic surgery is not seen to be trying to sell a service to the patient, but instead is advertised as available and able to meet the patient's needs and requirements with competence and care. The American Board of Plastic Surgery, the American Society of Plastic Surgeons (ASPS), and ASAPS all have ethical codes and guidelines governing advertising to which diplomats and members must adhere. These specifically prohibit misrepresentation of the surgeons' qualifications or expected results.
As Greer stated in 1984, “Understanding the motives, expectations, and desires of a patient seeking cosmetic surgery is at least as important as manual dexterity for achieving consistently satisfactory results.” The patient may seek cosmetic surgery for any number of reasons. Elucidating the patient's motivation is a goal of your first patient encounter. The best reason for wanting plastic surgery is for self-improvement. However, there are many other potential reasons. Patients may feel that surgery will alter their life in some way, perhaps make them more outgoing, help them secure a partner, or save their marriage. The surgeon must be wary of patients with hidden agendas, as an excellent surgical outcome may still not result in a happy patient postoperatively.
During the initial consultation, the surgeon must attempt to ascertain what the patient actually wants. This may be different from what the spouse or partner or parents want. If the patient is not initiating the surgery, then beware operating on the patient. If the patient has attended the first appointment with his or her partner and the surgeon feels the partner is the driving force behind the consultation, a second appointment should be scheduled with the patient alone. It is important to ensure that it is the patient who wants the surgery and that s/he fully understands the ramifications of surgery before going ahead with any procedures.
Another potential warning sign regarding patient motivation is “doctor shopping”. While we encourage any patient to seek a second, or even third, opinion if they wish, if the surgeon is aware that the patient has seen several doctors already, this should strike a warning bell. The surgeon should inquire as to the reason for this. Perhaps the patient's request for surgery has been declined by other surgeons with good reason. The patient's expectations may be excessively high and unrealistic. The patient may simply be indecisive. The surgeon should be cautious about offering surgery to these patients unless there is a thorough understanding about the reasons for that patient shopping around.
The ideal patient for cosmetic plastic surgery is one with whom the surgeon can develop rapport and understanding. Patients should be pleasant to the surgeon and the office staff, have effective communication skills, and be intelligent, well educated, and well informed regarding their potential treatment. They must have an identifiable deformity for correction, with realistic expectations of the outcome and a full understanding of potential complications. They should be sensible and compliant with pre- and postoperative instructions. Unfortunately, not all of our patients fit this profile!
In the past two decades, the number of cosmetic procedures performed on men has increased more than 250%. Currently, male patients account for 7.0% of all cosmetic surgery in the US, and men underwent over 100,000 cosmetic surgery operations in 2019. The most common operations include liposuction, male breast reduction (for gynaecomastia) and eyelid surgery (blepharoplasty), with tummy tuck (abdominoplasty) and nose surgery (rhinoplasty) rounding out the top five surgical procedures for men ( Fig. 1.3 ). However, overall men represented a significant proportion of patients undergoing facial aesthetic surgery, making up 34.8% of ear surgeries performed, as well as 16.6% of all eyelid surgeries, 14.0% of the chin augmentations performed and 16.4% of all necklift procedures in 2019.

Importantly, men are often overrepresented in the complication data for their procedures, particularly hematoma rates. This should be thoroughly discussed with patients before surgery. The reported incidence of hematoma following male rhytidectomy ranges from 8% to 13% in most series, twice as high as for females. This may be related to the greater vascularity of the male facial skin, with a higher number of microvessels to supply the hair follicles. The senior author believes that strict perioperative blood pressure control may be the most important aspect of care to reduce this rate. To this end, we routinely give all male patients clonidine 0.1 mg postoperatively unless contraindicated. Clonidine is a centrally acting, alpha-2 adrenergic receptor agonist, which is long-acting, with a half-life of about 12 hours. We believe this medication helps stabilize the patient’s blood pressure to reduce the risk of postoperative bleeding.
How young is too young for aesthetic surgery? This is not a straightforward question, and the answer usually depends on the reason for the surgery and the degree of patient deformity and concern. The number of teenage patients is small – only 0.9% of all patients undergoing plastic surgical procedures in 2019, down from 1.6% in 2016. Data from the last 20 years of reporting from both the ASAPS and the ASPS show similar rates every year over the time period, ranging between 1% and 3%. In 2019, liposuction was the most common surgery for teenagers overall, with 3571 procedures performed on patients 17 and under. While these data show that only 1.2% of all breast augmentations were performed on women 17 years of age and under, this was the second most common type of operation performed in this age group, with 3329 performed in 2019. This is despite the fact that the US Food and Drug Administration (FDA) only approves saline-filled breast implants for cosmetic augmentation in women aged 18 years and over and silicone-filled implants for women 22 years and older. The FDA states that this restriction is placed because “breasts continue to develop through late teens and early 20 s and because there is a concern that a young woman may not be mature enough to make an informed decision about the potential risks”. Ear set-back surgery (otoplasty) was the third most common surgery for teenagers, with breast reduction and nose surgery (rhinoplasty) completing the top five most common procedures ( Fig. 1.4 ).

As the FDA implies in their statement on breast augmentation, the greatest concern when operating on a young patient is that the teen will have unrealistic expectations from the surgery. Clearly, plastic surgeons need to assess the emotional maturity as well as the physical maturity of younger patients before undertaking any surgical procedures. The young patient must understand that the surgery itself results in a permanent change. In particular, patients must understand that there will be permanent scars and there are potential complications that will be with them for life. A thorough preoperative assessment of why the young patient wishes to have the surgery, and what difference the patient thinks it will make to their life, should be undertaken. Any unrealistic expectations of the changes that the surgery may make should warn the surgeon against operating until the patient is more emotionally mature and may prompt a psychological referral instead.
In almost all of the US, individuals are considered minors and therefore unable to consent to surgery until they reach the age of 18. State legislation requires parental consent for surgery on any patient under 18 years. However, the state recognizes that the legal age of majority is arbitrary and that there are minors who are competent and others, of legal age, who are not. While this can be confusing, the fundamental basis of the legislation is to protect minors from the consequences of poor decisions. A responsible plastic surgeon also has a role to play in protecting young patients from the consequences of unnecessary surgery, even if the patient is over the age of majority. First and foremost, it is the surgeon's job to care about the patient's overall well-being.
Younger patients need support people during and after surgery as much, or even more, than older adults. During the preoperative assessments, make note of who attends with the patient. Is it a parent or caregiver? Or is it a boyfriend or girlfriend? While patients over 18 are not required to inform their parents of their request for surgery, it can show a level of maturity if the patient has discussed the surgery with parents and has family support before going ahead. Contrast this with young patients who do not want to tell anyone they are undergoing surgery. Who will look after them during their postoperative recovery period? Who will bring them to their follow-up visits? Who will support them if there are complications? Also, plastic surgery for aesthetic purposes is not normally covered by insurance, raising the question of how patients will pay for the primary surgery and what arrangements they can make to pay for revisions and complications. Parental and family support assists both emotionally and physically, and the plastic surgeon should be wary of operating on a young patient without an obvious support network.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here