Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Lower extremity trauma is commonly associated with other organ injuries.
A primary survey is essential to quickly recognize life-threatening conditions and perform critical interventions as early as possible.
The initial assessment of extremity trauma involves evaluating vessel, bone, nerve, and soft-tissue injury, and checking for compartment syndrome.
A multidisciplinary approach with an orthoplastic concept is applied from diagnosis to rehabilitation.
The decision for limb amputation is not determined by a scoring system.
The concept of wound healing and a skilled microsurgery technique are required for complex lower extremity reconstruction.
Substantial effort and time should be devoted to successful limb salvage.
 Access video lecture content for this chapter online at Elsevier eBooks+
Access video lecture content for this chapter online at Elsevier eBooks+
Injury is the leading cause of death and disability in all age groups, causing approximately 5 million deaths worldwide annually, accounting for 9% of all deaths. In the United States, unintentional injuries or accidents are the third leading cause of death in all age groups, accounting for 6% of all deaths in 2018. Indeed, unintentional injuries are the leading cause of death in the population aged 1–44 years. The relative burden of mortality from injury is far more significant at younger ages, accounting for 31.8% of all deaths for the 1–9 year age group, 38.3% in the 10–24 year age group, and 34.0% in the 25–44 year age group. In developing countries, injury-related mortality rates are even higher than those in developed countries.
Trauma to the lower extremities is a common injury pattern observed in emergency medical and surgical practice. The management of lower extremity injuries involves a multidisciplinary approach. Initial assessment begins with the primary investigation of life-threatening injuries based on the Advanced Trauma Life Support (ATLS) protocol, which is a standardized acute care system that aims to reduce trauma mortality during the golden hour.
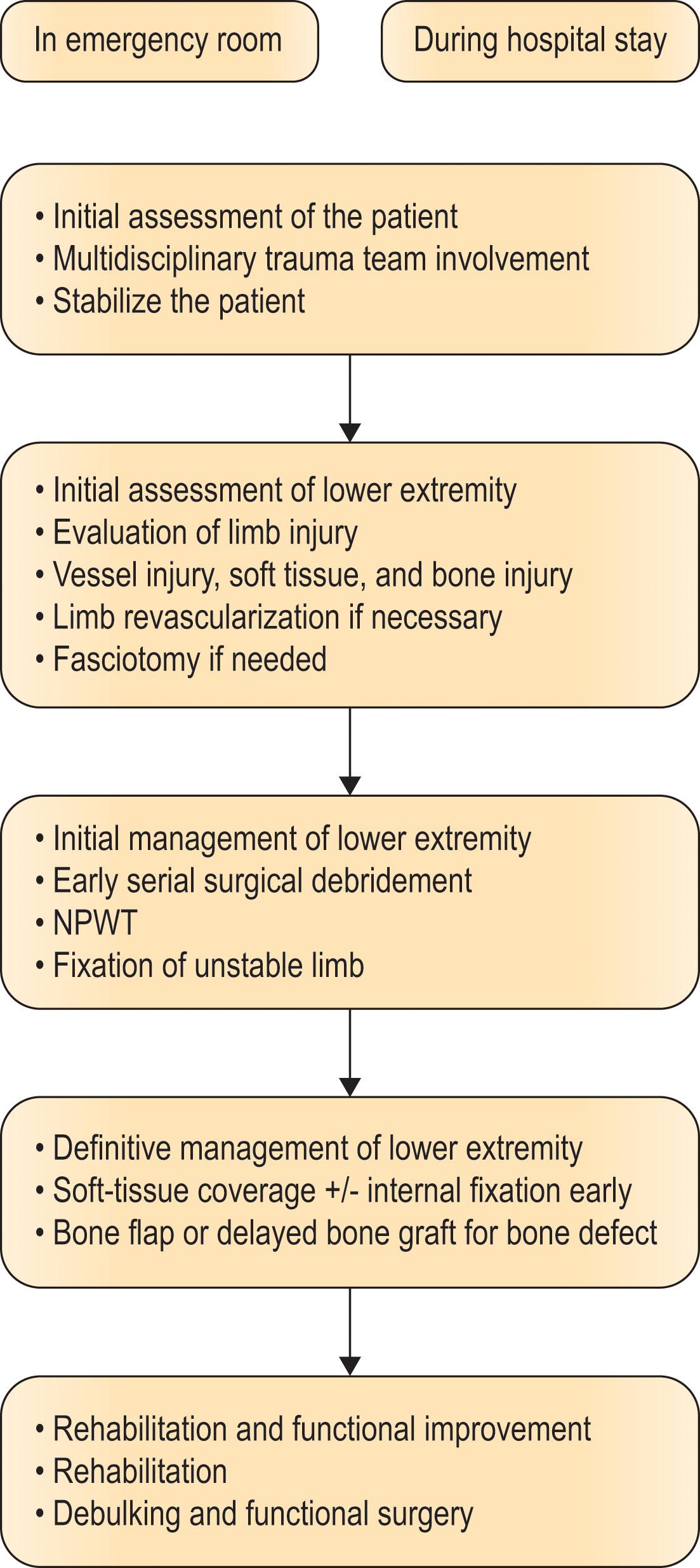
Following the initial evaluation of the medical condition and spinal cord injury, a thorough investigation of the extremity injury is initiated by the trauma team, which includes general surgery, vascular surgery, orthopedic surgery, and plastic surgery specialists. This integrated access to the patients, also known as Levin’s concept of orthopedic approach, should be applied from the emergency room to prevent amputation, restore limb function, and improve the quality of life outcome in patients with lower extremity injury. With a multidisciplinary team approach, surgical debridement of the necrotic tissue and external fixation of the fractured bone is followed by immediate flap coverage or delayed flap surgery after wound care. In cases of bone loss, bone graft or vascularized bone graft can be performed as a delayed procedure or by immediate bone flap coverage simultaneously with soft-tissue coverage ( Algorithm 2.1 ).
Without medical treatment, most patients with major trauma die due to blood loss. This first began to change in the 16th century when the French surgeon Ambroise Paré was the first to ligate arteries during amputation. Treatment improved over the following centuries, especially after the outbreak of World War II. Most patients who would have died in earlier times are now being saved thanks to advances in bleeding control. However, more than 6% of survivors of massive hemorrhage develop septic complications, with 20% of patients developing multi-organ failure (MOF). The activation of the immune system following trauma is vital for the protection and healing of the wound. Following severe trauma, the human body responds similarly to systemic inflammatory response syndrome (SIRS) and sepsis, and bacterial pathogens and injury cause similar immunologic responses at the genomic and transcriptomic levels. This similarity previously led to the assumption that post-traumatic SIRS was a response to bacterial inoculation. However, it is now considered to be a sterile process. This response is a combination of proinflammatory and anti-inflammatory responses, which start within 30 min of a major injury to favor blood loss and tissue damage rather than infection.
SIRS results from the release of damage-associated molecular patterns or alarmins after tissue injury. Recognition of these patterns leads to the activation of immune cells, such as neutrophils and monocytes, and the rapid generation of C3, C5a, and interleukins, which activate the inflammatory process and can cause early MOF ( Fig. 2.1A ). The post-traumatic immune system has a balancing compensatory anti-inflammatory response to dampen the inflammatory reaction, termed compensatory anti-inflammatory response syndrome (CARS), which can be described as postinflammatory immunosuppressive status. This feedback loop is characterized by increased levels of anti-inflammatory cytokines and cytokine antagonists. The anti-inflammatory response limits progressive tissue damage and maintains homeostasis to prevent further organ damage. In the balancing process of proinflammatory and anti-inflammatory reactions, the response can either be stabilized at baseline or progress to persistent inflammation, immunosuppression, and catabolism syndrome (PICS), with an increased risk of MOF and sepsis during the critical care period ( Fig. 2.1B ). Plastic surgeons should evaluate the general condition and immune response of the patient and accordingly decide when to reconstruct the defect of the limb or other parts of the body, not only for successful reconstructive surgery limb salvage but also to save the patient.
 Inflammatory response to injury.")
Lower extremity trauma is often accompanied by poly-trauma, and more than one-third of patients with multiple trauma have a significant lower extremity injury. The initial treatment of patients with multiple trauma should involve rapid assessment and management. For immediate evaluation, emergency trauma care should be well organized according to the concepts of triage, resuscitation, diagnosis, and therapeutic intervention.
The Airway, Breathing, Circulation, Disability, Exposure (ABCDE) approach is used to rapidly recognize life-threatening conditions and perform critical interventions first. This approach can save valuable time in the early stage of treatment in poly-trauma cases immediately upon arrival to the emergency room.
In the initial evaluation of a trauma patient, the airway should be assessed first. If the patient can respond in a normal voice, the airway is patent. Signs of a partially obstructed airway include noisy breathing and increased breathing effort. A reduced level of consciousness is a common sign of airway obstruction. Maxilla and mandible fractures can cause airway obstruction, and untreated airway obstruction rapidly leads to cardiac arrest. A head-tilt and chin-lift maneuver can secure the airway with spinal immobilization. Foreign materials in the airway should be removed, and suction of the airways should be performed frequently to remove blood or vomit. If the patient has reduced consciousness, a cervical spine injury is presumed, and cervical spine protection should be used throughout the evaluation process. A neck collar can be applied to stabilize the cervical spine.
The thorax and neck should be inspected, auscultated, and palpated to determine if the patient is breathing. Additionally, signs of accessory muscle work, chest symmetry, and nasal flaring should be looked for, and the chest should be percussed for dullness and resonance. If there is hypotension, cyanosis, neck vein distension, and tracheal deviation, tension pneumothorax should be suspected, and proper management must be performed promptly.
Capillary refill and pulsation can be assessed in any setting. Electrocardiography monitoring and blood pressure measurements should also be performed. In trauma patients, hemorrhage is the leading cause of preventable death. Cardiac arrest caused by hemorrhagic shock is difficult to reverse. Hemorrhagic shock can also lead to a progressive loss of consciousness in patients with hypotension. External bleeding from the wound can be controlled by direct compression and hemostatic dressing or with a tourniquet for a limited time. Crystalloid is the fluid of choice for initial resuscitation in trauma patients with bleeding.
The level of consciousness, blood glucose level, pupil size, and motor/sensory status should be checked. The Glasgow Coma Scale (GCS) can be used to objectively describe brain injury in trauma patients. If the GCS is ≤8 in trauma cases, severe brain damage can be presumed, and endotracheal intubation is recommended to secure a definite airway. Reduced consciousness induced by hypoglycemia can easily be corrected with oral or intravenous glucose.
The patient must be undressed, and the entire body should be examined for hidden injuries, rashes, bites, or other lesions. After the examination, a warm blanket or warming device should be provided to prevent hypothermia. Extremities should be splinted if fractures are suspected to reduce pain and blood loss.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here