Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

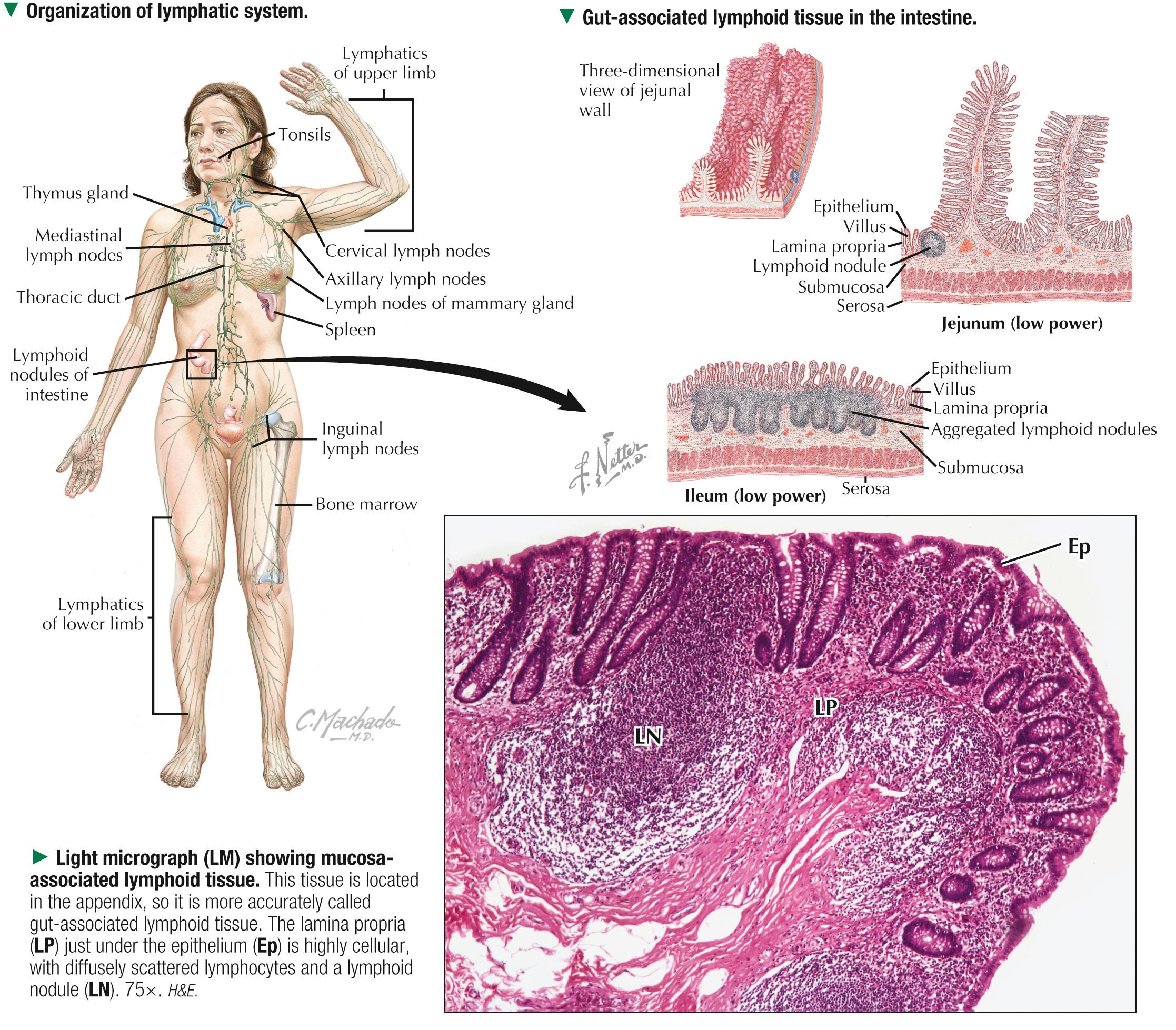
The extensive lymphoid —or immune — system protects the body against potentially harmful effects of pathogens, foreign substances, infectious agents (bacteria and viruses), and abnormal cells. Its major functions are thus to serve as a source of immunocompetent cells that can react with and neutralize antigens and to distinguish self from nonself. The system comprises lymphoid tissues and organs whose main constituents are aggregates of lymphocytes and other cells of the mononuclear phagocyte system. These cells are enmeshed in a supportive framework (stroma) of reticular cells and fibers, so lymphoid tissue is classified as a specialized reticular connective tissue. Lymphatic vessels are also part of the system. Components of the system have different arrangements: diffuse subepithelial lymphocyte aggregates are the most ubiquitous and occur throughout gastrointestinal, respiratory, and genitourinary tracts as mucosa-associated lymphoid tissue (MALT). More densely packed, spherical clusters of lymphocytes called lymphoid nodules (or follicles ) may also be found in these and other sites. The nodules may appear as single collections of lymphocytes or as more permanent, multiple aggregates, such as tonsils and Peyer patches. Discrete lymphoid organs may be encapsulated ( lymph nodes, thymus, and spleen ) or unencapsulated (bone marrow). Lymphoid organs are classified in functional terms as primary or secondary. Primary lymphoid organs —major sites of lymphocyte production and maturation—include bone marrow, where B lymphocytes are produced, and thymus, where T lymphocytes mature. B cells mediate humoral immunity by giving rise to plasma cells, which synthesize antibodies (or immunoglobulins) that inactivate foreign antigens. T cells, in contrast, mediate cellular immunity against microorganisms. Immune responses occur in secondary lymphoid organs, such as lymph nodes and spleen. All lymphoid tissue derives embryonically from mesoderm, except for the thymus, which arises from mesoderm and endoderm.
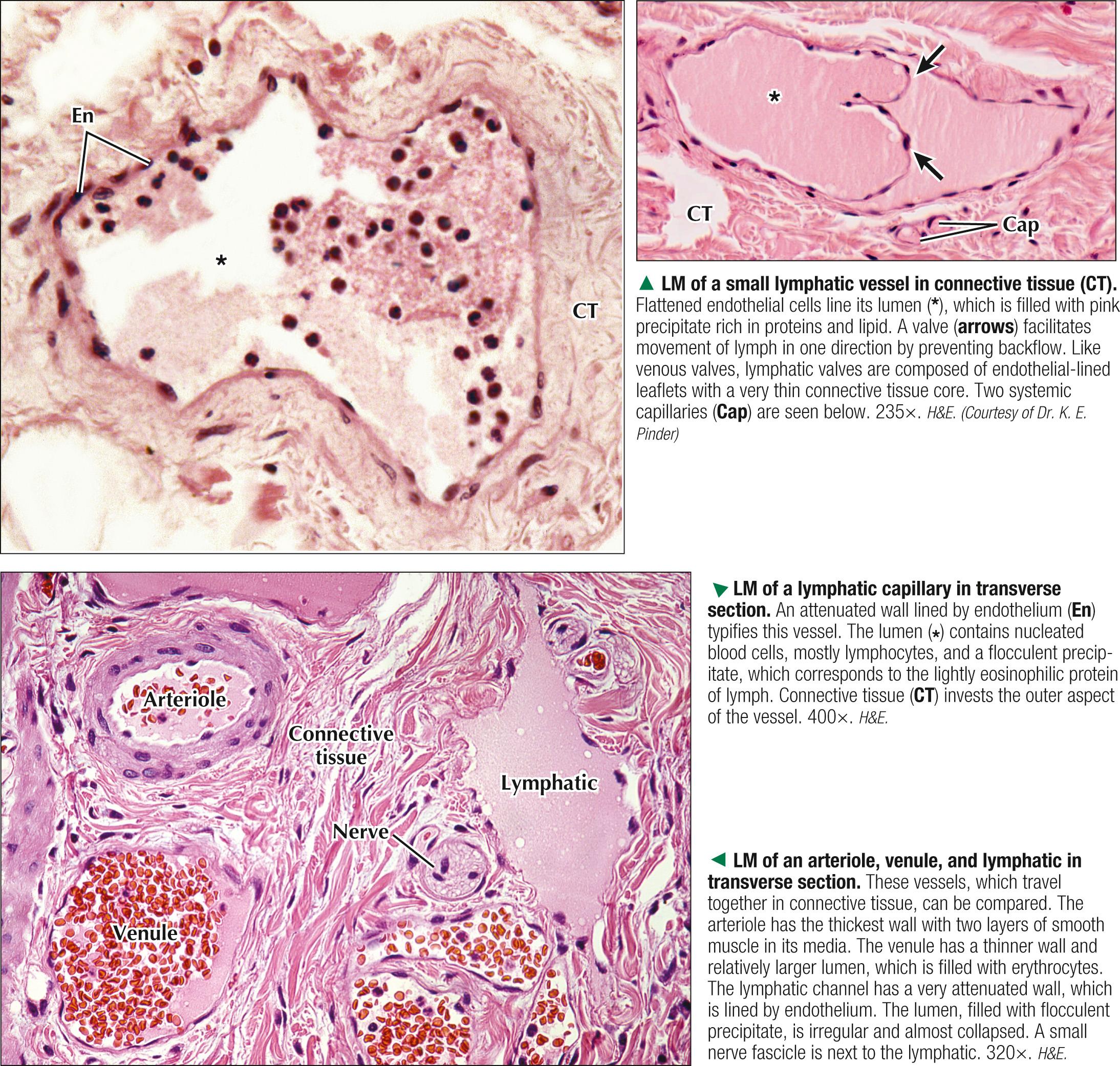
Cells of the lymphoid system are found in connective tissues throughout the body and can travel in the bloodstream or in lymphatic vessels —the lymph—draining part of the circulatory system. Because lymphatic vessels are hard to see in conventional tissue sections, they are probably the least appreciated body structures histologically. By light microscopy, they are similar to capillaries and veins. Lymphatic vessels have wide distribution in many, but not all, body regions. Originating as blind-ended channels in connective tissue spaces, they are then thin-walled lymphatic capillaries (100 µm in diameter) that anastomose and become larger. Lymphatic capillaries look similar to blood capillaries except that they lack a basal lamina. Small anchoring filaments connect endothelial cells to adjacent collagen fibers and help prevent vessel collapse. Lymphatic capillaries are most abundant in connective tissue of the skin (dermis); beneath mucous membranes of the respiratory, gastrointestinal, and genitourinary tracts; and in connective tissue spaces of the liver. These vessels absorb interstitial fluid, which fills the extracellular connective tissue matrix. This fluid and wandering lymphocytes are taken up and added back to the circulation. Like veins, lymphatic vessels have valves and thin walls; contraction of surrounding skeletal muscles causes lymph to move. Lymphatic vessels combine to form the thoracic duct. The large lymphatic ducts drain into the subclavian veins, right at the angle junction where the jugular vein and subclavian vein join together.
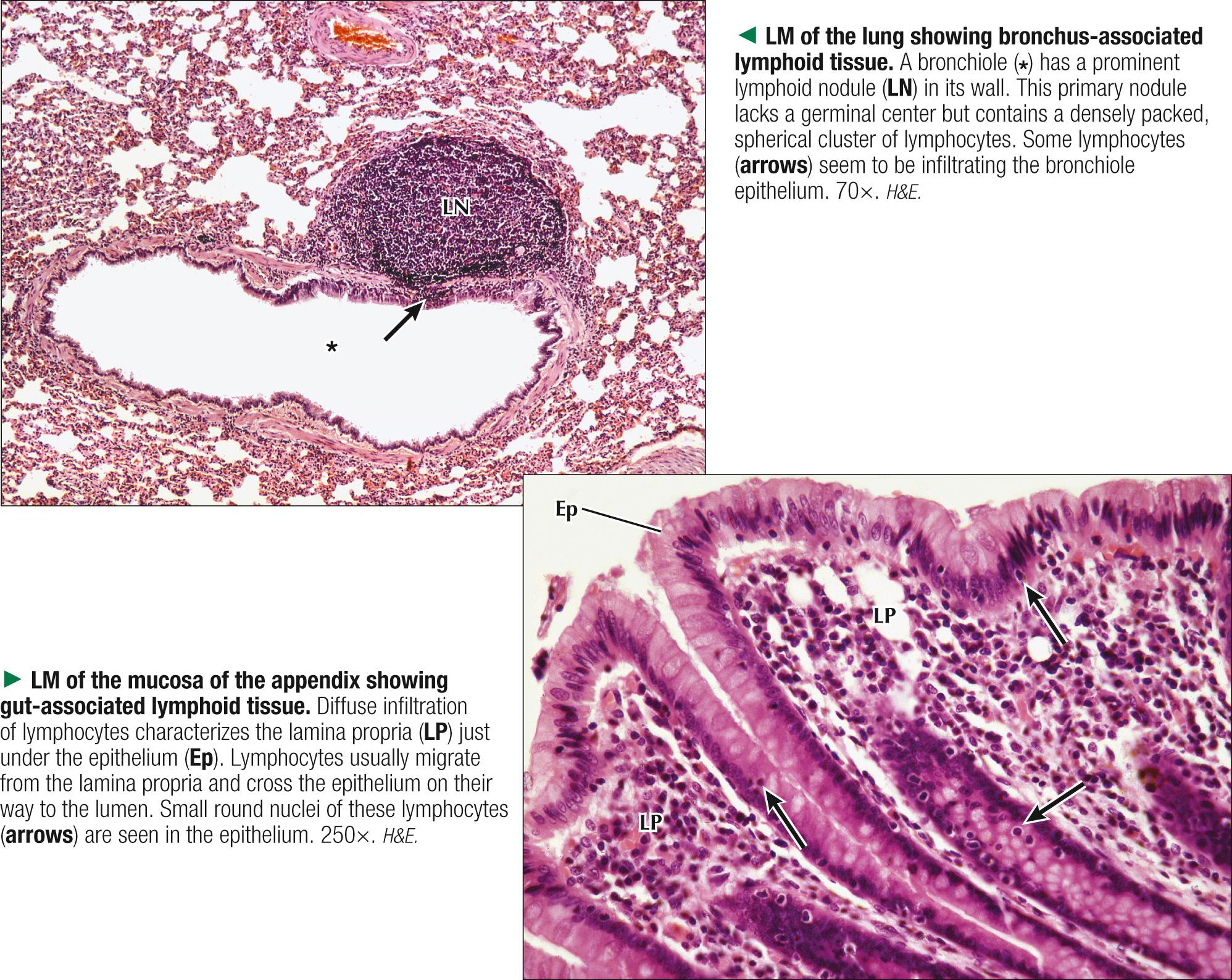
Mucous membranes of the gastrointestinal, respiratory, and genitourinary tracts are open to the external environment, so they harbor the body's largest, most diverse populations of microorganisms and pathogens. Extensive mucosal surfaces lead to vulnerability to infection. The diffuse lymphoid tissue common in the connective tissue— lamina propria —of these membranes is known as MALT. MALT may be subdivided, on the basis of location, into gut-associated (GALT), bronchus-associated (BALT), nose-associated (NALT), and vulvovaginal-associated (VALT) lymphoid tissue. GALT includes tonsils, Peyer patches, appendix, and less organized lymphocyte infiltrations scattered along the gastrointestinal tract. MALT is characterized by lymphocyte infiltrations, which are not sharply delineated from surrounding connective tissue but are supported by a loose framework of reticular fibers. Lymphocytes in these areas may also form lymphoid nodules (or follicles ), which are dense aggregations of lymphocytes arranged as spherical, unencapsulated clusters. There are two types, primary and secondary: a primary nodule contains small, immature B lymphocytes. In response to antigen exposure, primary nodules become secondary nodules, which contain pale-stained germinal centers. They are sites of extensive B lymphocyte proliferation and differentiation into plasma cells for antibody production. The major antibody (or immunoglobulin) formed in MALT is secretory IgA, which, after being produced by plasma cells, is actively transported via mucosal epithelial cells to the mucosal lumen. Although MALT contains both B and T cells, B cells predominate in nodules and T cells are abundant in adjacent areas. Also, specialized epithelial cells called M cells are abundant in the dome epithelium of Peyer patches. They take up small particles, such as bacteria and viruses, which are then engulfed by submucosal macrophages that process material and present it to B and T cells.
Infectious diseases caused by various microorganisms—bacteria, viruses, fungi, and parasites—develop when defense mechanisms of the host immune system cannot combat continual exposure to the pathogens. Rubella, commonly called German measles, is a contagious illness caused by rubella virus; its hallmark is an erythematous maculopapular rash plus fever and swollen lymph nodes. The portal of entry for the virus is the upper respiratory tract (NALT) through lymphoid tissue, where it reproduces intracellularly in a susceptible host. Rubella occurs mainly in children and young adults; in pregnant women it poses a serious risk to a fetus. A vaccine has greatly reduced the incidence of the disease.
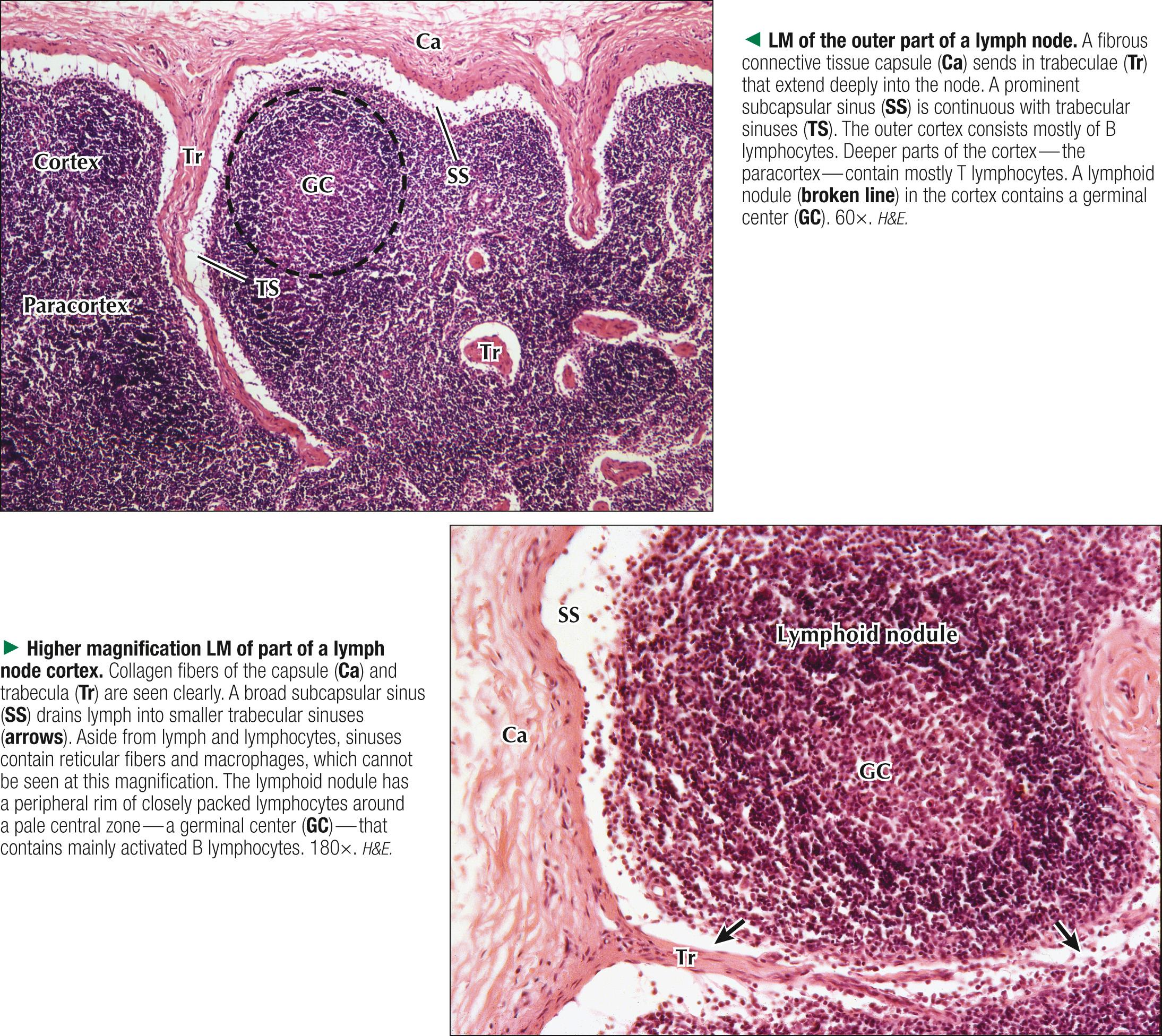
Lymph nodes are bean- or kidney-shaped lymphoid organs, 2-20 mm in diameter; 500-600 nodes are found in the body. They are seen along lymphatic vessels, and lymph percolates through them. They occur, often as chains or groups, in strategic regions such as the neck, groin, mesenteries, axillae, and abdomen. Lymph nodes derive originally from mesenchyme. During development, specific regions of each node are seeded with B lymphocytes from the bone marrow and T lymphocytes from the thymus. Main functions of lymph nodes are filtration of lymph before its return to the thoracic duct; production of lymphocytes that are added to lymph; synthesis of antibodies (mainly IgG); and recirculation of lymphocytes by their selective reentry from blood to lymph across walls of specialized efferent lymphatics. An outer capsule of dense fibrous connective tissue that typically merges with surrounding tissues and fat invests each node. It sends delicate, radiating partitions called trabeculae into the interior of the nodes. These beam-like structures of collagen fibers provide support and serve as conduits for blood vessels supplying the nodes. Between trabeculae is an internal stroma of reticular fibers organized three-dimensionally in which mainly lymphocytes are suspended. Specialized fibroblast-like cells (reticular cells), fixed macrophages, and dendritic (antigen-presenting) cells are also associated with the reticular fiber network.
Lymph nodes can undergo hypertrophy and histologic change in response to many clinical conditions. Abnormal enlargement of lymph nodes, or lymphadenopathy, may be due to increased numbers of lymphocytes and macrophages in the node during antigenic stimulation in a bacterial or viral infection. It may also be caused by metastasis, whereby neoplastic cells spread from a local site of development to distant locations. Such cells are often carried by lymphatics to the nearest lymph node. Surgical biopsy and microscopic examination of a lymph node are used for diagnosis and staging of many malignancies and may provide useful prognostic information.
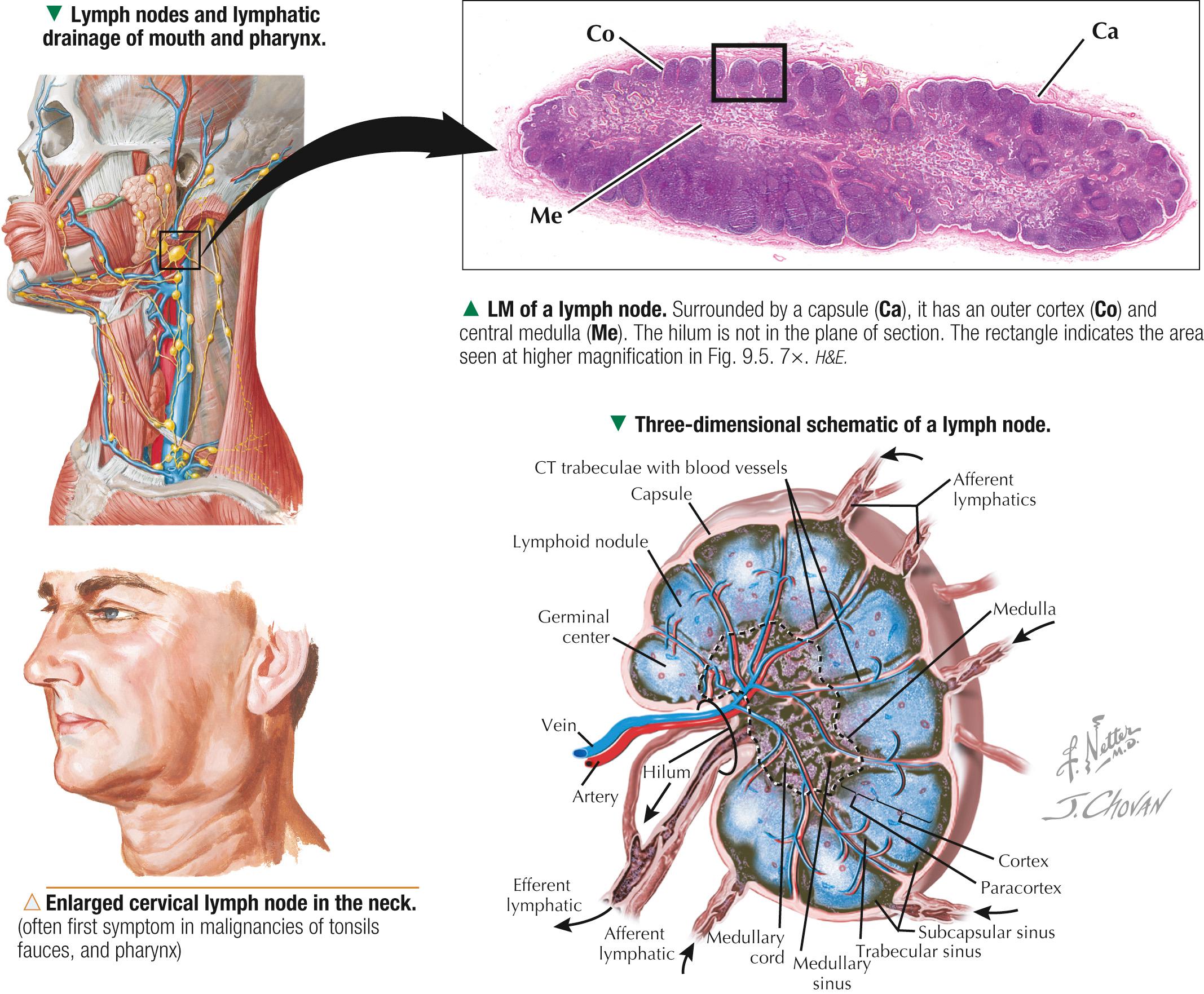
Lymph nodes contain aggregates of lymphocytes organized into an outer cortex, a paracortex, and an inner medulla. The darkly stained cortex just under the capsule consists of lymphoid nodules. In highly characteristic positions in the node, B cells occupy lymphoid nodules in the cortex, and T cells are in the paracortex, or thymus-dependent region. B cells in the nodules are those that originated from bone marrow (equal to the bursa of Fabricius in chickens). The cortex has two types of nodules. Primary nodules are spherical aggregates of tightly packed B cells in a meshwork of reticular fibers. After antigenic stimulation, primary nodules develop into secondary nodules, which have a germinal center surrounded by a mantle zone. Germinal centers are major sites of B cell proliferation and contain small and large lymphocytes, lymphoblasts, and follicular dendritic cells. The surrounding mantle zone contains small lymphocytes. Antigen-dependent T cell differentiation and proliferation occur in the paracortex, beneath and between nodules.
Lymphocytes can undergo intense mitotic activity, so neoplastic mutations of these cells are common. Lymphomas are localized lymphocyte malignancies that often form solid tumors, mainly affecting lymph nodes. Disease usually spreads from one node to another. Hodgkin disease (HD) is a major type of lymphoma distinguished by the presence of Reed-Sternberg cells in lymph nodes. The origin of these large cells is unknown, but a unique morphology allows identification in biopsy samples: a bilobed nucleus and prominent nucleoli often resemble owl eyes. In contrast to non–Hodgkin lymphoma, HD responds well to radiation and standard chemotherapy.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here