Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

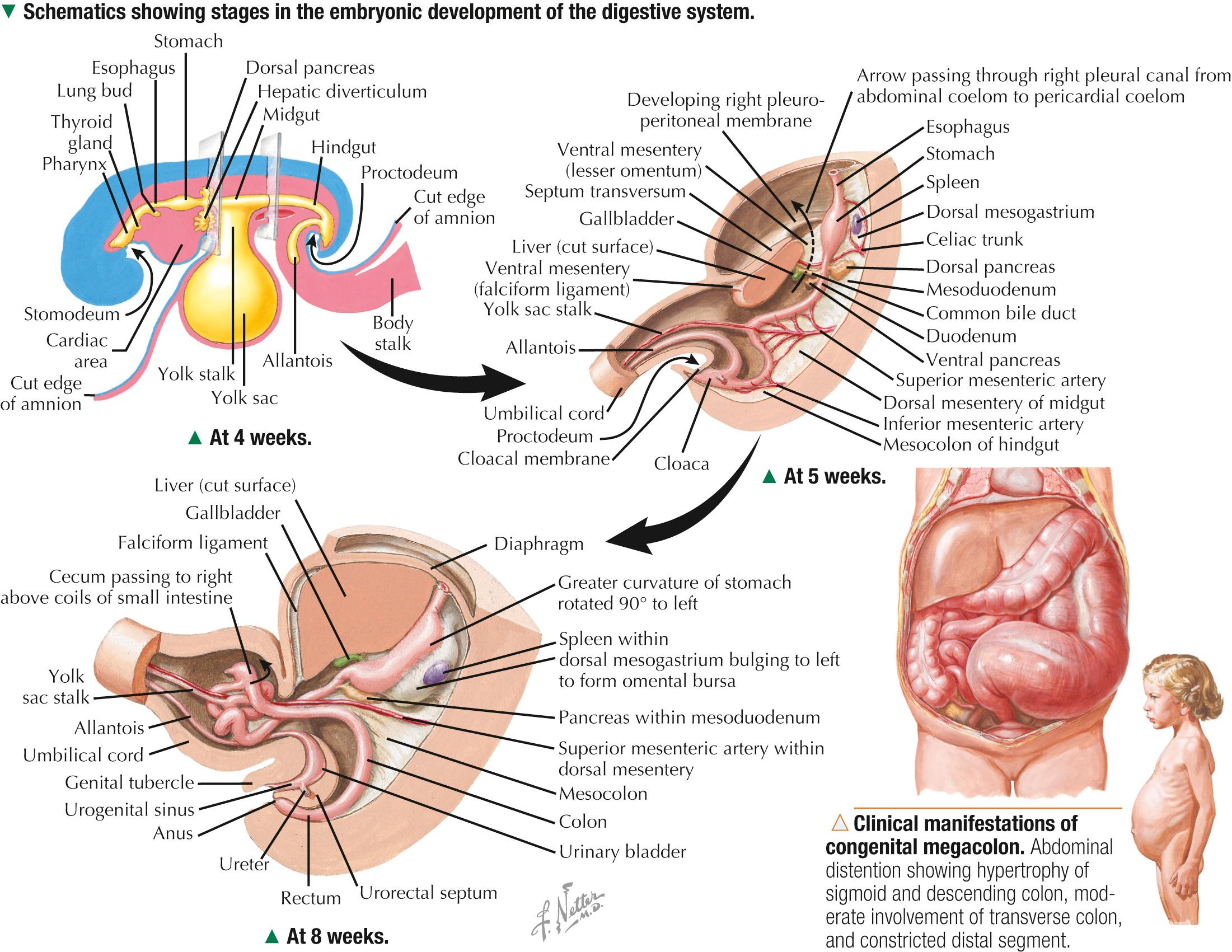
The early embryo starts as a flattened, trilaminar disc with three primary germ layers: ectoderm, mesoderm, and endoderm. Its ventral surface, covered by endoderm, communicates with the yolk sac. Later, lateral and cephalocaudal folding forms a long, cylindrical endodermal tube extending the length of the embryo; this becomes the primitive gut tube and then the digestive tract. Splanchnic mesoderm externally surrounds an endodermal lining. In the head area, the proximal part of the tube gives rise to the foregut. The caudal part, which extends into the tail, becomes the hindgut. A midgut in the center at first communicates with the yolk sac but then loses the connection. The endoderm becomes mucosal epithelium of the digestive tract and gives rise to the parenchyma and ducts of all intramural and accessory digestive glands. The overlying mesoderm becomes connective tissue, muscle, lymphatics, and blood vessels in the tube's wall. Neural crest ectoderm migrates to the gut wall to give rise to myenteric and submucosal neural plexuses. The foregut gives rise to the pharynx, esophagus, stomach, proximal duodenum, liver, gallbladder, and pancreas. The midgut becomes the rest of the duodenum, small bowel, cecum, ascending colon, and proximal transverse colon. The hindgut forms the rest of the transverse colon, descending colon, sigmoid colon, and rectum. The foregut rotates 90 degrees clockwise; the midgut, 270 degrees around its blood supply. Sheet-like mesenteries, derived from splanchnic mesoderm, suspend and attach parts of the tube to the body wall and serve as conduits for blood vessels, nerves, and lymphatics.
A wide spectrum of congenital disorders affecting different regions of the gastrointestinal tract may result in significant complications, mostly in infants and children and less frequently in adults. Congenital megacolon ( Hirschsprung disease )—the most common gut motility disorder caused by failure of migration of neural crest cells to the hindgut during weeks 5-12 of gestation—leads to partial or complete obstruction, usually of the sigmoid colon and rectum, with aganglionic segments that lack Meissner and Auerbach plexuses . Meckel diverticulum —the most prevalent developmental anomaly of the bowel—is a small outpocketing (usually about 5 cm long) of the gastrointestinal tract caused by incomplete obliteration of the vitelline ( yolk sac ) stalk in the seventh gestational week. Usually asymptomatic, it may sometimes lead to intestinal obstruction, perforation, and bleeding.
The stomach, the most dilated part of the digestive tube, is an expandable fibromuscular sac that connects the esophagus to the small intestine. In adults, it can hold about 1.5 L, or up to 3 L when distended. It stores and mixes food and reduces it to a semisolid mass, known as chyme, which it delivers to the duodenum. The stomach has four anatomic regions: cardia, fundus, body, and pylorus. As in other parts of the digestive tract, the wall has four concentric layers: mucosa, submucosa, muscularis externa, and serosa. The mucosa is 0.3-1.5 mm thick. The inner lining shows irregular longitudinal folds, known as rugae, which can be seen by the naked eye in a contracted stomach. They flatten as the stomach expands. Simple columnar epithelium of surface mucous cells lines the lumen. This epithelium regularly dips to form small gastric pits, or foveolae, which lead to long tubular gastric glands. The total number of glands is about 15 × 10 6 . Gastric pits and glands provide up to 800 m 2 of total surface area for secretion of mucus, acid, and digestive enzymes. The three types of glands have the same general structural plan but with regional histologic variations. Cardiac glands, in a small area around the esophageal (cardiac) orifice, are shortest, least numerous, and occupy less than 10% of the mucosa. In the body and fundus, main gastric glands, the largest and most numerous, make up about 75% of the mucosa. The pyloric area close to the duodenum contains small pyloric glands that constitute about 15% of the mucosa and resemble cardiac glands.
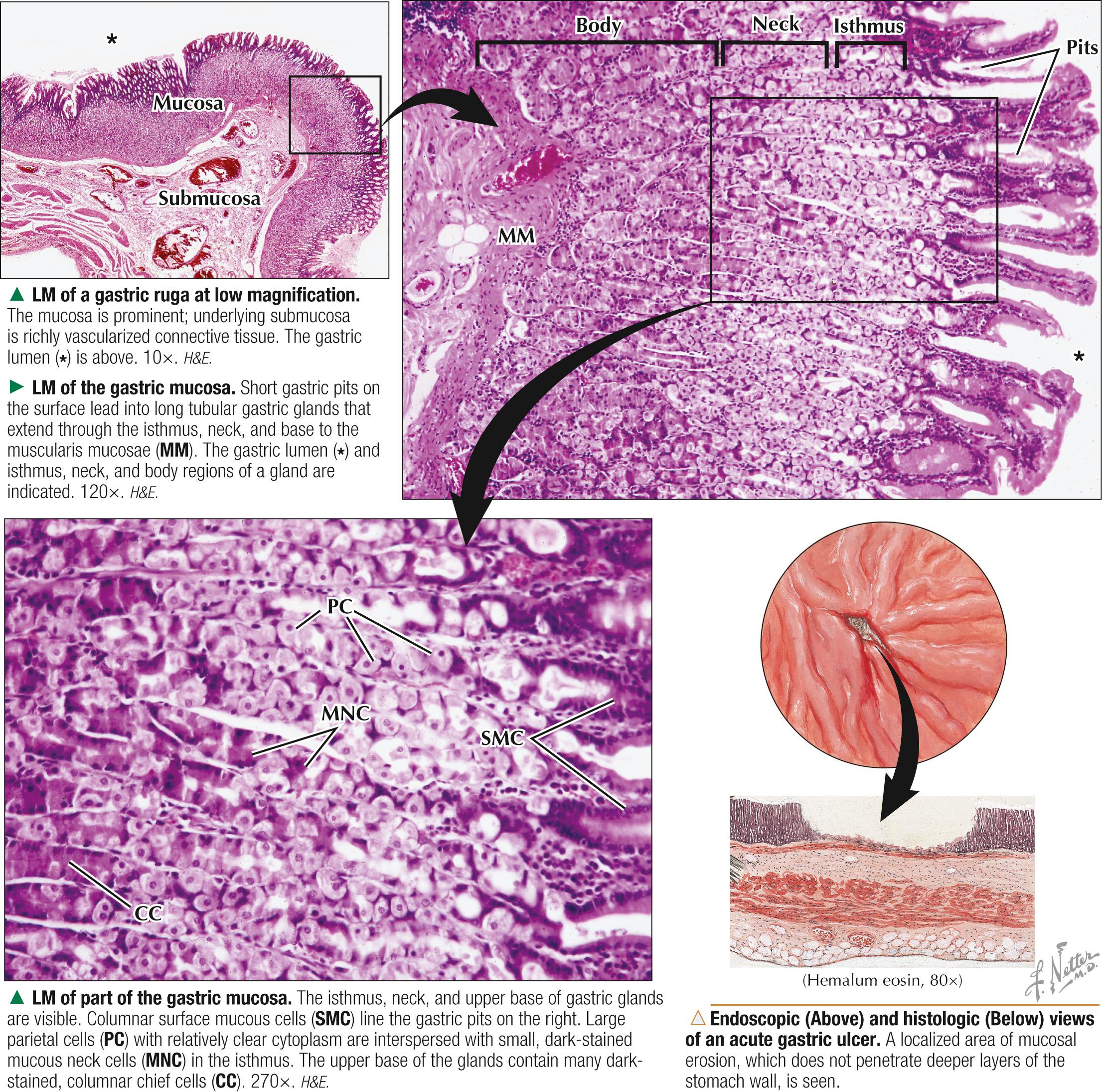
Gastritis — acute or chronic inflammation of the gastric mucosa—may be erosive or nonerosive. Symptoms include upper abdominal pain, indigestion, nausea, and vomiting. The most common diagnostic test is gastroscopy —passage from mouth to stomach of a thin, flexible tube with a camera attachment—for inspection of the gastric mucosa. In some cases, biopsy samples are removed via the gastroscope for more precise histologic evaluation. Erosive gastritis may lead to mucosal ulcerations, hemorrhage, or hematemesis; the most common causes are prolonged use of nonsteroidal antiinflammatory drugs (NSAIDs), excessive alcohol consumption, radiation, and chemotherapy. Treatment includes use of histamine H2-receptor blockers, antacids, and proton pump inhibitors .
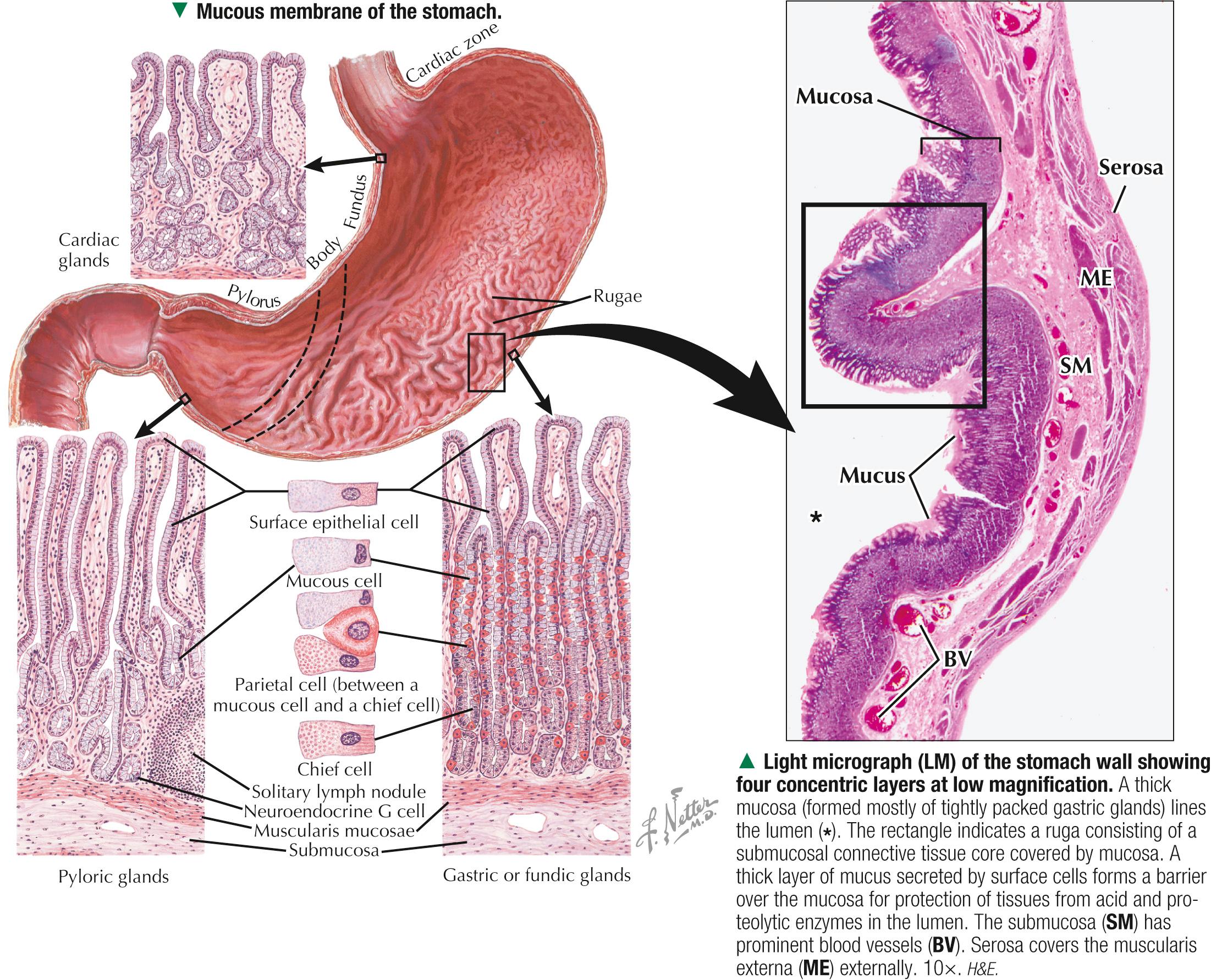
Gastric mucosa consists of a simple columnar epithelium, underlying lamina propria, and deeper muscularis mucosae. Surface mucous cells line the luminal surface and gastric pits. Several gastric glands discharge contents into the bottom of each pit. The glands occupy the entire thickness of the mucosa and extend through the lamina propria to the muscularis mucosae. The loose, richly cellular lamina propria under the surface epithelium and between the glands contains various connective tissue cells and an extensive capillary network. Mucosal glands are so tightly packed that the lamina propria is hard to see and usually appears scanty. The main gastric glands, the most specialized glands, are long, straight, and often bifurcated. In longitudinal section, glands (especially those in the fundus) have three parts. The upper part—the isthmus —opens into the gastric pit. The midregion—the neck —contains a mixture of mucous neck cells and parietal cells. Both isthmus and neck contain proliferating stem cells, which give rise to cells in the glands, plus those on the surface. The bottom part is the body (or main part): the upper area contains parietal cells plus gastric chief cells; the lower, the base, contains mostly chief cells. Cardiac and fundic glands (compound tubular glands) contain mostly mucus-secreting cells.
A thin film of mucus secreted by surface mucous and mucous neck cells forms a highly viscous barrier that protects the stomach surface. The mucus consists mostly of glycoproteins rich in carbohydrates and bicarbonate (HCO − 3 ) ions. It counteracts effects of HCl and proteolytic enzymes in the gastric lumen. Surface mucous cells—tall columnar epithelial cells with basal nuclei —form a continuous layer that lines the whole gastric lumen. The cells rest on a basement membrane (not easily seen by light microscopy). Junctional complexes link lateral cell borders. Apical parts of the cells are filled with mucin granules, which account for pale-staining, washed-out cytoplasm. Surface mucous cells also contain many mitochondria (best seen by electron microscopy), which provide energy for HCO − 3 secretion into the lumen. Surface mucous cells extend into gastric pits, which lead into densely packed, branched tubular glands. Mucous neck cells in the upper (neck) parts of the glands are smaller and more cuboidal than are surface mucous cells in gastric pits and on the luminal surface. Hard to see in hematoxylin and eosin (H&E) sections, they are better visualized with periodic acid–Schiff. Cells have a flattened basal nucleus and apical mucin granules. Unlike surface cells, whose mucus is alkaline, mucous neck cells elaborate a more acidic or neutral mucus such as sialomucin.

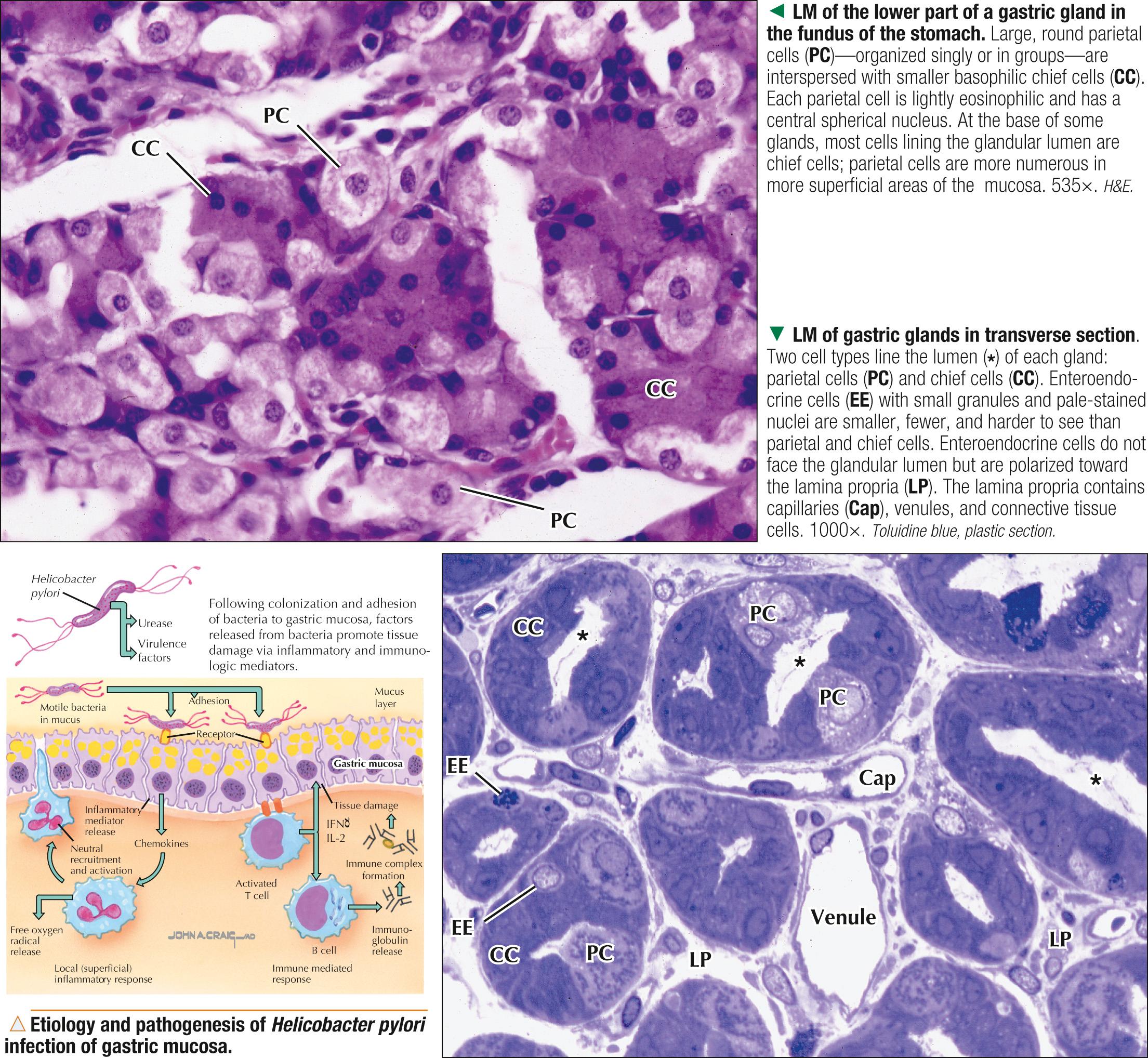
Main gastric glands in the mucosa of the fundus and body of the stomach are long, straight and branched tubular glands, which are perpendicular to the mucosal surface. Several glands usually open into the base of a gastric pit. Proliferating stem cells are in the isthmus and neck of the gastric glands. They migrate either up to renew cells on the surface or down to give rise to other cells deeper in gastric glands. Parietal cells are most numerous in the body of the glands but are also mixed with mucous neck cells in neck areas or with chief cells in basal areas of glands. They are large (20-35 µm in diameter), rounded or polygonal cells with one central nucleus. Their deeply eosinophilic cytoplasm is due to abundant mitochondria and relative paucity of rough endoplasmic reticulum. Cuboidal to columnar chief cells, mostly in basal parts of glands, have a round basal nucleus. Their basal cytoplasm is basophilic; secretory (zymogenic) granules make their apical cytoplasm look more granular. Gastric glands also contain less numerous enteroendocrine cells, scattered with the other cells, that produce gut hormones and are hard to see in routine sections. Special immunocytochemical or electron microscopic methods are needed to identify them with certainty.
The gram-negative bacterium Helicobacter pylori inhabits gastric mucosa. Its mode of transmission is unclear, but infection rates are high in populations in developed (40%) and underdeveloped (85%) countries. It may cause inflammation of the stomach ( gastritis ) and gastric ulcers via urease, which damages the mucosa. Chronic infection may lead to gastric adenocarcinoma. Diagnosis is by endoscopic or histologic study of the mucosa and stool antigen and blood antibody tests. Treatment with antibiotics is usually very effective.
Parietal cells secrete high concentrations of HCl, pH 0.8-2, into gastric gland lumina. Trench-like infoldings of apical cell membranes form a ramifying network of narrow channels (1-2 µm wide)—the secretory canaliculi. They occur throughout the cytoplasm and near the nucleus and open into glandular lumina. Canaliculi are lined by many densely packed microvilli for increased surface area. Membranes of canaliculi and microvilli contain the proton pump H + ,K + -ATPase for acid secretion. Many mitochondria in the cytoplasm constitute up to 40% of cell volume, have densely packed cristae with many matrix granules, and provide energy for ion transport. Lysosomes are common and engage in turnover of organelles by autophagocytosis. An elaborate tubulovesicular system, which has Cl − and K + conductance channels, also occurs near cell surfaces and canaliculi. Resting cells not producing HCl have many tubulovesicles, which during active secretion fuse with canaliculi membranes. The resulting decrease in tubulovesicle number occurs together with a large increase in microvilli and canaliculi. H + ions are actively transported across apical cell membranes and unite with luminal Cl − ions to form HCl. Infoldings of basal plasma membrane also increase surface area to facilitate HCO − 3 transport in exchange for Cl − . Basal membranes bear receptors for acetylcholine, gastrin, and histamine, which stimulate acid secretion. Parietal cells also synthesize intrinsic factor, a glycoprotein that facilitates vitamin B 12 absorption in the proximal small intestine. For this function, the base of the cells contains a small Golgi complex, a few free ribosomes, and rough endoplasmic reticulum.
Vitamin B 12 (also called cobalamin ) is essential for production of erythrocytes in bone marrow and normal neurologic function. Pernicious anemia —a form of megaloblastic anemia —is an autoimmune disease resulting in marked atrophy of gastric mucosa, destruction of parietal cells, and failure to produce intrinsic factor, which leads to vitamin B 12 malabsorption . Symptoms include fatigue, asthenia, memory impairment, and peripheral neuropathy. The diagnosis is based on histologic findings of chronic atrophic gastritis and detection in serum of antibodies to intrinsic factor and the proton pump (H + , K + -ATPase) of parietal cells. Patients respond favorably to early detection, continuing treatment via intramuscular injections of cobalamin, and a well-balanced diet rich in folic acid and vitamin B 12 .

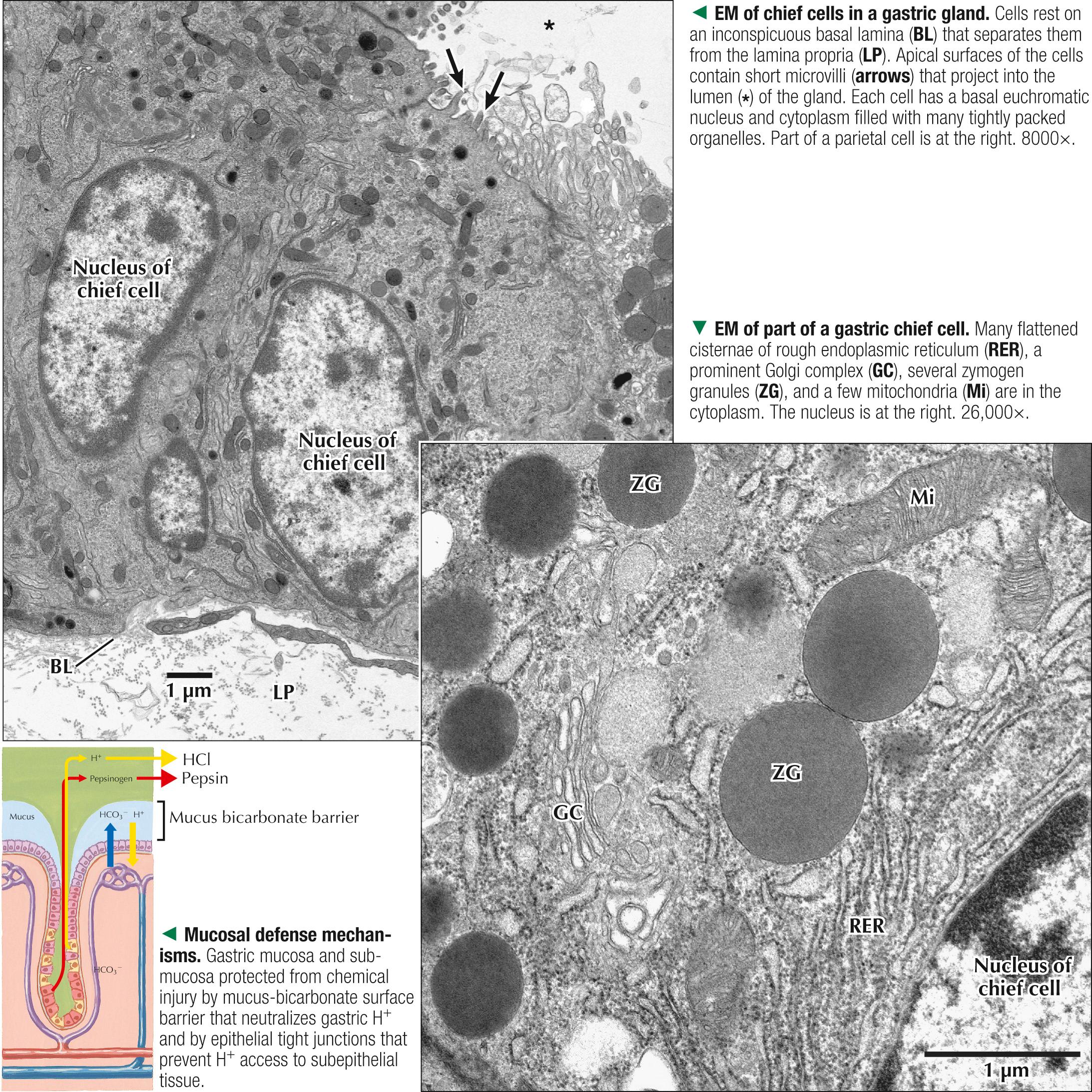
Chief cells produce two distinct groups of proteolytic enzymes, called pepsinogen I and II, as inactive proenzymes. These classic protein-synthesizing cells have a basal nucleus and organelles for synthesis and secretion of protein. Their ultrastructure closely resembles that of pancreatic acinar cells. The basal aspect of each pyramidal cell rests on a basal lamina; its apical border contacts the gastric gland lumen. The basal cytoplasm contains extensive rough endoplasmic reticulum and many free ribosomes, which account for intense basophilia in H&E sections. The supranuclear cytoplasmic region has a prominent Golgi complex. Mitochondria are scattered in the cytoplasm and are especially large and numerous during cell secretion. Large, electron-dense membrane-bound secretory vesicles, the zymogen granules, are a salient feature of apical cytoplasm and emanate from the concave side of the Golgi. They discharge their contents by exocytosis —fusion of their limiting membranes with apical plasma membranes. Luminal plasma membranes contain short stubby microvilli that amplify surface area for secretion. Released pepsinogen is converted to pepsin, the active form of the enzyme, because of the low intraluminal pH in gastric glands. Chief cells also produce lipase, another digestive enzyme.
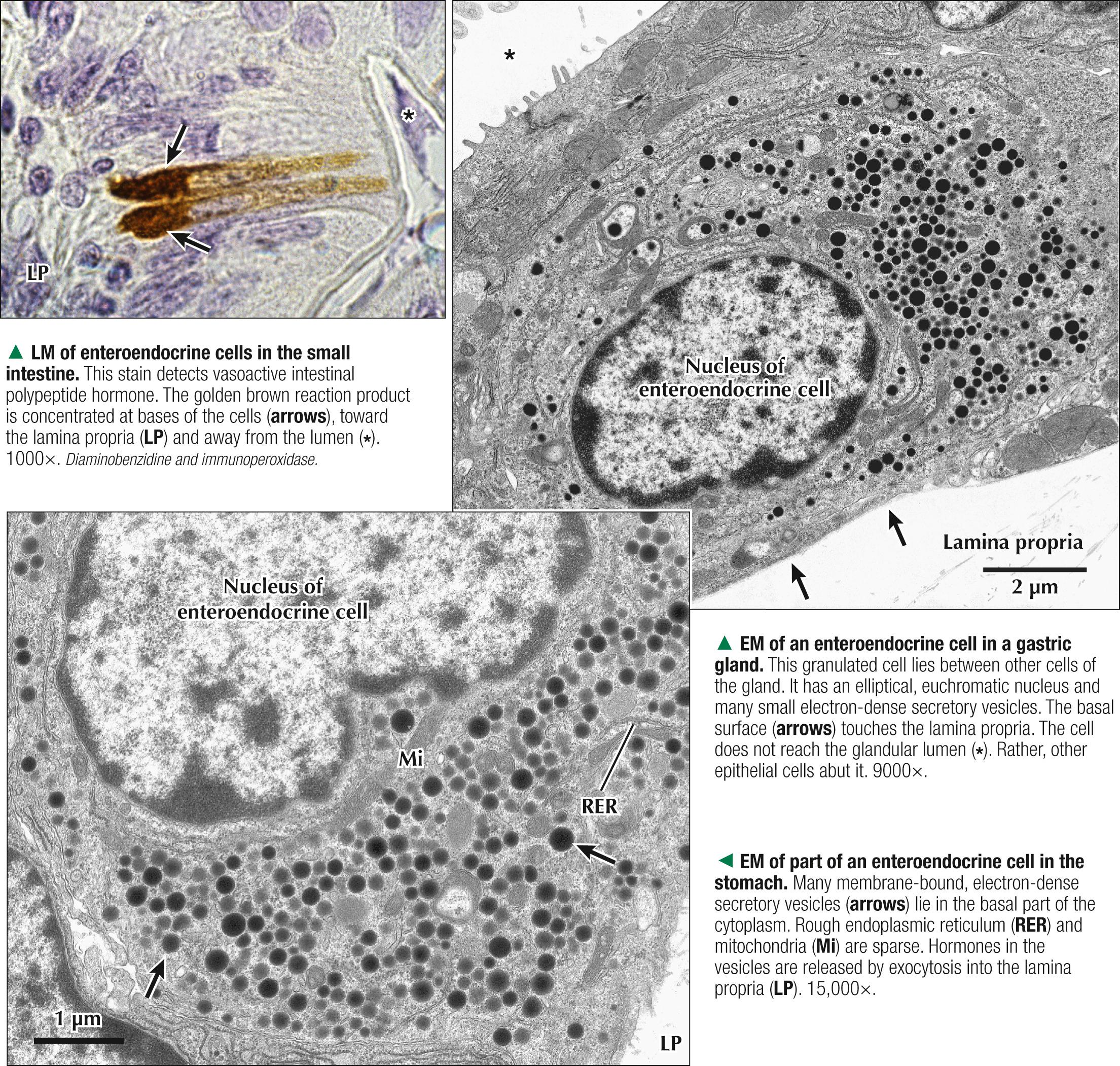
Enteroendocrine cells—hormone-producing cells of the gastrointestinal tract—are small pyramidal cells that are diffusely scattered in the epithelium, from the esophagus to the colon. Probably derived embryonically from endoderm, they are widespread in the mucosal lining, gastric glands, intestinal glands, and villi. They are called argentaffin, argyrophil, or APUD (amine precursor uptake and decarboxylation) cells on the basis of metabolic and staining properties. Cells are hard to see in routine sections, but immunocytochemistry and electron microscopy can reveal them. They make up a family of cells that belong to the diffuse neuroendocrine system; grouped together, these cells would form the largest endocrine organ in the body. The cell types are classed according to specific secretory product, but all conform to the same ultrastructural plan. Some may reach the lumen; most do not extend to the surface and are on the basal lamina, where they face the lamina propria. All have small, membrane-bound, electron-dense secretory vesicles concentrated in basal cell areas. One elliptical nucleus is usually euchromatic. The cytoplasm has a small Golgi complex, a few mitochondria, and scattered elements of rough endoplasmic reticulum. Cells produce various peptides and amines, which enter the bloodstream or act locally, with powerful effects on target cells. More than 30 gastrointestinal hormones, such as gastrin, motilin, cholecystokinin, somatostatin, secretin, and vasoactive intestinal polypeptide, are produced.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here