Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

The continued success of liver transplantation over the past quarter century can be attributed to a number of factors: better understanding of disease pathophysiology, enhanced intraoperative management, and improved posttransplantation care, to name a few. Atop this list, however, is the introduction of new immunosuppressive agents, all of which have contributed to improved graft and patient survival. Like any medication, these agents are not without side effects. This chapter focuses on the long-term toxicities of frequently used immunosuppressive medications.
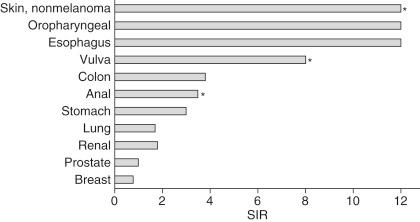
The goal of immunosuppressive therapy is to dampen the immune response at the time of transplantation. Unfortunately, these agents are not specifically targeted against the immune response to the transplanted organ. As a result, other protective functions of the human immune system are jeopardized. Among them is the body’s ability to neutralize malignantly transformed cells, particularly those driven by viral infection. As such, one of the long-recognized side effects of immunosuppression is an increased risk for selected malignancies. The most common malignancies among transplant recipients are nonmelanomatous skin cancers, which may affect nearly a quarter of liver transplant recipients. Other more life-threatening cancers, however, are present at elevated rates in this patient population and generally involve the gastrointestinal (GI) tract, and in particular GI malignancies with the human papillomavirus ( Table 97-1 ). In a recent analysis of all solid organ transplant recipients using the U.S. Organ Procurement and Transplantation Network (OPTN)/United Network for Organ Sharing (UNOS) database, the overall incidence of posttransplantation malignancy in liver transplant recipients was 4.46%, with GI cancers (as a whole) being the most common type.
Regardless of malignancy type, standard preventative practices (e.g., smoking cessation, sun protection, breast self-examinations) and routine cancer screening examinations (e.g., chest x-ray, colonoscopy, dermatological evaluation) should be highly encouraged after transplantation and incorporated into the posttransplantation management pathway for all recipients.
More specific to the transplant population is the collection of lymphoid malignancies known as posttransplantation lymphoproliferative disorder (PTLD). This was the single most common type of cancer reported among liver transplant recipients in the recent review by Sampaio et al. PTLD differs from lymphomas seen in immunocompetent patients in that it may present outside of nodal tissue, tends to arise (and regress) rapidly, and is frequently driven by Epstein-Barr virus (EBV). Indeed, the greatest risk for PTLD is seen in EBV-seronegative patients who receive an EBV-seropositive organ. Thus PTLD may reasonably be considered an infectious disease risk with oncological sequelae rather than a case of direct oncological transformation. Accordingly, PTLD responds to reduction or withdrawal of immunosuppression in approximately 50% of affected individuals, making prompt and aggressive reduction of immunosuppression the first therapeutic maneuver upon diagnosis. In a long-term follow-up study of liver transplant patients at the Mayo Clinic in Rochester, Minnesota, the overall incidence of PTLD was 3.1% with EBV-negative disease predominating later after transplantation ( Fig. 97-1 ).
-positive and EBV-negative posttransplantation lymphoproliferative disorder (PTLD) in liver transplant recipients.")
PTLD may occur anytime after transplant and usually presents with the typical viral prodrome of malaise, fever, and weight loss. Laboratory findings typically include an elevated l -lactate dehydrogenase level and EBV viremia. Graft involvement and central nervous system invasion, as well as multiple site involvement, are poor prognostic factors. Diagnosis requires biopsy-proven disease of the affected organ or lymph node. Oncological evaluation is required. An elevated EBV level on polymerase chain reaction, although not diagnostic, may be suggestive of PTLD and can be used to gauge its course. Treatment consists primarily of immunosuppression withdrawal, allowing the patient to mount a response against EBV and PTLD. In addition, antiviral directed therapy (e.g., ganciclovir) is started. When withdrawal is insufficient, adjuvant therapies, including irradiation and chemotherapy, may be considered, typically CHOP (cyclophosphamide, hydroxydaunomycin [doxorubicin], Oncovin [vincristine], and prednisone)-based regimens.
Rituximab, an anti-CD20 antibody, may lead to remission in certain cases of PTLD. Early-onset PTLD is frequently B cell in origin and CD20 positive, making Rituximab a viable option and an often-used adjuvant to standard chemotherapeutic agents. Late-onset PTLD is usually non-Hodgkin’s lymphoma and is not viral related.
Another complication of immunosuppressive therapy is the development of posttransplantation infections. The vast majority of infections occur within the first 6 months after transplantation, when the intensity of immunosuppression is at its highest. However, infections may happen at any time and generally occur in a predictable pattern after transplant ( Table 97-2 ). Common and life-threatening opportunistic infections are addressed in detail in Chapter 78 . Long term, the risk for infection persists and is still directly related to a patient’s level of immunosuppression. Thus patients undergoing treatment for rejection remain at a high risk for infection, even after therapy has ceased. Although serious bacterial and fungal infections predominate early after transplantation, viral conditions prevail over the long term. These include reactivation of latent herpes viruses, including cytomegalovirus (CMV), EBV, herpes simplex, or herpes zoster. The relationship of these reactivations leads many to reinstitute viral-specific prophylaxis when treating for rejection (e.g., ganciclovir).
| Less Than 1 Month After Transplantation | 1-6 Months After Transplantation | More Than 6 Months After Transplantation |
|---|---|---|
| Infection with antimicrobial-resistant species: MRSA VRE Candia species (non-albicans) Aspiration Catheter infection Wound infection Anastomotic leaks and ischemia Clostridium difficile colitis Donor-derived infection (uncommon): HSV, LCMV, rhabdovirus (rabies), West Nile virus, HIV, Trypanosoma cruzi Recipient-derived infection (colonization): Aspergillus , Pseudomonas |
With PCP and antiviral (CMV, HBV) prophylaxis: BK polyomavirus infection, nephropathy C. difficile colitis HCV infection Adenovirus infection, influenza Cryptococcus neoformans infection Mycobacterium tuberculosis infection Anastomotic complications Without prophylaxis: Pneumocystis Infection with herpesviruses (HSV, VZV, CMV, EBV) HBV infection Infection with Listeria , Nocardia , Toxoplasma , Strongyloides , Leishmania , T. cruzi |
Community-acquired pneumonia, urinary tract infection Infection with Aspergillus , atypical Molds, Mucor species Infection with Nocardia , Rhodococcus species Late viral infections: CMV infection (colitis and retinitis) Hepatitis (HBV, HCV) HSV encephalitis Community-acquired (SARS, West Nile virus infections) JC polyomavirus infection (PML) Skin cancer, lymphoma (PTLD) |
Hepatitis C recurrence is ubiquitous in infected individuals, although the phenotype of recurrence varies considerably from an asymptomatic carrier state to rapid hepatic deterioration. The primary approach for all these conditions includes reduction of immunosuppression in addition to targeted antiviral therapy against hepatitis C. Nearly 100 antiviral agents have been developed against hepatitis C, which are in various experimental phases. The two recently approved agents, boceprevir and telaprevir, are both protease inhibitors that, when used in combination with pegylated interferon and ribavirin, have been shown to improve cure rates with a shorter duration of therapy.
Although the immunocompromised state is the principal reason behind posttransplantation infections, attentiveness to other perioperative factors may help to mitigate the risks. This includes minimizing immunosuppression in recipients who are ill or deconditioned, who have overcome a recent infection, or who are hospitalized at the time of transplant. Specific issues common to patients recovering from hepatic failure include hypogammaglobulinemia and leukocytopenia and should be recognized as clues to limit the immunosuppressive load. Maneuvers to thwart any potential infection after transplantation include (1) treating any donor-related infections, (2) taking precautions against health care–associated bacterial infections (i.e., surgical site, catheter-associated, and urinary tract infections; ventilator-assisted pneumonias), and (3) providing prophylaxis against potential opportunistic infections via the routine use of antimicrobials such as trimethoprim-sulfamethoxazole, amphotericin, and ganciclovir.
Pioneering studies found that corticosteroids (CSs) could prolong skin graft survival in rabbits. Fifty years ago Starzl et al showed that CS, along with azathioprine (AZA), extended patient and graft survival after kidney transplantation. Today CSs remain a cornerstone of immunosuppressive therapy, both as an induction agent at the time of transplant and as a pulse agent in the treatment of posttransplantation rejection episodes. The long-term consequences of CS use are numerous and well known ( Table 97-3 ). Here we focus on some of the more common complications of CS use in liver transplantation.
| System | Long-Term Side Effects |
|---|---|
| Cardiovascular | Sodium and fluid retention, hypertension, atherosclerosis |
| Gastroenterological | Gastritis, peptic ulcer, gastrointestinal bleeding, pancreatitis |
| Dermatological | Acne, increased bruising, impaired wound healing |
| Endocrine | Diabetes mellitus/glucose intolerance, cushingoid facies, hyperlipidemia, growth retardation, menstrual irregularities, hirsutism, weight gain—increased appetite, adrenal gland hormone suppression |
| Infectious | Increased risk for infections, including fungal |
| Musculoskeletal | Osteoporosis, vertebral and femoral fractures, osteonecrosis of femoral head; myopathy, muscle weakness |
| Ophthalmic | Cataracts, increased intraocular pressure, glaucoma, exophthalmos |
| Psychiatric | Psychosis, mood swings, depression, aggressive behavior, insomnia |
A well-known complication of long-term CS use is diabetes, which occurs in up to 40% of adult liver transplant recipients. CS-induced diabetes results in impaired glucose metabolism through increased insulin resistance. The mechanisms resulting in hyperglycemia include (1) a reduction in insulin production, (2) an increase in gluconeogenesis, (3) a decrease in peripheral glucose utilization, and (4) reduced glycogen synthesis. These effects are thought to be dose dependent, because reduced doses of CS have been shown to decrease insulin resistance. In addition, CSs enhance appetite, particularly for sweetened foods. As will be described later, calcineurin inhibitors (CNIs) contribute significantly to the development of posttransplantation diabetes mellitus (PTDM). Even though many programs have employed steroid avoidance or low-maintenance-dose CS protocols, PTDM remains a considerable problem. Thus one can extrapolate that PTDM is primarily due to the CNI.
The prevalence of dyslipidemia has been documented in up to 45% of liver transplant recipients. The mechanism or mechanisms leading to dyslipidemia are not clear but may be due to steroid-induced insulin resistance, which leads to increased levels of very-low-density lipoprotein (VLDL), triglycerides, and low-density lipoprotein (LDL). Lipogenesis may also be pronounced with CS use.
The endocrine complications just described (diabetes and dyslipidemia) increase the risk for cardiovascular events after transplantation. Another risk factor contributing to cardiac disease is hypertension. The mechanisms involved in causing an increase in blood pressure include (1) sodium and water retention in the distal nephron, (2) upregulation of receptors present on vascular smooth muscle, and (3) contributions involving pathways in the central nervous system, adipose tissue, and liver.
Liver transplant recipients not previously diagnosed with hypertension may develop elevated blood pressure after transplantation. While no one medication can tackle all the mechanisms listed earlier, use of a calcium channel blocker and a diuretic (if merited) may prove effective as first-line therapy.
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here