Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Depends on site of injury:
Injury to a metacarpal or several phalanges: PA of hand and oblique of entire hand and wrist .
Injury to the thumb or to a single digit: PA and lateral of the digit .
Dislocations at 4th & 5th CMC joints.
Fractures at base of 4th or 5th MCs.
Fracture of the hamate.
CMC, carpometacarpal;
IPJ, interphalangeal joint;
MC, metacarpal;
MCPJ, metacarpophalangeal joint;
PA, posterior-anterior (view).
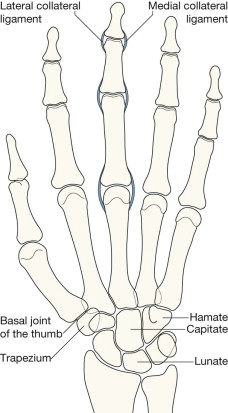
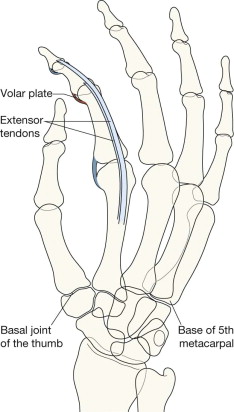
Knowledge of the anatomical attachments of (a few) tendons and ligaments is essential. A seemingly trivial fragment of bone on the radiograph may indicate that a particular tendon or ligament is no longer anchored to the bone. Failure to recognise the functional implication can lead to inappropriate management.
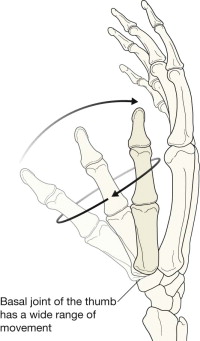
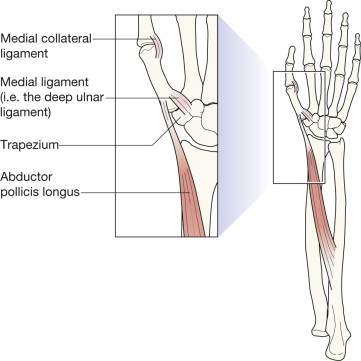
The stability of the carpometacarpal (CMC) joint of the thumb depends on fairly lax but very tough capsular ligaments . The deep ulnar ligament is the thickened part of the capsule on the palmar aspect of the 1st CMC joint. This strong ligament extends from the first metacarpal to the trapezium. The capsular ligaments and the shape of the first CMC joint (ie the trapezium–metacarpal joint) enables the thumb to adopt an extraordinary degree of mobility including the crucial ability of opposition.
1st CMC joint = basal joint of the thumb.
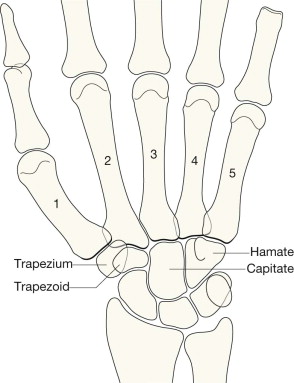
On the PA view of the hand:
The articular cortex at the base of each metacarpal parallels the articular surface of the adjacent carpal bone.
The CMC joint spaces are clearly seen; they are equal (approximately1–2 mm) in width.
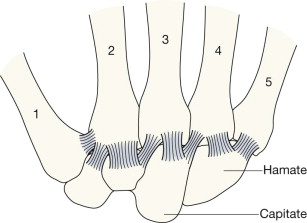
The 2nd to 5th CMC joints are visualised as a zigzag tram line (see opposite).
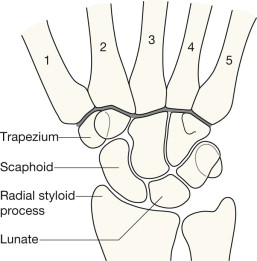
On the PA radiograph, the joint surfaces of the 2nd through to the 5th metacarpal and their adjacent carpal bones articulate, and their articular surfaces parallel one another. These joints are thus seen as a zigzag tram line , shown as a thick dark line on this drawing.
The zigzag line is analogous to “seeing the light of day” through each of the CMC joints.
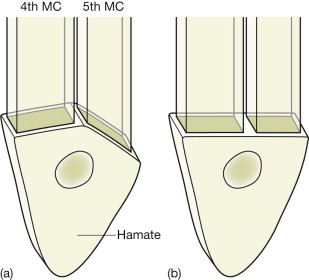
A stylised drawing of the important alignment between the bases of the hamate and the 4th and 5th CMC joints. Understanding the radiographic appearance of these two joints on the PA view is important. In some people the normal joints look like (a); in others the normal joints look more like (b).
See also pp. 167–168.
Target the precise clinical site of injury.
Search for fractures and for any evidence of subluxation/dislocation.
Review the relevant muscle and ligamentous attachments because a small fracture may indicate a big loss of function.

Check for fractures, dislocations, and subluxations; check whether the 4th and 5th carpometacarpal (CMC) joints show “the light of day” (p. 157); check the basal joint of the thumb; if there is a fracture of the 1st metacarpal determine whether it is intra-articular (Bennett's fracture) or extra-articular. This is a normal PA view.

Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here