Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Recent studies estimate that approximately 25 million individuals worldwide, including 1 million people in the United States, identify as transgender. Over the last several years, an increasing number of transgender women have pursued surgical interventions. Some 28% of transgender women report having undergone gender confirming surgical procedures, with 5%–13% of these surgeries involving genital procedures. Of the transgender women who have not undergone these surgeries, 45%–54% report hoping to do so in the future. The surgical management of individuals with gender dysphoria is often complex and benefits from a multidisciplinary approach. Recognizing and understanding the importance of a multidisciplinary approach helps the surgeon counsel and educate patients regarding available surgical options.
Vaginoplasty is one of the most commonly performed gender confirming surgeries, and is often the first procedure considered by transgender women. Vaginoplasty helps to relieve and/or alleviate gender dysphoria, improves psychosocial outcomes, and has high patient satisfaction. Research shows that surgery has a beneficial effect on both life satisfaction as well as general quality of life. A successful surgical result involves the creation of a natural-appearing vagina and mons pubis: this includes a feminine-appearing labia majora (smooth, graded, and contiguous appearance) and minora (moist appearance) with removal of the stigmatizing scrotum ( Fig. 14.2.1 ). Functionally, the neovagina should be able to accommodate receptive penetrative intercourse (when this is a stated preoperative goal), allow urination while sitting, and provide erogenous sensation.
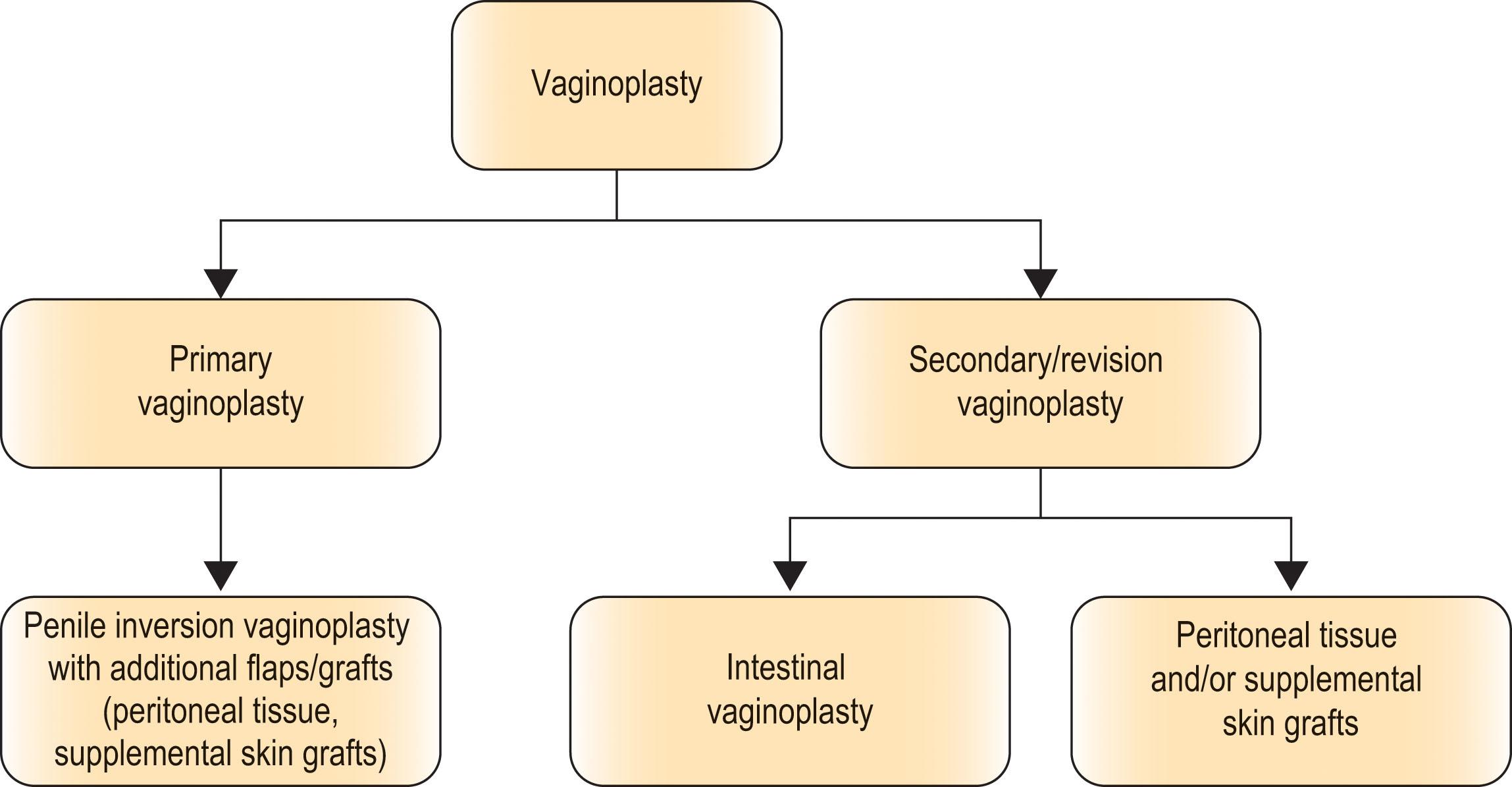
Vaginoplasty has undergone technical refinements, however, the anterior pedicled penile flap remains the mainstay. Vaginoplasty typically involves penectomy, orchiectomy, clitoroplasty, vulvoplasty, and the construction of a vaginal canal. Various surgical techniques are used to create the vagina and its lining, with the most common being a skin-lined neovagina (also known as penile-inversion vaginoplasty). Other methods include pedicled intestinal flaps (intestinal vaginoplasty), skin grafts from other anatomic sites (abdomen, flanks, buttocks, etc.), and/or peritoneal tissue.
During the surgical consultation, it is important to review and understand the patient’s goals and expectations. In addition, to reviewing the surgical options (including the risks and benefits), the limitations of surgery are also discussed. This discussion includes information regarding both appearance and function. In a follow-up study of 55 transsexual patients treated in Belgium, De Cuypere et al . noted that the transsexual person’s expectations were met at an emotional and social level, but less so at the physical and sexual level. This occurred despite an indicated improvement in sex life and sexual excitement after reassignment surgery. After deciding to proceed with surgery, written documentation of informed consent should be included in the patient’s chart.
Regardless of which technique is utilized, a preoperative bowel preparation is administered. Additionally, hair removal, whether by electrolysis or laser, is completed as thoroughly as possible from the penile shaft and central perineum and scrotum ( Fig. 14.2.2 ) prior to surgery. Preoperative depilation helps to prevent intravaginal hair growth.

Historically, hormones were discontinued approximately two weeks prior to surgery. The purpose of hormone cessation was to reduce the risk of venous thromboembolism. More recently, however, concerns about abrupt hormone withdrawal and potential adverse emotional and physiologic effects have been raised. This, along with what seems to be a low risk of VTE, has led many to try to re-evaluate perioperative hormone protocols. Specific recommendations regarding VTE prophylaxis are based upon an assessment of patient risk factors. Surgeons and clinicians prescribing hormones should collaborate regarding perioperative hormone therapy management, and a shared decision-making approach with patients can be utilized.
The penile inversion vaginoplasty is generally utilized for primary vaginoplasty ( Algorithm 14.2.1 ). The use of pedicled penile and scrotal flaps was described over 40 years ago, and despite technical refinements, remains the mainstay for neovaginal construction. This technique utilizes the penile skin, often in conjunction with supplemental scrotal skin grafts to provide vaginal lining. The vascular basis of these flaps is derived from one of two sources: (1) the femoral artery (deep and superficial external pudendal arteries) and (2) the internal pudendal artery (perineal branches).
Primary vaginoplasty surgery most commonly involves penile disassembly and inversion with an anteriorly based pedicled penile flap. The penile disassembly and inversion technique utilizes the penile skin and a second, posteriorly based, scrotal–perineal flap to construct the vaginal cavity. The author’s preferred technique is described herein: the labia majora are formed from the lateral aspects of the scrotum, the neoclitoris is formed from the dorsal glans penis, and the vestibular lining and labia minora are formed by a urethral flap and the penile skin. The penile urethra is shortened, spatulated, and everted to create the neo-urethral meatus. Depending upon the length of the penis and previous surgical history (i.e., circumcision), skin grafts may be required for additional vaginal depth. Full-thickness skin grafts may be harvested from the scrotum and perineum. Additional full-thickness skin grafts may be harvested from the groin, lower abdomen, or flanks.
Prior to surgery, sequential compression devices are placed, and intravenous antibiotics are administered. Following induction of general anesthesia, either fractionated or unfractionated heparin is administered subcutaneously, the patient is positioned in lithotomy, the patient is prepped and draped using a povidone-iodine solution, and a urinary catheter is inserted.
The procedure begins with the creation of a posteriorly based scrotal–perineal flap. The dimensions of this flap vary; however, most commonly a limited scrotal–perineal flap is used and ultimately inset into the anteriorly based penile flap. The lateral aspect of the flap is designed in a “V”-shaped fashion so as not to create a circular introitus, thereby minimizing the chance of introital contracture ( Fig. 14.2.3 ). The flap is centered cephalad to the anus such that the introitus will be formed at the location of the perineal body (i.e., central tendon). The flap is elevated with Colles fascia.

A full-thickness scrotal skin graft is then harvested. It is typically drawn in a “bat-wing” configuration and abuts the superior border of the perineal skin flap ( Fig. 14.2.3 ). The skin graft is defatted, depilated, and sutured over a dilator on a back table ( Fig. 14.2.4 ).

An incision is made on the ventral penis along the midline raphe. An additional circumferential incision at the junction of the glans penis and penile shaft is also made. In uncircumcised individuals, the foreskin is used to fashion the preputial skin of the clitoris. In individuals who are circumcised, less skin is available to construct the clitoral prepuce (the senior author utilizes approximately 1 cm of distal penile shaft skin). The skin of the penis is elevated from the underlying corporal bodies (corpora cavernosa and spongiosa). On the dorsal aspect of the penis, care is taken to preserve the dorsal neurovascular bundle, which will be the neurovascular basis of the neoclitoris. A bilateral orchiectomy, including the spermatic cords, is performed at the level of the external inguinal ring. This allows the spermatic cords to retract within the inguinal canal and prevents a palpable bulge in the groin area ( Fig. 14.2.5 ).

Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here