Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

Access video content for this chapter online at Elsevier eBooks+ 
Gender-affirming genital surgery involves a complex series of staged procedures requiring a multidisciplinary approach with numerous other healthcare providers. Due to the irreversible nature of surgery, the World Professional Association for Transgender Health (WPATH) has published guidelines within the Standards of Care (SOC) to assist healthcare teams in identifying appropriate surgical candidates. The recommended criteria were not developed as a barrier but rather a set of guidelines designed to help provide care.
The mental health professional is an essential component in the evaluation and treatment of patients with gender dysphoria. The WPATH SOC recommends two formal referral letters from mental health professionals before undergoing genital gender affirmation surgery. The assessment may be done by the patient’s therapist or psychiatrist or another mental health provider to ensure that any associated mental health issues are well controlled. The length of time required for a patient to live in a gender role congruent with the gender identity ensures opportunity for patients to experience and adjust socially to their desired gender role before undergoing surgery.
WPATH SOC recommends a typical minimum of 1 year of hormone treatment before genital gender affirmation surgery. The overall goal for hormone therapy for a transmasculine person is to raise the circulating blood testosterone concentration to a male range of 300–1000 ng/dL. Patients will note pronounced changes in secondary sex characteristics including increases in facial and body hair, muscle mass, male pattern baldness, clitoral enlargement, and deepening of the voice. Potential adverse side effects include polycythemia vera, abnormal lipid profiles, and osteoporosis. While hormone therapy may be valuable in modifying the external physical appearance to better align with an individual’s gender identity, it is important to emphasize that hormone therapy also plays a crucial preoperative role in physically preparing individuals for genital gender affirmation surgery as it results in clitoral and labial hypertrophy which ultimately aids in perineal masculinization procedures. While there are no known specific testosterone-associated surgical complications, supraphysiologic or nonstandard hormone regimens may require perioperative assessment by an endocrinologist. Otherwise, there is no need for trans men to alter their hormone regimens in the perioperative period.
An in-person preoperative surgical consultation is required. During this visit, it is the authors’ strong belief that surgical options and surgical stages be thoroughly reviewed with the patient. The transgender community encompasses a wide spectrum of goals for seeking gender affirmation surgery. Patients experiencing gender dysphoria may have specific issues they wish to address surgically without wanting to take on additional surgical risk for procedures involving other areas. The surgeon should understand the patient’s individual expectations as unrealistic expectations are likely to lead to disappointment in final postoperative results. Preoperative optimization for certain conditions, especially obesity and smoking, should be addressed preoperatively to minimize risk for complications including delayed healing and partial flap necrosis. BMI greater than 35 is a relative contraindication due to increased distance to recipient structures and donor site thickness.
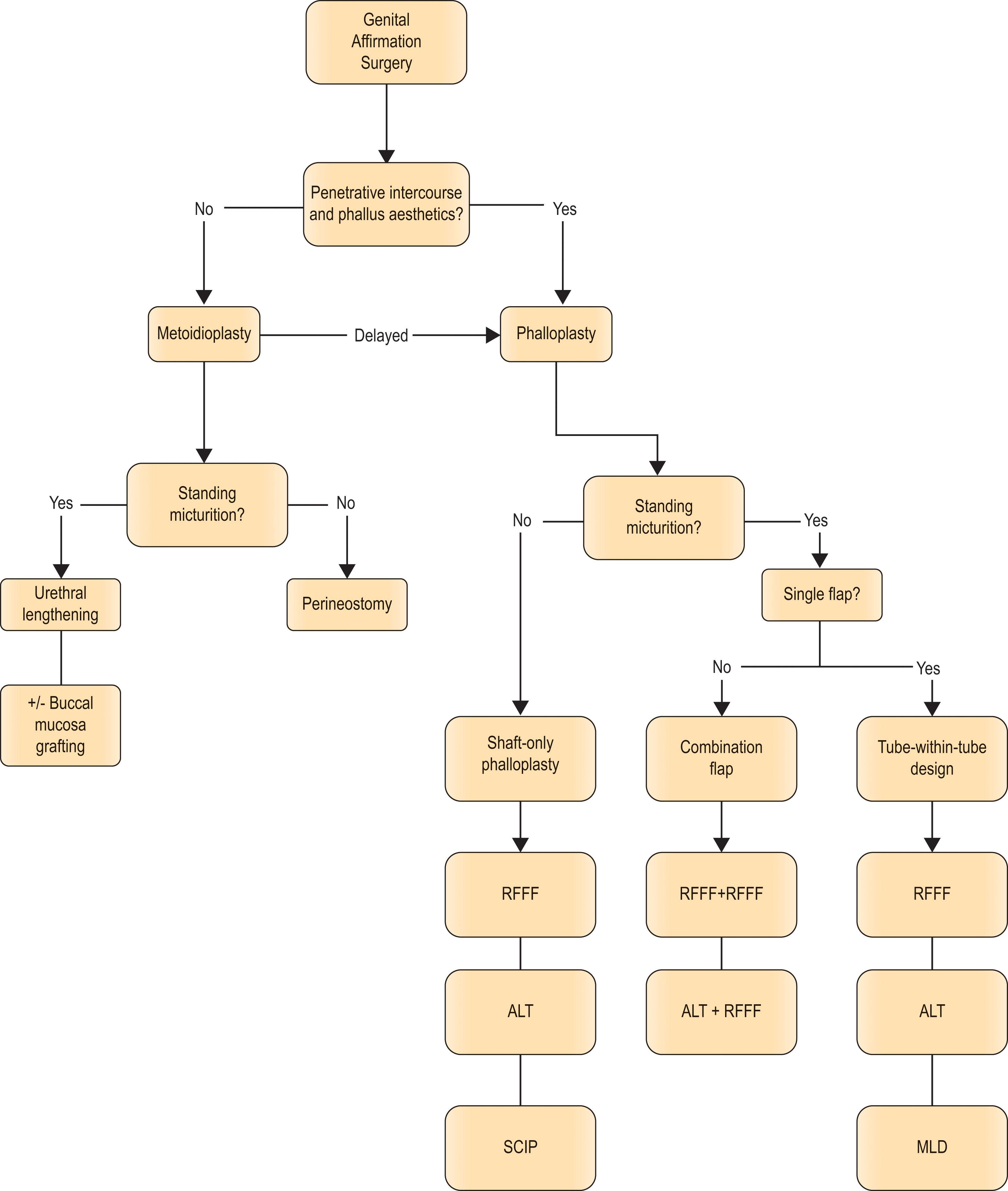
The authors strongly advocate for a comprehensive understanding of three key patient goals, including desire for standing micturition, penetrative intercourse, and overall neophallus aesthetics, broadly based off Moinstrey and colleagues’ ideal phallic reconstruction goals.
We believe it is imperative to understand a patient’s stance on these topics, as they represent essential branch points in the decision-making process for surgical plan and ultimate donor site selection ( Algorithm 14.3.1 ). For patients for whom penetrative intercourse and larger neophallus aesthetics are not of priority, a metoidioplasty may be an excellent option for achieving reconstructive goals while minimizing surgical risk. For patients who wish to forgo urination from the tip of the neophallus, reconstruction of a shaft-only phallus can be created to reduce risk for urologic complications.
In this situation, the urethra can either be left in its native position or lengthened to the base of the phallus using labia minora tissue. This type of reconstruction would allow later secondary urethroplasty should the patient desire this as part of their transition. If left in the native position, the patient can still decide if they desire scrotoplasty and/or vaginectomy. If a vaginectomy and perineoplasty is performed, then the urethra is externalized as a perineal urostomy.
For patients who wish to stand to urinate and wish to have penetrative intercourse and proportionate phallic length, a tube in tube design is recommended. Most surgeons will recommend a vaginectomy whenever the urethra is lengthened to be able to cover the urethroplasty with various vascularized layers with a significant decrease in complications.
Modern phalloplasty approaches have evolved from a long lineage of techniques originally centered on reconstruction of congenital and traumatic penile defects. Russian surgeon Nicolaj Bogoras first reported neophallus reconstruction in 1936 utilizing a pedicled abdominally based flap for reconstruction of a penile amputation. In the early 1970s, Orticochea introduced a myocutaneous gracilis flap reconstruction. In the 1980s, with the advent of microsurgery and free tissue transfer, Chang and Hwan introduced the tube-within-a-tube design.
In the context of gender affirmation surgery, phalloplasty broadly involves the creation of a neophallus using a flap from a donor site ( , , , , , ). The phalloplasty can be designed and constructed from single or multiple donor sites (in cases where a composite flap is desired for separate urethra and shaft portions). Surgery can be performed in a single-stage fashion, where perineal masculinization is performed at the same time as flap creation, or staged in 2–3 operations spaced several months apart to separate steps in tissue transfer and/or perineal masculinization. The length of hospitalization for these stages can range from 1 day to 1 week or more. There are pros and cons to each approach, which will largely depend on patient preference and surgeon experience ( Table 14.3.1 ). While numerous donor sites have been described including superficial circumflex iliac artery perforator, latissimus dorsi, and free fibula, the most frequently used donor sites in the United States are the forearm and the anterolateral thigh (ALT).
| Staging sequence | Pros | Cons | |
|---|---|---|---|
| Single stage | Stage 1: perineal masculinization and tube in tube phalloplasty | Single surgery. | Longer anesthesia time, concern for cumulative complication risk from multiple concurrent procedures. |
| Metoidioplasty first |
|
|
Additional staged surgeries. Flap complications may impact patients’ ability to urinate. |
| “Big Ben method” (Dr. Christopher Nim and Dr. David Ralph in London) |
|
|
|
Regardless of phalloplasty donor site choice, patients desiring postoperative standing micturition require urethral lengthening to create a conduit from the native urethra to the tip of the reconstructed neophallus. The pars fixa refers to the non-mobile portion of the neourethra created during perineal masculinization by closure of the embryonic urethral plate in a tubelike fashion. This is in contrast to the pars pendulans which refers to the pendulous portion of the neourethra traversing the neophallus reconstruction.
One of the most crucial steps in pars fixa urethral reconstruction is vaginectomy. The distal vaginal mucosa is often excised directly, or in some cases, the anterior vaginal mucosa may be recruited as local tissue flaps for additional urethral lengthening. Due to the risk for bowel injury, it is preferable to ablate the proximal vagina using electrocautery. After removal of the vaginal mucosa, the remaining vaginal vault is typically sutured closed upon itself to obliterate dead space. Deep sutures should be placed with care to avoid damage to the underlying rectum. Careful tissue handling permits use of bulbospongiosus muscle and fascial tissue for additional coverage over the urethral suture line.
After completion of vaginectomy, we proceed with urethral lengthening and reconstruction of the pars fixa. The pars fixa urethra is the fixed segment of urethra that extends from the native urethral meatus to the clitoral head. This technique is the same for both radial forearm and ALT phalloplasty procedures. Generally speaking, local tissue is recruited for tube formation, often utilizing hairless labia minora tissue. Patients with less robust tissue response to testosterone hormone therapy may also require further recruitment of perivaginal introitus tissue. For patients with deficient minora tissue distally, an epidermal autograft from excess minora or vaginal epithelium may be used.
In our experience, we find it essential to excise a triangular portion of mucosa surrounding the periurethral fornices ( Fig. 14.3.1 ). This results in two main benefits: it eliminates blind pouches within the urethral lengthening which facilitates future Foley insertions, and also serves to decrease urinary stasis which may lead to debris accumulation. Labia minora flaps are elevated in a submucosal plane from distal to proximal. If additional urethral lengthening is required, an additional 1–2 cm may be gained by utilizing the ventral clitoral epithelium by de-epithelializing the lateral edges of the clitoris and tubularizing this structure.

The pars fixa is then formed from the labia minora flaps tubed around the native urethra. The medial labial flaps are closed in two layers to form the deep surface of the neourethra. The lateral flap edges are then sewn together in layers to form the superficial surface of the neourethra ( Fig. 14.3.2 ).
 Dissection of labia minora flaps. (B) Tubularization and closure. (C) Completed tubularization over urinary catheter.")
This neourethra is further reinforced with layers of local tissue flaps. Labia minora skin flaps are created and inset over the origin of the pars fixa in a “pants-over-vest” fashion to provide vascularized tissue coverage at the vulnerable takeoff of the urethral lengthening suture line. The central and distal parts of pars fixa are covered with bulbospongiosus myofascial flaps.
The clitoris is de-epithelialized, and a dorsal clitoral nerve is tagged for future coaptation. A midline position is marked for transposition of the urethral lengthening segment and clitoris via a subcutaneous tunnel. A Coudé catheter is passed to verify a facile pathway through the urethral lengthening without blind-ending pouches. This is left in place to facilitate eventual urethral anastomosis ( Fig. 14.3.3 ).

Scrotoplasty is completed with labia majora fasciocutaneous flaps. The flaps are trimmed to size and sutured upon themselves in a layered closure with absorbable sutures ( Fig. 14.3.4 ).
 After dissection of labial flaps. (B) After perineal closure and scrotoplasty closure.")
At this point, the phalloplasty flap is transposed to the pubic mons, and the required urethral anastomosis, nerve coaptation, and vascular anastomoses (if applicable) are completed.
Over time, the radial forearm flap has been found to be functional, safe, and reliable, with the highest reported rates of survival and functional urinary conduit among the most commonly performed free flap phalloplasty procedures. Advantages include a reliable and predictable vascular pedicle, relatively thin supple flap thickness helpful for facilitating a double tube design, innervation density for neurotization, and robust vascularity to allow for glansplasty. The main disadvantage is the conspicuous donor site and possible need for hand therapy to regain preoperative range of motion and strength.
The flap is typically harvested from the nondominant forearm. A standard Allen’s test confirms the presence of an intact palmar arch. Of particular note, in patients with abnormal Allen’s test results, routine interventional radiology angiogram fails to demonstrate adequacy of compensatory blood flow if radial artery occlusion maneuvers are not performed. In these situations, even with a diminutive or incomplete arch on angiogram, we recommend proper patient counseling for an intra-operative test to clamp the radial artery via a distal wrist cut down; if the hand regains adequate perfusion despite radial artery clamping, then surgery may proceed with radial forearm harvest. Persistently abnormal perfusion may necessitate ALT phalloplasty harvest.
During preoperative flap design, attention is closely paid to the flap thickness as determined by pinch testing, as this determines whether double tube reconstruction and glansplasty are feasible at the time of initial reconstruction. If the flap is deemed too thin – less than 0.5 cm with pinch testing – then glansplasty is not offered at the time of initial phalloplasty because of increased risk of inadequate blood supply to the distal glans after coronaplasty. Due to the full-thickness skin flaps required for coronaplasty, the subdermal plexus is no longer available to provide blood flow to the distal glans. There is no strict upper limit to flap thickness that precludes reconstruction in our experience. However, thickness quadruples with double tubing ( Fig. 14.3.5 ), requiring additional skin for increased flap circumference, thus creating a larger donor defect. Furthermore, increased flap bulk inherently creates more cumulative flap edema postoperatively, which threatens flap viability. The typical optimal pinch test thickness ranges from 0.75 cm to 1.5 cm.

During preoperative evaluation, note is also made of the level of hair-bearing skin. Hair removal, typically via laser or electrolysis, must be completed far ahead of surgery and decreases the risk of urethral stone formation and post-void drip that occurs with the presence of large amounts of urethral hair. Fortunately, small amounts of hair are frequently asymptomatic. Patients must be counseled regarding the impact of flap elevation on existing tattoos, which in many instances may be noticeable on the external phalloplasty. If desired, tattoo removal may be completed preoperatively or postoperatively on the phalloplasty after sufficient healing, prior to nerve regeneration and sensory return.
The double tubed radial forearm phalloplasty flap is designed along the radial artery and just proximal to the wrist crease ( Fig. 14.3.6 ). Although it is tempting to harvest the most distal wrist tissue for maximum phallus length, note that placement of the flap too distally impairs wrist extension postoperatively and creates completely avoidable morbidity. The radial and dorsal flaps serve as the external surface, while internalization of the ulnar portion forms the pars pendulans urethra. When determining the maximum length of the neophallus, consideration must be given to the length of flap pedicle required from the bifurcation of the brachial artery, which is estimated using the distance from the femoral vessels to the pubic mons. In terms of flap width, the skin paddle must be wide enough to permit tensionless closure during tubing. There is no simple, specific formula used to calculate the width of the flap. Mathematically, the external flap skin should be 4pi*thickness. However, this calculation does not incorporate unaccounted, unpredictable variables of varying skin elasticity, subcutaneous tissue compressibility, and postoperative edema. As a simple rule of thumb, if the remaining forearm skin is able to be pinched together, then a sufficient amount of skin will be harvested with the flap. After determining the flap length and width, the remaining landmarks are determined. Just ulnar to the flexor carpi radialis tendon, a 1 cm strip is marked for de-epithelialization between the external and internal portions, which critically serves as the vascular bridge between the outer and inner tubes. The proximal neourethra is designed either as a “house” or “tail” depending on the anticipated length gained with urethral lengthening, based on the soft-tissue response to testosterone. Both designs allow for obliquely oriented urethral anastomosis. The urethral strip is typically 4 cm in width distally and can be widened proximally. When tubed, this design allows for comfortable passage of a 16 F Foley catheter. Our group additionally harvests an adipofascial flap at the proximal urethral segment beyond the borders of the neourethra ( Fig. 14.3.7 ). This provides vascularized soft-tissue coverage circumferentially around the proximal neourethra and urethral anastomosis between the distal pars fixa and proximal pars pendulans urethra as discussed later in the chapter. Proximally, zigzag incisions extend from the proximal flap markings to the antecubital crease for pedicle exposure
 Ulnar volar forearm forms urethral segment abutted by a 1cm strip of de-epithelialized flap to facilitate rolling (hatch-marked). Anticipated course of radial artery (red) and cephalic vein (blue). (B) Dorsal forearm forms shaft segment.")
 Note inclusion of additional outflow vein corresponding to urethral component of flap (red arrow) in addition to additional perfused proximal adipofascial tissue to reinforce eventual urethral anastomosis (blue arrow). (B) The radial forearm phalloplasty most reliably yields a thin and pliable flap.")
The radial forearm flap is raised in typical fashion under tourniquet control with additional attention to several notable nuances ( Fig. 14.3.8 ). The de-epithelialized skin strip is carefully harvested as thinly as possible in order to maximize preservation of the subdermal plexus for perfusion of the neourethra. The skin graft is spared for use with glansplasty later on. The urethral adipofascial flap is elevated at the proximal edge of the urethral portion. The forearm skin is elevated off of the flap in a subdermal plane for 1–2 cm beyond the border of the urethra. Later on, this provides vascular soft-tissue coverage around the distal urethral lengthening and urethral anastomosis. The cephalic vein is harvested and traced proximally until it joins with the deep venous system via the profunda cubitalis (deep cubital vein), thus combining the superficial venous drainage with the radial artery venae comitantes ( Fig. 14.3.9 ). If present, we spare the largest caliber superficial vein leading to the urethral segment (see Fig. 14.3.7 ) and use this as a second venous anastomosis, ideally preventing venous congestion in the pars pendulans urethra. The lateral antebrachial cutaneous nerve is harvested with the flap to provide sensation to the external neophallus. Smaller branches to the medial antebrachial cutaneous nerve may run along the ulnar flap and are optional but may be used as well. The superficial branch of the radial nerve is preserved and left in situ in the forearm; however, to avoid inadvertent thinning of the flap, the nerve is elevated with the flap and subsequently freed from the flap ( Fig. 14.3.10 ). Palmaris longus tendon is often harvested up with the flap if it is in proximity to the pedicle or venous plexus; otherwise it may be spared. The radial artery and venae are traced proximally until the bifurcation of the brachial artery or until enough pedicle length has been elevated. In the rare instances where the radial artery pedicle is too short for midline positioning of the phallus, vein grafting may be required.
 Volar forearm with subfascial dissection radial to flexor carpi radialis (FCR). (B) Extended dorsal forearm dissection for shaft coverage.")
 to combine the superficial venous drainage with the radial artery venae comitantes to maximize venous outflow.")
.")
After tourniquet deflation, the flap is then double tubed. The pars pendulans is tubed by joining the ulnar flap edge with the ulnar de-epithelialized strip edge, utilizing a two-layer closure with absorbable suture. Particular attention is given to shallow longitudinal bites along the dermal portion to prevent disruption of the subdermal plexus. A water leak test may be tempting, but too many additional sutures may secondarily compromise vascularity to the urethra. The external flap is then wrapped around the pars pendulans. The radial flap edge is then sutured to the radial de-epithelialized strip edge in two layers with absorbable suture, again taking shallow bites through the de-epithelialized portion. The external epidermis is closed with a running absorbable suture. Thus the pars pendulans is enveloped completely with the vascularized forearm flap, with staggered suture lines that decrease the risk of urinary fistula ( Fig. 14.3.11 ).
 Native flap. (B,C) Tubing of urethra. (D) Subsequent closure of shaft.")
At the distal flap, the urethral tube and external tube are sutured together with interrupted monocryl. The coronal ridge is then marked using a 1 cm wide skin flap, based 3 cm from the glans tip, at a point on the dorsum opposite the external suture line. Moving ventrally, the markings gently curve distally and taper together to join at the ventral surface. The coronal ridge is then incised proximally and raised sharply as a full-thickness flap in a subdermal plane up to the distal marking. Absorbable sutures are then used to shape the coronal ridge circumferentially ( Fig. 14.3.12 ). The skin graft is then placed over the denuded subcutaneous tissue proximal to the coronal ridge, taking care to not overly tighten the graft and constrict the glans. At this point, the phalloplasty is left in situ until ready for flap division.
 Glansplasty design. (B) Full-thickness flap elevation in a subdermal plane to create coronal ridge. (C) Coronal ridge shaping sutures. (D) Skin grafting of residual defect using prior skin harvested from radial forearm flap harvest.")
In our practice, the groin contralateral to the free flap is typically used, as this minimizes the required pedicle length to the recipient vessels. However, the deep inferior epigastric system is also a commonly described recipient vessel site which provides similar caliber vessels. An incision is made from the femoral vessels toward the recipient site overlying the pubic symphysis and along the groin crease. The superficial femoral artery is prepared for end-to-side anastomosis. The greater saphenous vein is prepared for end-to-end anastomosis ( Fig. 14.3.13 ). If a urethral vein is available in the flap, additional smaller saphenous branches are prepared as well. At this point, the patient undergoes pars fixa and pars pendulans anastomosis.
 An extension is made laterally toward groin vessels. (B) Exposure of superficial femoral artery and saphenous vein.")
The forearm is typically closed by the harvesting team during urethral anastomosis. In preparation for skin grafting, the large gap between the brachioradialis–flexor carpi radialis (BR-FCR) interval must be reapproximated, and the FCR tendon must be protected. Absorbable suture is used to close the BR-FCR interval proximally and to cover the distal FCR tendon by imbricating the surrounding flexor pollicis longus (FPL) musculature ( Fig. 14.3.14 ). A split-thickness skin graft sheet from the thigh is inset over the forearm. The skin graft is bolstered using a negative pressure dressing, and a volar splint is fabricated. In thin patients, the skin graft contour blends well and may be camouflaged with tattooing after complete healing.
 Distal FCR tendon is covered with imbrication of adjacent FPL muscle belly. (B) Split-thickness sheet graft from thigh is inset. (C) Late postoperative result of forearm healing.")
Become a Clinical Tree membership for Full access and enjoy Unlimited articles
If you are a member. Log in here